You might also like
- Complete Medical Guide for Disease Volume VII; Atopic DermatitisFrom EverandComplete Medical Guide for Disease Volume VII; Atopic DermatitisNo ratings yet
- Ebook PDF Current Medical Diagnosis and Treatment Study Guide 2nd PDFDocument41 pagesEbook PDF Current Medical Diagnosis and Treatment Study Guide 2nd PDFcecil.slocum194100% (41)
- Eczema and Nummular Dermatitis GuideDocument91 pagesEczema and Nummular Dermatitis GuideJhost Clinton PurbaNo ratings yet
- EczemaDocument34 pagesEczemaPratzNo ratings yet
- Olga's Dermatoligy PresentationDocument61 pagesOlga's Dermatoligy PresentationHerdy PerdanaNo ratings yet
- Dermatitis: Department of Dermato Venereology Faculty of Medicine Gadjah Mada UniversityDocument30 pagesDermatitis: Department of Dermato Venereology Faculty of Medicine Gadjah Mada UniversityMuhammad mukramNo ratings yet
- Skin Block: - Introduction To Diseases of The Skin - Acneiform, Alopecias, and Pigmentary DisordersDocument60 pagesSkin Block: - Introduction To Diseases of The Skin - Acneiform, Alopecias, and Pigmentary DisordershemihemaNo ratings yet
- Dr. R. Sekhon - Dermatology Telehealth Jan 27 MRDocument45 pagesDr. R. Sekhon - Dermatology Telehealth Jan 27 MRAnissa ADNo ratings yet
- LCD Kuliah Dermatitis Wa2008Document32 pagesLCD Kuliah Dermatitis Wa2008Made Wardhana100% (2)
- Adebola Ogunbiyi, FMCP, FWACP, FRCP, FNAMED UCH, IbadanDocument63 pagesAdebola Ogunbiyi, FMCP, FWACP, FRCP, FNAMED UCH, Ibadanadamu mohammadNo ratings yet
- Overview Common Dermatologic Problems in ChildrenDocument26 pagesOverview Common Dermatologic Problems in Childrenokwadha simionNo ratings yet
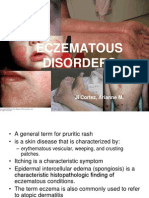
- Eczematous Disorders CFM REPORT 2Document32 pagesEczematous Disorders CFM REPORT 2Arianne CortezNo ratings yet
- Dermatology in 2hrsDocument222 pagesDermatology in 2hrslarisaP100% (4)
- Atopic Eczema 2Document27 pagesAtopic Eczema 2Pierre-Charles WoodNo ratings yet
- Treating Atopic Dermatitis in Children Under 40 CharactersDocument26 pagesTreating Atopic Dermatitis in Children Under 40 CharactersAnnisa SasaNo ratings yet
- 6435 SOAP NOTE Presentation Atopic DermatitisDocument21 pages6435 SOAP NOTE Presentation Atopic DermatitisMelinda Powell100% (2)
- Pedia AdDocument14 pagesPedia AdKc GarciaNo ratings yet
- Derma ADDocument49 pagesDerma ADFatima Marwa Teo MaghinayNo ratings yet
- HANDOUT 3Y Inflammatory Dermatoses 5-28-2012Document23 pagesHANDOUT 3Y Inflammatory Dermatoses 5-28-2012Monica ArmonioNo ratings yet
- DermatitisDocument61 pagesDermatitisAlex XanderNo ratings yet
- Dermatology Primer: Selected Skin Diseases and Treatment Tailored For The Athletic TrainerDocument64 pagesDermatology Primer: Selected Skin Diseases and Treatment Tailored For The Athletic TrainerSilviu100% (1)
- Hypersensitivity and Immunological DisordersDocument32 pagesHypersensitivity and Immunological DisordersQashqar & GB FolksNo ratings yet
- Dermatology - LoveDocument433 pagesDermatology - LoveAntonio EscobarNo ratings yet
- Feline DermatologyDocument55 pagesFeline DermatologySilviuNo ratings yet
- KULKEL Atopic DermatitisDocument34 pagesKULKEL Atopic Dermatitisirhamni istiqomahNo ratings yet
- Atopic DermatitisDocument26 pagesAtopic DermatitissetiabudiNo ratings yet
- Approach To Patient With Allergic Diseases: Jovilia M. Abong, M.D. FPCP, Fpsaai, MSCDocument65 pagesApproach To Patient With Allergic Diseases: Jovilia M. Abong, M.D. FPCP, Fpsaai, MSCCristinaConcepcionNo ratings yet
- 2 EczemaDocument5 pages2 Eczemaحسين طاهر حاتم طاهرNo ratings yet
