You might also like
- Exercise 1 Gametogenesis ReviewerDocument4 pagesExercise 1 Gametogenesis ReviewerJasper AdonisNo ratings yet
- General Cytogenetics InformationDocument11 pagesGeneral Cytogenetics Informationjo_jo_mania100% (1)
- Para Compre 2Document17 pagesPara Compre 2serainie maiNo ratings yet
- The Immune System OhtDocument6 pagesThe Immune System OhtKa-Shun Leung100% (1)
- Hemostasis and Thrombosis: OutlineDocument11 pagesHemostasis and Thrombosis: OutlineManila MedNo ratings yet
- DermDocument10 pagesDermyassrmarwaNo ratings yet
- TABLE (Coccidia)Document8 pagesTABLE (Coccidia)TRISHA MAE ORDONANo ratings yet
- Hematology NotesdocxDocument11 pagesHematology NotesdocxdmclmllNo ratings yet
- The Complement SystemDocument4 pagesThe Complement SystemExamville.com100% (1)
- Lecture 3 Figure 1 - Motor TractsDocument9 pagesLecture 3 Figure 1 - Motor TractsSusanaGonzálezFernándezNo ratings yet
- Nephrotic Syndrome WikipediaDocument10 pagesNephrotic Syndrome WikipediaJohn KevlarNo ratings yet
- Commensal AmoebaDocument2 pagesCommensal AmoebaCoy NuñezNo ratings yet
- Saturday Nation 27th April 2013Document72 pagesSaturday Nation 27th April 2013Pinto PioNo ratings yet
- Infectious Disease (Part 1) : Viral DiseasesDocument11 pagesInfectious Disease (Part 1) : Viral Diseasesmiguel gaquitNo ratings yet
- Chronic Inflammatory Dermatoses Inflammatory Blistering DisordersDocument4 pagesChronic Inflammatory Dermatoses Inflammatory Blistering DisordersspringdingNo ratings yet
- Esphagus Stomach Duodenum Gross AnatomyDocument9 pagesEsphagus Stomach Duodenum Gross AnatomyWinchester LoapedNo ratings yet
- Chapter 9-SensesDocument74 pagesChapter 9-SensesMaiah DinglasanNo ratings yet
- MCB 252 Final Exam Study GuideDocument62 pagesMCB 252 Final Exam Study GuideJay ZNo ratings yet
- Ontogeny and Phylogeny of Immune SystemDocument3 pagesOntogeny and Phylogeny of Immune SystemPM Basiloy - AloNo ratings yet
- Acidfaststaining 140111210509 Phpapp02Document16 pagesAcidfaststaining 140111210509 Phpapp02AnjuNo ratings yet
- Renal SyndromeDocument13 pagesRenal SyndromeAndreas KristianNo ratings yet
- Hematology Abnormal White Blood CellDocument4 pagesHematology Abnormal White Blood CellBryan James LinNo ratings yet
- Kidney Physiology (Q & A)Document28 pagesKidney Physiology (Q & A)ramadan100% (1)
- Patho A 1. 11 Infectious Diseases Tagayuna 2015Document10 pagesPatho A 1. 11 Infectious Diseases Tagayuna 2015Ala'a Emerald AguamNo ratings yet
- Cytogenetics Course PackDocument29 pagesCytogenetics Course Packanonymous squashNo ratings yet
- Abdominal Pain: No. Features Explanation Associated WithDocument4 pagesAbdominal Pain: No. Features Explanation Associated WithNazmun LailahNo ratings yet
- Kidney NewDocument4 pagesKidney NewParth BhayanaNo ratings yet
- NSAID's "Non-Steroidal Anti-Inflammatory Drugs": Mmbakhaitan@uqu - Edu.saDocument19 pagesNSAID's "Non-Steroidal Anti-Inflammatory Drugs": Mmbakhaitan@uqu - Edu.saAhmed HossamNo ratings yet
- Histo Review 2Document13 pagesHisto Review 2Coy NuñezNo ratings yet
- Diseases of ImmunityDocument13 pagesDiseases of ImmunityRose AnnNo ratings yet
- 2 Phlebotomy Notes Taken From The Lecture of Sir Antonio Pascua JR RMTDocument5 pages2 Phlebotomy Notes Taken From The Lecture of Sir Antonio Pascua JR RMTRhoda Mae CubillaNo ratings yet
- Saturday 2014-10-11 PDFDocument72 pagesSaturday 2014-10-11 PDFKamau GabrielNo ratings yet
