You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Rhinoplasty Dissection ManualDocument185 pagesRhinoplasty Dissection ManualVikas Vats100% (3)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Original PDF Medical Terminology A Living Language 7th Edition PDFDocument41 pagesOriginal PDF Medical Terminology A Living Language 7th Edition PDFmegan.soffel782100% (34)
- PhilHealth Circular No. 0035, s.2013 Annex 2 List of Procedure Case RatesDocument98 pagesPhilHealth Circular No. 0035, s.2013 Annex 2 List of Procedure Case RatesChrysanthus Herrera50% (2)
- Illustrated Guide To Chemical Peels: Basics - Indications - UsesDocument26 pagesIllustrated Guide To Chemical Peels: Basics - Indications - UsesAdniana NareswariNo ratings yet
- Illustrated Guide To Chemical Peels: Basics - Indications - UsesDocument26 pagesIllustrated Guide To Chemical Peels: Basics - Indications - UsesAdniana NareswariNo ratings yet
- Human Anatomy & Physiology: Chapter 21-1Document103 pagesHuman Anatomy & Physiology: Chapter 21-1AngelyNo ratings yet
- Tajweed Course - Articulation PointsDocument29 pagesTajweed Course - Articulation Pointsapi-19863350100% (2)
- StainsDocument1 pageStainsLuiggi FayadNo ratings yet
- Cdc-Guideline For Disinfection and Sterilization in Health-Care Facilities-2008Document158 pagesCdc-Guideline For Disinfection and Sterilization in Health-Care Facilities-2008fuentenatura100% (1)
- Harvesting Rib Cartilage Grafts For Secondary Rhinoplasty: Background: MethodsDocument7 pagesHarvesting Rib Cartilage Grafts For Secondary Rhinoplasty: Background: MethodsLuiggi Fayad100% (1)
- StainsDocument1 pageStainsLuiggi FayadNo ratings yet
- Massry - Management of Postblepharoplasty Lower Eyelid RetractionDocument10 pagesMassry - Management of Postblepharoplasty Lower Eyelid RetractionLuiggi Fayad100% (1)
- Sterilization and Maintenance PDFDocument2 pagesSterilization and Maintenance PDFFranklin PraveenNo ratings yet
- Management of Stretch Marks (With A Focus On Striae Rubrae)Document6 pagesManagement of Stretch Marks (With A Focus On Striae Rubrae)Luiggi FayadNo ratings yet
- Gradual Approach To Refinement of The Nasal Tip: Surgical ResultsDocument6 pagesGradual Approach To Refinement of The Nasal Tip: Surgical ResultsLuiggi FayadNo ratings yet
- Annals of Plastic and Reconstructive SurgeryDocument10 pagesAnnals of Plastic and Reconstructive SurgeryLuiggi Fayad100% (2)
- Black&BlackDocument149 pagesBlack&BlackLuiggi FayadNo ratings yet
- Hezarfen Wings: A Lower Lateral Cartilage-Based Cartilage Suspension Technique For The Adjustment of Nasal Tip Rotation and Projection and The Correction of Supratip DeformityDocument5 pagesHezarfen Wings: A Lower Lateral Cartilage-Based Cartilage Suspension Technique For The Adjustment of Nasal Tip Rotation and Projection and The Correction of Supratip DeformityLuiggi FayadNo ratings yet
- A Novel Technique For Short Nose Correction in Asians: M-Shaped Conchal Cartilage Combining With Septal Extension GraftDocument3 pagesA Novel Technique For Short Nose Correction in Asians: M-Shaped Conchal Cartilage Combining With Septal Extension GraftLuiggi FayadNo ratings yet
- An Effective Algorithm For Management of Noses With Thick SkinDocument7 pagesAn Effective Algorithm For Management of Noses With Thick SkinLuiggi FayadNo ratings yet
- Conchal CartilageDocument4 pagesConchal CartilageAria WibowoNo ratings yet
- A Surgical Solution To The Deep Nasolabial Fold - Lassus, Claude 2nd PartDocument3 pagesA Surgical Solution To The Deep Nasolabial Fold - Lassus, Claude 2nd PartLuiggi FayadNo ratings yet
- Aging Nasolabial Fold and Treatment by Direct ExcisionDocument4 pagesAging Nasolabial Fold and Treatment by Direct ExcisionLuiggi FayadNo ratings yet
- Lateral Calcaneal Artery Skin FlapDocument8 pagesLateral Calcaneal Artery Skin FlapLuiggi FayadNo ratings yet
- Ethnic and Gender Considerations in The Use of Facial Injectables: Male PatientsDocument4 pagesEthnic and Gender Considerations in The Use of Facial Injectables: Male PatientsLuiggi FayadNo ratings yet
- A Modified Septal Extension Graft For The Asian Nasal TipDocument7 pagesA Modified Septal Extension Graft For The Asian Nasal TipLuiggi FayadNo ratings yet
