You might also like
- Defense Mechanisms PracticeDocument2 pagesDefense Mechanisms PracticePhclivranNo ratings yet
- GynecologyDocument42 pagesGynecologyYa MaNo ratings yet
- Pectus Carinatum, (Pigeon Chest) A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandPectus Carinatum, (Pigeon Chest) A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Project On Poverty in IndiaDocument40 pagesProject On Poverty in IndiaDhananjay69% (29)
- Osce Py CompilationDocument47 pagesOsce Py CompilationBrandonRyanF.MosidinNo ratings yet
- Obstetrics - Operative Vaginal DeliveryDocument5 pagesObstetrics - Operative Vaginal DeliveryJonathanNo ratings yet
- Problems With The PassagewayDocument2 pagesProblems With The PassagewayPrilay Pring AlcopraNo ratings yet
- Post-Partum Hge - @medicine - Way2Document6 pagesPost-Partum Hge - @medicine - Way2saeed hasan saeedNo ratings yet
- High Risk Post Partum Client ReviewerDocument7 pagesHigh Risk Post Partum Client ReviewerArianJubaneNo ratings yet
- Placenta Previa (OB)Document4 pagesPlacenta Previa (OB)Winj BudayNo ratings yet
- Postpartum ComplicationsDocument7 pagesPostpartum ComplicationsCarlo BerzNo ratings yet
- 1st Trimester BleedingDocument3 pages1st Trimester BleedingdawnscribdNo ratings yet
- NCM 109 Module 2mDocument29 pagesNCM 109 Module 2mKyle ChuaNo ratings yet
- Operative ObstetricsDocument4 pagesOperative Obstetricssarguss14100% (3)
- UntitledDocument3 pagesUntitledMON RUSSEL FRIASNo ratings yet
- Fetal Malposition UpdatedDocument3 pagesFetal Malposition UpdatedJozarine Chelsea LopezNo ratings yet
- Presentation 1Document6 pagesPresentation 1Sherylou Kumo SurioNo ratings yet
- A. Prolapsed of The Cord: Accidental ComplicationDocument7 pagesA. Prolapsed of The Cord: Accidental ComplicationSophia Loraine Dorone JesuraNo ratings yet
- Face PresentationDocument4 pagesFace PresentationRose Ann HajironNo ratings yet
- 9.1.1 Maternal Anatomy - April 04 - Dra. MendozaDocument6 pages9.1.1 Maternal Anatomy - April 04 - Dra. MendozaJCAsssssiloNo ratings yet
- Diseases of The Newborn Part1Document2 pagesDiseases of The Newborn Part1sarguss14No ratings yet
- OB - Operative Vaginal Delivery (AJB)Document5 pagesOB - Operative Vaginal Delivery (AJB)Darren Mae MosadaNo ratings yet
- OB 1.01 DystociaDocument9 pagesOB 1.01 DystociaRaquel Reyes100% (1)
- Comprehensive Ob Recall 2014Document3 pagesComprehensive Ob Recall 2014Rem AlfelorNo ratings yet
- Obstructed Labor: Basliel E. (MD)Document12 pagesObstructed Labor: Basliel E. (MD)Asteway MesfinNo ratings yet
- 05.1 Obstructed Labor and Problems of The PassengerDocument16 pages05.1 Obstructed Labor and Problems of The PassengerJAN CAMILLE LENONNo ratings yet
- 1 - Dystocia - Doc GuzmanDocument7 pages1 - Dystocia - Doc Guzmand99452727No ratings yet
- 04-05 - LEC Intrapartal Care and The Labor PhenomenonDocument29 pages04-05 - LEC Intrapartal Care and The Labor PhenomenonJAN CAMILLE LENONNo ratings yet
- OB 1.01 DystociaDocument7 pagesOB 1.01 DystociaDan Paolo Diña SolayaoNo ratings yet
- HerniaDocument5 pagesHerniasarguss14100% (5)
- NCM 109 MCN Finals Topic 1 Problems With The PassengerDocument3 pagesNCM 109 MCN Finals Topic 1 Problems With The PassengerQUEZON, BRITNEY KIM E.No ratings yet
- Pathologic ObDocument8 pagesPathologic ObFvckin NonsenseNo ratings yet
- Backup of LO 2 DD HERNIA - Id.en-2Document3 pagesBackup of LO 2 DD HERNIA - Id.en-2dianNo ratings yet
- Problems of The PassengerDocument9 pagesProblems of The PassengerDanah Grace SanchezNo ratings yet
- NCM 109 Module 3mDocument25 pagesNCM 109 Module 3mKyle ChuaNo ratings yet
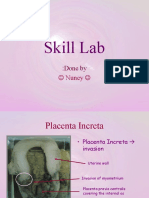
