You might also like
- Bottom Surgery: What You Need To KnowDocument4 pagesBottom Surgery: What You Need To KnowBook ReaderNo ratings yet
- Abstracts BookDocument186 pagesAbstracts BookGabriel Laurentiu CucuNo ratings yet
- Sex ChangeDocument41 pagesSex Changeiura echin67% (3)
- Vaginal tightening techniqueDocument5 pagesVaginal tightening techniquejuan carlos pradaNo ratings yet
- Total Colpocleisis Technique ManuscriptDocument5 pagesTotal Colpocleisis Technique ManuscriptvasasdfwqeNo ratings yet
- Video Presentations: Vaginal Salpingo-Oophorectomy: Tips and TricksDocument2 pagesVideo Presentations: Vaginal Salpingo-Oophorectomy: Tips and Tricksmohamad safiiNo ratings yet
- Sex ModifyDocument41 pagesSex Modifyshyam rana100% (1)
- Tunica Vaginalis Flap Reinforcement in Staged Hypospadias RepairDocument11 pagesTunica Vaginalis Flap Reinforcement in Staged Hypospadias RepairDrMadhu AdusumilliNo ratings yet
- Gynecological Aspectsof Transgender Healthcare 2009Document10 pagesGynecological Aspectsof Transgender Healthcare 2009Iris LopezNo ratings yet
- Metoidioplasty ArticleDocument5 pagesMetoidioplasty ArticlemalakyKBNo ratings yet
- Bioethics MutilationDocument26 pagesBioethics MutilationErl Driz100% (1)
- Preecha's Technique MtF. (The Pioneer in Sex Reassignment Surgery, Thailand) - 1Document7 pagesPreecha's Technique MtF. (The Pioneer in Sex Reassignment Surgery, Thailand) - 1VeroniqueNo ratings yet
- Transvaginal MorcellationDocument8 pagesTransvaginal Morcellationsanjayb1976gmailcomNo ratings yet
- Algoritmo Mama Trans MasculinaDocument11 pagesAlgoritmo Mama Trans MasculinaDr Felipe GoisNo ratings yet
- Complicationsoflapmyomectomy ANZ 2010Document7 pagesComplicationsoflapmyomectomy ANZ 2010Nadila 01No ratings yet
- Jms 50 061 Chandrashekar OutcomeDocument6 pagesJms 50 061 Chandrashekar OutcomeAripinSyarifudinNo ratings yet
- Proximal Hypospadias Repair With Bladder Mucosal Graft: Our 10 Years ExperienceDocument6 pagesProximal Hypospadias Repair With Bladder Mucosal Graft: Our 10 Years ExperienceLastri HillaryNo ratings yet
- Jandrol 112 016444Document7 pagesJandrol 112 016444Павел ГичакNo ratings yet
- Hysterectomy and Sexuality: Ester Illiano, Konstantinos Giannitsas, Elisabetta CostantiniDocument13 pagesHysterectomy and Sexuality: Ester Illiano, Konstantinos Giannitsas, Elisabetta CostantiniSaNta YoNo ratings yet
- Degloving InjuryDocument4 pagesDegloving InjuryWisdananingrumNo ratings yet
- Robotic Hernia Surgery: A Comprehensive Illustrated GuideFrom EverandRobotic Hernia Surgery: A Comprehensive Illustrated GuideOmar Yusef KudsiNo ratings yet
- Current Concepts of UrethroplastyDocument226 pagesCurrent Concepts of Urethroplastywasis0% (1)
- A New Practical Surgical Technique ForDocument5 pagesA New Practical Surgical Technique Forsualehasabiqa111No ratings yet
- Urethroplasty For Long Anterior Urethral Strictures: Report of Long-Term ResultsDocument5 pagesUrethroplasty For Long Anterior Urethral Strictures: Report of Long-Term ResultsAnonymous z0QfbwY3d8No ratings yet
- A New Facilitating Technique For Postpartum Hysterectomy at Full Dilatation: Cervical ClampDocument4 pagesA New Facilitating Technique For Postpartum Hysterectomy at Full Dilatation: Cervical ClampJani SheNo ratings yet
- Journal 2015Document3 pagesJournal 2015Rakha Sulthan SalimNo ratings yet
- Surgical Uterus Gynecologist Fundus Cervix: Types of HysterectomyDocument3 pagesSurgical Uterus Gynecologist Fundus Cervix: Types of HysterectomyMary Ann LunnayNo ratings yet
- The Bilateral Pedicled Epilated Scrotal Flap: A Powerful Adjunctive For Creation of More Neovaginal Depth in Penile Inversion VaginoplastyDocument8 pagesThe Bilateral Pedicled Epilated Scrotal Flap: A Powerful Adjunctive For Creation of More Neovaginal Depth in Penile Inversion VaginoplastySexologia Del OesteNo ratings yet