- EAR Anatomy, Physiology, Embryology & Congenital AnomalyDocument6 pagesEAR Anatomy, Physiology, Embryology & Congenital AnomalyThakoon TtsNo ratings yet
- Abdominal Wall, Omentum, Mesentery, RetroperitoneumDocument6 pagesAbdominal Wall, Omentum, Mesentery, RetroperitoneumMon Ordona De GuzmanNo ratings yet
- MLT503 - L2 - General Properties of VirusesDocument51 pagesMLT503 - L2 - General Properties of VirusesMuhammad FirdausNo ratings yet
- Photo Me TryDocument3 pagesPhoto Me TrylcrujidoNo ratings yet
- Immunity To MicrobesDocument65 pagesImmunity To Microbesmulatumelese100% (1)
- Abdominal OrgansDocument28 pagesAbdominal OrgansRS BuenavistaNo ratings yet
- Upper and Lower Limb NervesDocument6 pagesUpper and Lower Limb NervesTaimoor DogarNo ratings yet
- Histo Ra 3 - Barbosa, Azenith VincentDocument7 pagesHisto Ra 3 - Barbosa, Azenith VincentMinamiSapphire BarbosaNo ratings yet
- Differential Count WBCDocument4 pagesDifferential Count WBCacxieNo ratings yet
- Reference: Chapter 47. Basic and Clinical Pharmacology - 13th Edition. Katzung and Trevor. Lec GuideDocument8 pagesReference: Chapter 47. Basic and Clinical Pharmacology - 13th Edition. Katzung and Trevor. Lec GuideselflessdoctorNo ratings yet
- Topic Outline: Elements of Parasitology (3P's) Types of Association of Living OrganismsDocument6 pagesTopic Outline: Elements of Parasitology (3P's) Types of Association of Living OrganismsJhunrick Corpuz TumpalanNo ratings yet
- Mtle ScoresDocument3 pagesMtle Scoresapi-296788592No ratings yet
- Essential Update: FDA Approves First Test To Predict AKI in Critically Ill PatientsDocument5 pagesEssential Update: FDA Approves First Test To Predict AKI in Critically Ill PatientsRika Ariyanti SaputriNo ratings yet
- Lymphatic SystemDocument22 pagesLymphatic SystemArnab GuinNo ratings yet
- AnemiaDocument9 pagesAnemiaMila Canoza HerreraNo ratings yet
- Hemoflagellates PDFDocument72 pagesHemoflagellates PDFChavel ReyesNo ratings yet
- Schematic Diagram of The Pathophysiology of Toxic Shock SyndromeDocument2 pagesSchematic Diagram of The Pathophysiology of Toxic Shock SyndromeRan MaNo ratings yet
- SYPHYLISDocument1 pageSYPHYLISkhadzxNo ratings yet
- Subcutaneous Mycoses Hand-OutsDocument5 pagesSubcutaneous Mycoses Hand-OutsKristine BarquillaNo ratings yet
- Hema I Chapter 4 - AnticoagDocument16 pagesHema I Chapter 4 - AnticoagderibewNo ratings yet
- Histopath Lec - Week 2 - Topic 2Document3 pagesHistopath Lec - Week 2 - Topic 2Juren LasagaNo ratings yet
- Microscopy TransDocument2 pagesMicroscopy TransMarco TolentinoNo ratings yet
- Chapter 3 Genetic VariationDocument21 pagesChapter 3 Genetic VariationAbdulkarimNo ratings yet
- VanPutte Seeleys Essentials 11e Chap07 PPT AccessibleDocument140 pagesVanPutte Seeleys Essentials 11e Chap07 PPT AccessibleCyrille Aira AndresaNo ratings yet
- Hematology: Benign White Cell Disorder DR Thuy Feb 21 2017Document5 pagesHematology: Benign White Cell Disorder DR Thuy Feb 21 2017IS99057No ratings yet
- Immune System: Review OF Introductory ProcessesDocument4 pagesImmune System: Review OF Introductory ProcessesaudreyNo ratings yet
- Concept of Inflammatory and Immune SystemDocument15 pagesConcept of Inflammatory and Immune SystemUchiha Dominic100% (1)
- 14 Lymphatic SystemDocument3 pages14 Lymphatic SystemGracia Dela CruzNo ratings yet
- Covid 19 CPR 7 RulesDocument21 pagesCovid 19 CPR 7 RulesMiguel Cuevas DolotNo ratings yet
- How Can Patients Visitors Help - May18Document2 pagesHow Can Patients Visitors Help - May18Miguel Cuevas DolotNo ratings yet