- Skill Lab: Done byDocument42 pagesSkill Lab: Done byapi-19660835No ratings yet
- CORNELL NOTE Physical and Developmental Disorders in NewbornDocument4 pagesCORNELL NOTE Physical and Developmental Disorders in NewbornMargareth DandanNo ratings yet
- NCM QuizDocument7 pagesNCM QuizKyla Marie NabongNo ratings yet
- LM 7 Pedia Lec NTSDocument5 pagesLM 7 Pedia Lec NTShanhananicasNo ratings yet
- First Stage Second Stage Third Stage I. The Powers: A. Physiology of LaborDocument4 pagesFirst Stage Second Stage Third Stage I. The Powers: A. Physiology of LaborfinellajanNo ratings yet
- Inguinal Hernia and Hydrocele: Congenital Hydrocele Presents As A Mass in The Scrotum ShortlyDocument3 pagesInguinal Hernia and Hydrocele: Congenital Hydrocele Presents As A Mass in The Scrotum ShortlyBetão AviãoNo ratings yet
- Obstructed LaborDocument4 pagesObstructed Laborkhadzx100% (2)
- Intrapartum Fetal Assessment Step 2Document3 pagesIntrapartum Fetal Assessment Step 2Andrew McGowanNo ratings yet
- Module 4 - Activity 1Document3 pagesModule 4 - Activity 1sanji vinsmokeNo ratings yet
- MCN Placenta PreviaDocument2 pagesMCN Placenta PreviaBSN 1-N CASTRO, RicciNo ratings yet
- Complications of Labor: PassengerDocument6 pagesComplications of Labor: PassengerR-Chian Jose Germanp100% (1)
- Operative Vaginal DeliveryDocument8 pagesOperative Vaginal DeliveryGerben VillanuevaNo ratings yet
- Michigan Manuel GUDocument9 pagesMichigan Manuel GUDeng PanNo ratings yet
- 2M Intrapartal Complications Written Report 109Document72 pages2M Intrapartal Complications Written Report 109kai xoxoNo ratings yet
- Labor ReadinessDocument1 pageLabor ReadinessEvidence ChaibvaNo ratings yet
- Hernia UmbilikalisDocument16 pagesHernia UmbilikalisWibhuti EmrikoNo ratings yet
- MCN Exam 4 Study Guide - Pt. 5 Neuromusclar Disorders in ChildrenDocument6 pagesMCN Exam 4 Study Guide - Pt. 5 Neuromusclar Disorders in ChildrenColin MacKenzieNo ratings yet
- Shoulder Dystocia NCPDocument6 pagesShoulder Dystocia NCPNicole Genevie MallariNo ratings yet
- Health Assesment Transes 2Document17 pagesHealth Assesment Transes 2Jayr MortaNo ratings yet
- HerniasDocument6 pagesHerniasYalin AbouhassiraNo ratings yet
- Pelvic Organ ProlapseDocument5 pagesPelvic Organ Prolapsecgao30No ratings yet
- Nursing of Client With Highrisk Labor and DeliveryDocument6 pagesNursing of Client With Highrisk Labor and DeliveryshainakyllebarbonNo ratings yet
- CN DystociaDocument7 pagesCN DystociaAlbert Francis BialaNo ratings yet
- OS 214 Renal Exam (B)Document4 pagesOS 214 Renal Exam (B)api-3799593100% (1)
- ObsNGyn - Urogynecology and Mics Topics AtfDocument17 pagesObsNGyn - Urogynecology and Mics Topics AtfarongeremewNo ratings yet
- Obstetrics - Abnormalities of The Amniotic FluidDocument6 pagesObstetrics - Abnormalities of The Amniotic FluidJonathanNo ratings yet
- Ob Finals Williams SamplexDocument86 pagesOb Finals Williams SamplexJustine MembridoNo ratings yet
- PSB 368Document6 pagesPSB 368Miguel Cuevas DolotNo ratings yet
- Physical Assessment: Ear, Nose, Mouth, and ThroatDocument59 pagesPhysical Assessment: Ear, Nose, Mouth, and ThroatMiguel Cuevas DolotNo ratings yet
- Effectiveness of Transdermal MagnesiumDocument2 pagesEffectiveness of Transdermal MagnesiumMiguel Cuevas Dolot100% (1)
- Physical Examination in ENT: Ussana Promyothin, MDDocument60 pagesPhysical Examination in ENT: Ussana Promyothin, MDMiguel Cuevas DolotNo ratings yet
- Drug IndexDocument2 pagesDrug IndexMiguel Cuevas DolotNo ratings yet
- Anesthesia Pocket Cards 7 18 18Document6 pagesAnesthesia Pocket Cards 7 18 18Miguel Cuevas DolotNo ratings yet