- Eczema and DermatitisDocument47 pagesEczema and DermatitisDeborah ChemutaiNo ratings yet
- Atopic Dermatitis: By:-Raj Gundaniya (11) Parth Chauhan (6) Group: - B1Document9 pagesAtopic Dermatitis: By:-Raj Gundaniya (11) Parth Chauhan (6) Group: - B1Shakti RathodNo ratings yet
- Dermatitis: Perioral Dermatitis, Numular Dermatitis, NeurodermatitisDocument25 pagesDermatitis: Perioral Dermatitis, Numular Dermatitis, NeurodermatitisNAOMI SINAGANo ratings yet
- Dermatology For The Small Animal PractitionerDocument145 pagesDermatology For The Small Animal Practitionerсветлана бугаева100% (5)
- Atopic Dermatitis (1 of 13) : Acute Flare Up TreatmentDocument12 pagesAtopic Dermatitis (1 of 13) : Acute Flare Up TreatmentDarlen RabanoNo ratings yet
- Dermatitis & Urticaria: Department of Dermato Venereology Faculty of Medicine Gadjah Mada UniversityDocument34 pagesDermatitis & Urticaria: Department of Dermato Venereology Faculty of Medicine Gadjah Mada UniversityadystiNo ratings yet
- Skin Disease: Roshana MallawaarachchiDocument51 pagesSkin Disease: Roshana MallawaarachchiRoshana Mallawaarachchi100% (1)
- Rash DecisionsDocument40 pagesRash DecisionsKURBULDKNo ratings yet
- Eczema and DermatitisDocument24 pagesEczema and Dermatitisjackofmanytrades100% (1)
- Atopic Dertmatitis: Micheal Felner MD, FaadDocument17 pagesAtopic Dertmatitis: Micheal Felner MD, Faadkhawar93No ratings yet
- Atopic Dermatitis PresentsiDocument17 pagesAtopic Dermatitis PresentsianniNo ratings yet
- JR DR Arif Dermatitis Atopi Kelompok 1Document46 pagesJR DR Arif Dermatitis Atopi Kelompok 1regina pingkanNo ratings yet
- 07.02.2020 Lupus ErythematosusDocument67 pages07.02.2020 Lupus ErythematosussujataNo ratings yet
- 5: Allergy and The Skin: Eczema and Chronic Urticaria: Mja Practice Essentials - AllergyDocument6 pages5: Allergy and The Skin: Eczema and Chronic Urticaria: Mja Practice Essentials - AllergyDavid PattersonNo ratings yet
- Atopic DermatitisDocument10 pagesAtopic DermatitistazzycaNo ratings yet
- BSC Amw3, Bvs3 Angela Bayfield 2010Document31 pagesBSC Amw3, Bvs3 Angela Bayfield 2010Laura Joanne SteadNo ratings yet
- Scabies DemodicosisDocument35 pagesScabies DemodicosisrishikeshkallaNo ratings yet
- Caninedemodicosis SheilaTorres 211127 143246Document64 pagesCaninedemodicosis SheilaTorres 211127 143246Ahmed eisaNo ratings yet
- Skin Diseases Presentation2Document40 pagesSkin Diseases Presentation2DaniTadeNo ratings yet
- DermatologyDocument223 pagesDermatologySahan EpitawalaNo ratings yet
- Atopic DermatitisDocument43 pagesAtopic DermatitisSaurav Arora100% (2)
- Atopic DermatitisDocument22 pagesAtopic DermatitisAbdul Hamid Alraiyes100% (2)
- Dms146 Slide DermatitisDocument65 pagesDms146 Slide DermatitisAdhitya Rama Jr.No ratings yet
- Dermatology Class NotesDocument48 pagesDermatology Class Notesapi-26938624100% (6)
- Bacterial Skin Infections GuideDocument41 pagesBacterial Skin Infections GuideUmmi Rinandari100% (1)
- Eczema Remedies | How to Relieve Eczema With Diet & Natural RemediesFrom EverandEczema Remedies | How to Relieve Eczema With Diet & Natural RemediesRating: 4 out of 5 stars4/5 (1)
- Exfoliative Dermatitis, (Erythroderma) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandExfoliative Dermatitis, (Erythroderma) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Pompholyx, (Dyshidrotic Ezcema) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandPompholyx, (Dyshidrotic Ezcema) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Eczema No More: The Complete Guide to Natural Cures for Eczema and a Holistic System to End Eczema & Clear Your Skin Naturally & PermanentlyFrom EverandEczema No More: The Complete Guide to Natural Cures for Eczema and a Holistic System to End Eczema & Clear Your Skin Naturally & PermanentlyRating: 5 out of 5 stars5/5 (1)