- Effectiveness of Transdermal MagnesiumDocument2 pagesEffectiveness of Transdermal MagnesiumMiguel Cuevas Dolot100% (1)
- PSB 368Document6 pagesPSB 368Miguel Cuevas DolotNo ratings yet
- Covid 19 CPR 7 RulesDocument21 pagesCovid 19 CPR 7 RulesMiguel Cuevas DolotNo ratings yet
- ACLS Cardiac Arrest Algorithm For Suspected or Confirmed COVID-19 PatientsDocument1 pageACLS Cardiac Arrest Algorithm For Suspected or Confirmed COVID-19 PatientsMariuxi Tatiana ChocoNo ratings yet
- (MED) COVID-19 Trans V. 2.0Document6 pages(MED) COVID-19 Trans V. 2.0Isabel VinasNo ratings yet
- Covid 19 PDFDocument18 pagesCovid 19 PDFMiguel Cuevas DolotNo ratings yet
- Physical Examination in ENT: Ussana Promyothin, MDDocument60 pagesPhysical Examination in ENT: Ussana Promyothin, MDMiguel Cuevas DolotNo ratings yet
- Clinical Examination of The Ear, Nose and Throat: Dave Pothier ST Mary's 2003Document30 pagesClinical Examination of The Ear, Nose and Throat: Dave Pothier ST Mary's 2003Ekambaram TrmNo ratings yet
- Physical Examination in ENT: Ussana Promyothin, MDDocument60 pagesPhysical Examination in ENT: Ussana Promyothin, MDMiguel Cuevas DolotNo ratings yet
- Physical Assessment: Ear, Nose, Mouth, and ThroatDocument59 pagesPhysical Assessment: Ear, Nose, Mouth, and ThroatMiguel Cuevas DolotNo ratings yet
- Vertigo Gail Ishiyama 1 13 10Document40 pagesVertigo Gail Ishiyama 1 13 10Myname Rama LienNo ratings yet
- Pedia Tickler Update 2017Document2 pagesPedia Tickler Update 2017Tani BokNo ratings yet
- Cook Book (Filipino) 13 PDFDocument23 pagesCook Book (Filipino) 13 PDFAdina AnghelNo ratings yet
- Drug IndexDocument2 pagesDrug IndexMiguel Cuevas DolotNo ratings yet
- Active Listening HANDOUT PDFDocument26 pagesActive Listening HANDOUT PDFMiguel Cuevas DolotNo ratings yet
- Nocturnals Physiology 2018Document14 pagesNocturnals Physiology 2018Miguel Cuevas DolotNo ratings yet
- Benign Paroxysmal Positional Vertigo: Waseem WatadDocument37 pagesBenign Paroxysmal Positional Vertigo: Waseem WatadnoviNo ratings yet
- A Case-Control Study of The Association of Diet and Obesity With Gout in Taiwan PDFDocument12 pagesA Case-Control Study of The Association of Diet and Obesity With Gout in Taiwan PDFMiguel Cuevas DolotNo ratings yet
- A Case-Control Study of The Association of Diet and Obesity With Gout in Taiwan PDFDocument12 pagesA Case-Control Study of The Association of Diet and Obesity With Gout in Taiwan PDFMiguel Cuevas DolotNo ratings yet
- Clinical AbstractDocument4 pagesClinical AbstractMiguel Cuevas DolotNo ratings yet
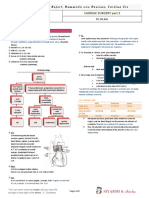
- TCVS - Cardiac Surgery Part 2 Dr. de AsisDocument8 pagesTCVS - Cardiac Surgery Part 2 Dr. de AsisMiguel Cuevas DolotNo ratings yet
- Neurologic ExamDocument1 pageNeurologic ExamMiguel Cuevas DolotNo ratings yet
- HEMAreviewDocument3 pagesHEMAreviewMiguel Cuevas DolotNo ratings yet
- Anesthesia Pocket Cards 7 18 18Document6 pagesAnesthesia Pocket Cards 7 18 18Miguel Cuevas DolotNo ratings yet
- Community-Acquired Pneumonia - CPG 2016Document26 pagesCommunity-Acquired Pneumonia - CPG 2016Jamie SebastianNo ratings yet
- Kerosene PDFDocument31 pagesKerosene PDFRudyMLanaNo ratings yet
- History Taking ExaminationDocument7 pagesHistory Taking ExaminationIndunil AnuruddhikaNo ratings yet
- Vibrations - NptelDocument3 pagesVibrations - NptelMSK65No ratings yet
- The Ecological Effects of Eucalyptus PDFDocument97 pagesThe Ecological Effects of Eucalyptus PDFgejuinaNo ratings yet