- Covid 19 PDFDocument18 pagesCovid 19 PDFMiguel Cuevas DolotNo ratings yet
- Anesthesia Pocket Cards 7 18 18Document6 pagesAnesthesia Pocket Cards 7 18 18Miguel Cuevas DolotNo ratings yet
- Intern App PediatricsDocument36 pagesIntern App PediatricsMiguel Cuevas Dolot100% (2)
- Lewy Body Dementias Dementia With Lewy Bodies And.9Document29 pagesLewy Body Dementias Dementia With Lewy Bodies And.9Cristina GhizdavetNo ratings yet
- Design Interventions For PandemicDocument6 pagesDesign Interventions For PandemicMahima TannuNo ratings yet
- CA TroidDocument2 pagesCA TroidSiti RohmahNo ratings yet
- Activity 14 - Community Action Plan (DIZON)Document5 pagesActivity 14 - Community Action Plan (DIZON)Louis Fetilo FabunanNo ratings yet
- The Truth About Caffeine: Medline ArtiDocument2 pagesThe Truth About Caffeine: Medline ArtiSarcastic SunSHAYNENo ratings yet
- FNH 08Document4 pagesFNH 08Ana Mae LinguajeNo ratings yet
- Job Hazard AnalysisDocument16 pagesJob Hazard AnalysisTimothy GalisinNo ratings yet
- Dengue 20230427Document11 pagesDengue 20230427Ariana hazelNo ratings yet
- Caring - Watson & SwansonDocument35 pagesCaring - Watson & SwansonDenis ArindaNo ratings yet
- Inisiasi DialisisDocument27 pagesInisiasi DialisisandarsamuelNo ratings yet
- ChlamydiaDocument15 pagesChlamydiaburntashesNo ratings yet
- Material Safety Data Sheet: - AdsealDocument12 pagesMaterial Safety Data Sheet: - Adsealwuhan lalalaNo ratings yet
- DengueDocument14 pagesDengueKarenn Joy Concepcion OctubreNo ratings yet
- Effect of Sports Participation On Social Development in Children Ages 6-14Document4 pagesEffect of Sports Participation On Social Development in Children Ages 6-14estradahoneyrheynNo ratings yet
- Trichinella SpiralisDocument20 pagesTrichinella SpiralisVlad GheorghitaNo ratings yet
- A Proposal Proposing The Implementation of Outreach Program 2019Document3 pagesA Proposal Proposing The Implementation of Outreach Program 2019Jai SabusabNo ratings yet
- Assessment of Patient's Waiting Time in The Radiology Department of A Teaching HospitalDocument5 pagesAssessment of Patient's Waiting Time in The Radiology Department of A Teaching HospitalDanica LayagNo ratings yet
- DMAC15-Medical Equipment To Be Held at The Site of An Offshore Diving OperationDocument13 pagesDMAC15-Medical Equipment To Be Held at The Site of An Offshore Diving OperationEric BouldenNo ratings yet
- 18th Amendment Working Paper PDFDocument14 pages18th Amendment Working Paper PDFIqbal Haider Butt0% (1)
- VXIDocument2 pagesVXIRue Wan UyNo ratings yet
- Benefits of Exercise: MedlinePlusDocument5 pagesBenefits of Exercise: MedlinePlusM Teresa LeivaNo ratings yet
- IS 427-Specification For Distemper, Dry, ColourDocument17 pagesIS 427-Specification For Distemper, Dry, ColoursunitkghoshNo ratings yet
- How To Write An Audit ReportDocument5 pagesHow To Write An Audit ReportWilliam Wu100% (1)
- Data Categories Administration of Information: ENTER DATA - Choose Procedure - ComputeDocument2 pagesData Categories Administration of Information: ENTER DATA - Choose Procedure - ComputeAirishNo ratings yet
- Articles Arnold Bakker 245 PDFDocument9 pagesArticles Arnold Bakker 245 PDFFranzNo ratings yet
- 01-Chapter 1 Robot Applications in IndustryDocument46 pages01-Chapter 1 Robot Applications in Industrythe altidude100% (1)
- Temporary and Permanent SplintingDocument7 pagesTemporary and Permanent SplintingGanisht AzmiNo ratings yet
- Guidelines On The Required Health Standards in Basic Education Offices and SchoolsDocument3 pagesGuidelines On The Required Health Standards in Basic Education Offices and SchoolsjeromeNo ratings yet