- Best Practice & Research Clinical Obstetrics and GynaecologyDocument17 pagesBest Practice & Research Clinical Obstetrics and Gynaecologymusyawarah melalaNo ratings yet
- Treatment For Failed Epispadias Repair Presenting in AdultsDocument6 pagesTreatment For Failed Epispadias Repair Presenting in AdultsDhonz R AdiwaramanNo ratings yet
- Kulkarni 2016 PDFDocument21 pagesKulkarni 2016 PDFquirinalNo ratings yet
- Pi Is 0002937814024491Document1 pagePi Is 0002937814024491Althaf FathanNo ratings yet
- 10.1089lap.2016.0031Document5 pages10.1089lap.2016.0031dw21541No ratings yet
- Keys to Successful Orthotopic Bladder SubstitutionFrom EverandKeys to Successful Orthotopic Bladder SubstitutionUrs E. StuderNo ratings yet
- Ve Sico Vaginal FistulasDocument7 pagesVe Sico Vaginal FistulasSubhan Arif RahmanNo ratings yet
- Tau 06 03 510Document7 pagesTau 06 03 510Eko NoviantiNo ratings yet
- Gynecology: Three Minimally Invasive Procedures You Need to Know About For: Permanent Birth Control, Heavy Menstrual Periods, Accidental Loss of Urine Plus: Modern Hormone Therapy for the Post Menopausal WomenFrom EverandGynecology: Three Minimally Invasive Procedures You Need to Know About For: Permanent Birth Control, Heavy Menstrual Periods, Accidental Loss of Urine Plus: Modern Hormone Therapy for the Post Menopausal WomenNo ratings yet
- Laparoscopic Myomectomy in Patients With Uterine Myomas Associated With InfertilityDocument9 pagesLaparoscopic Myomectomy in Patients With Uterine Myomas Associated With Infertilitysanta_pangaribuan_1No ratings yet
- Current Concepts in Plastic Surgery - AgulloDocument273 pagesCurrent Concepts in Plastic Surgery - AgulloAnonymous LnWIBo1GNo ratings yet
- Penis Reconstruction for Trapped Penis with Chordae and Subglanular HypospadiaDocument6 pagesPenis Reconstruction for Trapped Penis with Chordae and Subglanular HypospadiamariaNo ratings yet
- 3 PBDocument6 pages3 PBAulia Rizqi MulyaniNo ratings yet
- Vaginal Agenesis or HypoplasiaDocument18 pagesVaginal Agenesis or Hypoplasianikd_6No ratings yet
- Vaginal Cuff 2Document5 pagesVaginal Cuff 2Aulia Rizqi MulyaniNo ratings yet
- Post Aua ReconstructivaDocument14 pagesPost Aua ReconstructivaIndhira Sierra SanchezNo ratings yet
- Laparoscopic Simple Prostatectomy With Prostatic Urethra Preservation For Benign Prostatic HyperplasiaDocument5 pagesLaparoscopic Simple Prostatectomy With Prostatic Urethra Preservation For Benign Prostatic Hyperplasiajuan jose velascoNo ratings yet
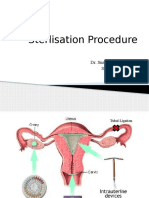
- Sterlisation Procedure: Dr. Sushruta Shrivastava SR Dept of OBGY AIIMS, BhopalDocument30 pagesSterlisation Procedure: Dr. Sushruta Shrivastava SR Dept of OBGY AIIMS, BhopalsushrutaNo ratings yet
- TOG Vaginal HysterectomyDocument6 pagesTOG Vaginal HysterectomyYasmin AlkhatibNo ratings yet
- Sili Kono MaDocument4 pagesSili Kono MaDella Rahmaniar AmelindaNo ratings yet
- Project Format KTU 2Document98 pagesProject Format KTU 2vivek jaiswalNo ratings yet
- One-Step Urethroplasty in Recurrent Chordee On Scrotal HipospadiaDocument5 pagesOne-Step Urethroplasty in Recurrent Chordee On Scrotal HipospadiaWahyu KurniawanNo ratings yet
- International Journal of Gynecology and Obstetrics: Adolf Lukanovi Č, Katarina Dra ŽičDocument4 pagesInternational Journal of Gynecology and Obstetrics: Adolf Lukanovi Č, Katarina Dra ŽičkevindjuandaNo ratings yet
- Vaginal Reconstruction With Pudendal Thigh Flap-An Early Experience in Shaheed Sohrawardi Medical College HospitalDocument7 pagesVaginal Reconstruction With Pudendal Thigh Flap-An Early Experience in Shaheed Sohrawardi Medical College HospitalisabelNo ratings yet