- Epiroc MTH46BDocument8 pagesEpiroc MTH46BGalo DoloresNo ratings yet
- Adoption: Legal DefinitionDocument8 pagesAdoption: Legal Definitionsharon victoria mendezNo ratings yet
- Concept MapDocument1 pageConcept MapKeith20% (5)
- Gustav Vasa BIBLE, 1541.Document93 pagesGustav Vasa BIBLE, 1541.Molitvena zajednica sv. Mihaela arhanđela100% (3)
- Form 4 Biology Chapter OverviewDocument21 pagesForm 4 Biology Chapter OverviewKar KuanNo ratings yet
- Piata de Publicitate 2012-2020 - Prezentare RezumativaDocument5 pagesPiata de Publicitate 2012-2020 - Prezentare RezumativamanageranticrizaNo ratings yet
- Murder Conviction UpheldDocument9 pagesMurder Conviction UpheldBobNo ratings yet
- RTR - Nonmetallic Pipng ProcedureDocument16 pagesRTR - Nonmetallic Pipng Proceduremoytabura96100% (1)
- Consumers Guide To The ExpertsDocument406 pagesConsumers Guide To The ExpertsHassan Younhous Traore KonéNo ratings yet
- The Black Emperor's Grand Grimoire - by Frank GenghisDocument144 pagesThe Black Emperor's Grand Grimoire - by Frank GenghisFrank Genghis0% (2)
- Lect 1 Transforming EER Diagrams Into Relations (Part III)Document13 pagesLect 1 Transforming EER Diagrams Into Relations (Part III)KIM OFFNo ratings yet
- Institute of Graduate Studies (Igs)Document46 pagesInstitute of Graduate Studies (Igs)Syara Shazanna ZulkifliNo ratings yet
- The Impact of COVID-19 On The Steel IndustryDocument25 pagesThe Impact of COVID-19 On The Steel IndustryAyesha KhalidNo ratings yet
- Kuruk Etra:: Dharma-K Etra Śalya-ParvaDocument1 pageKuruk Etra:: Dharma-K Etra Śalya-ParvaRavinder Khullar100% (1)
- Second Travel of Rizal: Week 8 Unit 3Document22 pagesSecond Travel of Rizal: Week 8 Unit 3John Russell GasangNo ratings yet
- Seagate WD Hard Drive Price List From Billion HoDocument4 pagesSeagate WD Hard Drive Price List From Billion HoALi RAzaNo ratings yet
- Taeka HaileleulDocument167 pagesTaeka HaileleulBini100% (1)
- Group L2 Nitish at Solutions UnlimitedDocument10 pagesGroup L2 Nitish at Solutions UnlimitedMani ThomasNo ratings yet
- Human Ear and Role of Hearing in HCIDocument4 pagesHuman Ear and Role of Hearing in HCIrafia0% (1)
- Novec1230 RoomIntegrityDocument2 pagesNovec1230 RoomIntegritynastyn-1No ratings yet
- G25M R TransmissionDocument29 pagesG25M R TransmissionMaksym VovkNo ratings yet
- Individualized Learning Program Project Evaluation FormDocument3 pagesIndividualized Learning Program Project Evaluation Formakbisoi1No ratings yet
- Deutz td2011 l04w Service Manual PDFDocument7 pagesDeutz td2011 l04w Service Manual PDFLuis Carlos RamosNo ratings yet
- LP Lab ManuelDocument23 pagesLP Lab ManuelRavi Kumar LankeNo ratings yet
- Acid-Base Neut Inquiry Student Handout JN KEYDocument5 pagesAcid-Base Neut Inquiry Student Handout JN KEYbradle2005No ratings yet
- Enthalpy ChangesDocument2 pagesEnthalpy Changesapi-296833859100% (1)
- Legal Documents Evidence in Safety Related Proceedings 1663086621Document9 pagesLegal Documents Evidence in Safety Related Proceedings 1663086621richardNo ratings yet
- 7 Principles Video Content CreationDocument2 pages7 Principles Video Content CreationJackiee Fiorela PalaciosNo ratings yet
- LPC Licensure Process HandbookDocument14 pagesLPC Licensure Process HandbookMac PatelNo ratings yet
- Rulings On Healing and RukiyaDocument324 pagesRulings On Healing and RukiyatheproboxerNo ratings yet