- Diels-Alder Reaction: MechanismDocument5 pagesDiels-Alder Reaction: MechanismJavier RamirezNo ratings yet
- Refrigeration Engineer Quick ReferenceDocument2 pagesRefrigeration Engineer Quick ReferenceventilationNo ratings yet
- Primary Three Exam Question.Document17 pagesPrimary Three Exam Question.ogidan preciousNo ratings yet
- Airbus A319-A320-A321 - Quick Reference HandbookDocument113 pagesAirbus A319-A320-A321 - Quick Reference Handbookrafaelldalpra100% (9)
- Business Model Navigator Whitepaper - 2019Document9 pagesBusiness Model Navigator Whitepaper - 2019Zaw Ye HtikeNo ratings yet
- FENA-01 - 11 - 21 - Ethernet Adapter - User's Manual - Rev BDocument388 pagesFENA-01 - 11 - 21 - Ethernet Adapter - User's Manual - Rev BQUOC LENo ratings yet
- 173 EvidenceDocument6 pages173 EvidenceSantiago RubianoNo ratings yet
- ELC609F12 Lec0 IntroductionDocument16 pagesELC609F12 Lec0 IntroductionMohammed El-AdawyNo ratings yet
- Sindarin-English Dictionary - 2nd EditionDocument192 pagesSindarin-English Dictionary - 2nd EditionNea Tan100% (1)
- Smart Locker - A Sustainable Urban Last-Mile Delivery Solution: Benefits and Challenges in Implementing in VietnamDocument14 pagesSmart Locker - A Sustainable Urban Last-Mile Delivery Solution: Benefits and Challenges in Implementing in VietnamQuynh LeNo ratings yet
- Neuromuscular Diseases. ALSDocument7 pagesNeuromuscular Diseases. ALSjalan_zNo ratings yet
- Asynchronous ChipsDocument27 pagesAsynchronous ChipsSai TejaNo ratings yet
- An Experimental Investigation On Abrasive Jet Machining by Erosion Abrasive GrainDocument3 pagesAn Experimental Investigation On Abrasive Jet Machining by Erosion Abrasive GrainPkNo ratings yet
- 1.1 - Selectividad Acti9Document34 pages1.1 - Selectividad Acti9Bladimir MichelNo ratings yet
- Mobile Communication Networks: Exercices 4Document2 pagesMobile Communication Networks: Exercices 4Shirley RodriguesNo ratings yet
- 1 Name of Work:-Improvement of Epum Road (Northern Side) Connecting With Imphal-Saikul Road I/c Pucca DrainDocument1 page1 Name of Work:-Improvement of Epum Road (Northern Side) Connecting With Imphal-Saikul Road I/c Pucca DrainHemam PrasantaNo ratings yet
- Suneet Narayan Singh (Updated CV), NDocument4 pagesSuneet Narayan Singh (Updated CV), Nnishant gajeraNo ratings yet
- Deva Surya - 19MF02Document30 pagesDeva Surya - 19MF02SaravananNo ratings yet
- 1 Quarter: 5 Grade Benchmark Scope and Sequence Pacing Guide 2015-2016Document3 pages1 Quarter: 5 Grade Benchmark Scope and Sequence Pacing Guide 2015-2016api-292307509No ratings yet
- PECI 405 ECPP 7th Sem CivilDocument96 pagesPECI 405 ECPP 7th Sem CivilYasaswi AkkirajuNo ratings yet
- Popular CultureDocument6 pagesPopular CultureAmritaNo ratings yet
- 100 Yer PM PPM 0605Document40 pages100 Yer PM PPM 0605biplabpal2009No ratings yet
- Good Stuff Courage, Resilience, Gratitude, Generosity, Forgiveness, and Sacrifice (Akhtar, Salman)Document221 pagesGood Stuff Courage, Resilience, Gratitude, Generosity, Forgiveness, and Sacrifice (Akhtar, Salman)madhugaggar999No ratings yet
- WRP Examination Extension 1 2012Document12 pagesWRP Examination Extension 1 2012Belinda JadeNo ratings yet
- VAM Must Sumitomo 1209 PDFDocument4 pagesVAM Must Sumitomo 1209 PDFnwohapeterNo ratings yet
- Eoi QAMDocument6 pagesEoi QAMPeeyush SachanNo ratings yet
- Ge Druck PTX 7535Document2 pagesGe Druck PTX 7535ICSSNo ratings yet
- Genie Z45/22Document58 pagesGenie Z45/22jonny david martinez perezNo ratings yet