- Bariatric Robotic Surgery: A Comprehensive GuideFrom EverandBariatric Robotic Surgery: A Comprehensive GuideCarlos Eduardo DomeneNo ratings yet
- Case Report: Vaginal Myomectomy For A Thirteen-Centimeter Anterior MyomaDocument4 pagesCase Report: Vaginal Myomectomy For A Thirteen-Centimeter Anterior MyomaAna Di JayaNo ratings yet
- Hamlet Reinaissance Ideas, The World and Death PDFDocument2 pagesHamlet Reinaissance Ideas, The World and Death PDFCarlos Rodríguez RuedaNo ratings yet
- UGRA 2017 Guide2010Document46 pagesUGRA 2017 Guide2010avgNo ratings yet
- ML EnterprisesDocument10 pagesML EnterprisesKirpal Trading companyNo ratings yet
- Cute Crochet Cat With Heart Amigurumi PDF PatternDocument5 pagesCute Crochet Cat With Heart Amigurumi PDF PatternJustyna Janicka100% (4)
- Role Autonomic NervousDocument18 pagesRole Autonomic Nervoustassiana99No ratings yet
- Kami Export - The Call of The Wild PDFDocument10 pagesKami Export - The Call of The Wild PDFursjinalNo ratings yet
- A Lesson For The TigerDocument8 pagesA Lesson For The TigerBestka ZaushaNo ratings yet
- Biology Test Chapter 1,2,3Document2 pagesBiology Test Chapter 1,2,3Abdul GhaffarNo ratings yet
- General Orientation To Human Anatomy: Atlas ADocument33 pagesGeneral Orientation To Human Anatomy: Atlas AEmilie ArvidsonNo ratings yet
- Barium Swallow (Esophagram) :: Positions and Barium Images PurposeDocument3 pagesBarium Swallow (Esophagram) :: Positions and Barium Images PurposeAaron SmithNo ratings yet
- Basic Obstetrics For The Midwifery Board ExaminationDocument3 pagesBasic Obstetrics For The Midwifery Board ExaminationJoshua Diao93% (14)
- The Eighteenth Century PDFDocument65 pagesThe Eighteenth Century PDFAlexei Ada100% (2)
- Call of Cthulhu - The Arkham Gazette #3 (7E Conversion)Document20 pagesCall of Cthulhu - The Arkham Gazette #3 (7E Conversion)tommy fletcher100% (2)
- English Year 2 Paper 1 Miss ReenDocument13 pagesEnglish Year 2 Paper 1 Miss ReenNurul AinNo ratings yet
- EVS Model Paper Mar 2023Document4 pagesEVS Model Paper Mar 2023Haseena V K K MNo ratings yet
- Clasificacion Fisuras LPHDocument72 pagesClasificacion Fisuras LPHkarenNo ratings yet
- SBA4Document81 pagesSBA4Jenny TaylorNo ratings yet
- Omelet: A Tragedy of Bill Shake-A-SpeareDocument138 pagesOmelet: A Tragedy of Bill Shake-A-Speareedwrite5470No ratings yet
- 11sta MariaDocument85 pages11sta MariaDASURECOWebTeamNo ratings yet
- The Satanic PhallusDocument12 pagesThe Satanic PhallusDAVIDNSBENNETTNo ratings yet
- Pap SmearDocument10 pagesPap SmearEunice Jade Claravall ArgonzaNo ratings yet
- Furuncle and Carbuncle FootDocument0 pagesFuruncle and Carbuncle Footrasputin22100% (1)
- CD Part 2 - Communicable Diseases With Pics (1) ConDocument239 pagesCD Part 2 - Communicable Diseases With Pics (1) ConMackoi SalamanesNo ratings yet
- Subjectobject Pronounspossessive AdjectivesDocument1 pageSubjectobject Pronounspossessive AdjectivesDana Danutza100% (1)
- Araling Panlipunan 3Document3 pagesAraling Panlipunan 3HAZEL JANE BAGUIONo ratings yet
- 16 Preovulatory Stasis Dystocia in Oviparous Lizards PDFDocument4 pages16 Preovulatory Stasis Dystocia in Oviparous Lizards PDFRizza SainTrow VeiroNo ratings yet
- Latihan Sains Tingkatan 3 Bab 4Document11 pagesLatihan Sains Tingkatan 3 Bab 4李友志67% (3)
- Agent Causation and Agential ControlDocument309 pagesAgent Causation and Agential Controlorj78No ratings yet
- Rusty MonitorDocument2 pagesRusty MonitorVeteran Tree Group AustraliaNo ratings yet
- LDC Model Questions Part 4Document13 pagesLDC Model Questions Part 4AdwaithNo ratings yet