- Anatomy of The Superficial Fascia System of The Breast: A Comprehensive Theory of Breast Fascial AnatomyDocument10 pagesAnatomy of The Superficial Fascia System of The Breast: A Comprehensive Theory of Breast Fascial AnatomyLuiggi FayadNo ratings yet
- Adjunctive Applications For Botulinum Toxin in Facial Aesthetic SurgeryDocument6 pagesAdjunctive Applications For Botulinum Toxin in Facial Aesthetic SurgeryLuiggi FayadNo ratings yet
- Evidence-Based Clinical Practice Guideline - Reduction MammaplastyDocument16 pagesEvidence-Based Clinical Practice Guideline - Reduction MammaplastyLuiggi FayadNo ratings yet
- Nanofat Grafting Basic Research and ClinicalDocument10 pagesNanofat Grafting Basic Research and ClinicalLuiggi FayadNo ratings yet
- Lateral Calcaneal Artery Skin FlapDocument8 pagesLateral Calcaneal Artery Skin FlapLuiggi FayadNo ratings yet
- MastopexyDocument15 pagesMastopexyLuiggi FayadNo ratings yet
- Blindness Following Cosmetic Injections of The FaceDocument18 pagesBlindness Following Cosmetic Injections of The FaceLuiggi FayadNo ratings yet
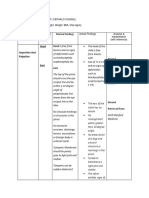
- Assessment Method Used Normal Findings: Head Head Is Free FromDocument6 pagesAssessment Method Used Normal Findings: Head Head Is Free FromGil PerezNo ratings yet
- 12.12.2017/ EN FCI-Standard #326: Yuzhnorusskaya OvcharkaDocument10 pages12.12.2017/ EN FCI-Standard #326: Yuzhnorusskaya Ovcharkainvisiblevision4No ratings yet
- PPT Skenario A - G6 - Blok 14Document66 pagesPPT Skenario A - G6 - Blok 14Ellysa CarolinnNo ratings yet
- EPISTAXIS LectureDocument30 pagesEPISTAXIS LectureDhienWhieNo ratings yet
- Nasal Septal HematomaDocument12 pagesNasal Septal HematomaNoor Al Zahraa AliNo ratings yet
- Infant Assessment FormDocument2 pagesInfant Assessment FormteuuuuNo ratings yet
- Newborn Assessment: General AppearanceDocument19 pagesNewborn Assessment: General AppearancetweExeENo ratings yet
- Case Presentatio Insomnia 1Document49 pagesCase Presentatio Insomnia 1kiran mahal100% (1)
- Tonsillitis and EpistaxisDocument17 pagesTonsillitis and EpistaxisAllaine Grace CanoNo ratings yet
- EENT Instillation and IrrigationDocument13 pagesEENT Instillation and Irrigationplebur100% (1)
- Dim Mak AnatomyDocument6 pagesDim Mak Anatomyloy7100% (6)
- Development of FaceDocument17 pagesDevelopment of FaceDr Billa AishwaryaNo ratings yet
- Step-By-step Sculpting A 90mm Figure The RoninDocument41 pagesStep-By-step Sculpting A 90mm Figure The Roninkykendra71% (7)
- Anomalias Congenitas de La NarizDocument35 pagesAnomalias Congenitas de La NarizgloristharNo ratings yet
- Chapter 7 Gross Anatomy of The Skeletal SystemDocument4 pagesChapter 7 Gross Anatomy of The Skeletal SystemDANIEL LANCE NEVADONo ratings yet
- Space Infection: Dr. Amit T. Suryawanshi Oral and Maxillofacial Surgeon Pune, India Contact Details: Email IDDocument121 pagesSpace Infection: Dr. Amit T. Suryawanshi Oral and Maxillofacial Surgeon Pune, India Contact Details: Email IDBinek NeupaneNo ratings yet
- Reconstruction of The Nasal ColumellaDocument5 pagesReconstruction of The Nasal ColumellaIndah GitaswariNo ratings yet
- Procedure 28-: Assessing The Nose and Sinuses: Physical AssessmentDocument2 pagesProcedure 28-: Assessing The Nose and Sinuses: Physical Assessmentlee jenoNo ratings yet
- La Salle University: College of Nursing Ozamiz CityDocument12 pagesLa Salle University: College of Nursing Ozamiz CityKristine NacuaNo ratings yet
- UPPER RESPIRATORY TRACT INFECTIONS QuizletDocument3 pagesUPPER RESPIRATORY TRACT INFECTIONS QuizletKatriona IntingNo ratings yet
- The Speaking ProcessDocument2 pagesThe Speaking ProcessJames William100% (1)
- O CO O CO O CO: Chapter 15: Respiratory SystemDocument3 pagesO CO O CO O CO: Chapter 15: Respiratory SystemPrecious Faith RodriguezNo ratings yet
- Special Senses ReportingDocument17 pagesSpecial Senses ReportingVanessa LopezNo ratings yet
- Cleft Lip and PalateDocument4 pagesCleft Lip and PalateAyah HyasatNo ratings yet
- Named Signs, Syndromes, Tests and ProceduresDocument64 pagesNamed Signs, Syndromes, Tests and ProceduresHAMSTRINGNo ratings yet
- How To Draw A Digital Portrait PDFDocument195 pagesHow To Draw A Digital Portrait PDFjuan_emilio100% (2)