Professional Documents
Culture Documents
Misses and Errors in Upper Extremity Trauma Radiographs: Soterios Gyftopoulos Munish Chitkara Jenny T. Bencardino
Uploaded by
rasyidOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Misses and Errors in Upper Extremity Trauma Radiographs: Soterios Gyftopoulos Munish Chitkara Jenny T. Bencardino
Uploaded by
rasyidCopyright:
Available Formats
M u s c u l o s k e l e t a l I m a g i n g • R ev i ew
Gyftopoulos et al.
Errors in Reading Upper Extremity Trauma Radiographs
Musculoskeletal Imaging
Review
Downloaded from www.ajronline.org by 202.80.213.249 on 08/29/19 from IP address 202.80.213.249. Copyright ARRS. For personal use only; all rights reserved
FOCUS ON:
Misses and Errors in Upper
Extremity Trauma Radiographs
Soterios Gyftopoulos1 OBJECTIVE. The article reviews a select group of traumatic upper extremity injuries that
Munish Chitkara can be easily misinterpreted on radiographs.
Jenny T. Bencardino CONCLUSION. The awareness of these specific injuries and an understanding of their
underlying pathophysiology and the role that radiographs can play in their evaluation will
Gyftopoulos S, Chitkara M, Bencardino JT give the reader the best opportunity to make the important imaging findings and guide ap-
propriate treatment.
T
he role of radiographs in the eval- cept make the important finding. These types
uation of patients with upper ex- of errors can be frustrating because on sec-
tremity trauma is well estab- ond look, the diagnosis is rather obvious.
lished, serving an important role An analysis of these types of errors is be-
alongside clinical history and physical exami- yond the scope of this review. Instead, we are
nation. Radiographs can be especially helpful going to focus on the errors that can be mini-
for the patient who is a poor historian or is dif- mized by gaining a better understanding of
ficult to examine, providing information cru- the underlying anatomy and pathophysio-
cial to identifying the underlying pathologic logy of the trauma, as well as the strengths
abnormality and help direct management. and weaknesses of radiographs, for a select
The diagnosis of a major dislocation or group of upper extremity injuries that can be
comminuted fracture can usually be made easily misinterpreted and result in long-term
by the referring clinician, whether an emer- complications for the patient.
gency medicine physician or an orthopedic
surgeon. Radiologists play an important role Sternoclavicular Dislocation
in the diagnosis of more subtle easily missed Background
injuries and in recommending the best im- The sternoclavicular joint is a cartilage-
aging protocol for evaluating the patient. A lined joint formed by incongruent articular
radiologist may suggest additional views that surfaces. Capsular and ligamentous struc-
reveal injuries not easily apparent on the con- tures, including the capsular, costoclavicu-
ventional radiographic study. Radiologists lar, and interclavicular ligaments, render the
more fully understand the limitations of ra- sternoclavicular joint one of the most stable
diography for certain diagnoses and can best joints in the body, with 1% of all dislocations
Keywords: missed fracture, radiographs indicate the need for more advanced imag- and 3% of all shoulder dislocations occurring
DOI:10.2214/AJR.14.12589
ing, such as CT or MRI, to arrive at the cor- at this location [1–3]. Injuries to the sterno-
rect diagnosis in an appropriate time frame. clavicular joint are a result of direct or indi-
Received January 23, 2014; accepted after revision There are various reasons for a “miss” or rect forces usually occurring in the setting of
March 20, 2014. error when interpreting radiographs. The high-energy trauma (e.g., motor vehicle crash
1
most obvious reason is when the radiolo- or falls from a height) and contact sports (e.g.,
All authors: Department of Radiology, NYU Langone
Medical Center, 660 First Ave, New York, NY 10016.
gist overlooks the finding, which is present rugby, wresting, or football) [3]. The medial
Address correspondence to S. Gyftopoulos on the study, during the initial review. This aspect of the sternoclavicular joint is usual-
(Soterios20@gmail.com). miss could be secondary to a number of dif- ly the target for injuries related to direct trau-
ferent causes, such as an error of speed, er- ma, whereas forces along the anterolateral or
AJR 2014; 203:477–491 ror in search technique, satisfaction of search, anteromedial aspects of the shoulder can in-
0361–803X/14/2033–477
or error due to multitasking. Another reason directly disrupt the joint [3]. Because of the
may be that your eyes “played a trick on you,” propensity of this type of injury to occur in
© American Roentgen Ray Society and frankly you did everything correctly ex- high-energy trauma, sternoclavicular disloca-
AJR:203, September 2014 477
Gyftopoulos et al.
tions can be missed initially while the other Posterior Shoulder Dislocation glenoid, known as a reverse bony Bankart.
more apparent and possibly more serious inju- Background This is best seen on the axillary view and
ries are treated [4–6]. A careful evaluation of The glenohumeral joint provides the larg- typically presents as a discrete osseous frag-
the patient’s history and physical examination est range of motion of all the body’s large ment adjacent to the posterior glenoid. When
findings may raise the possibility of a sterno- joints, maintained by a coordinated interplay there is high suspicion for posterior disloca-
clavicular joint disruption. of dynamic and static stabilizers [9, 10]. This tion and negative radiographs, MRI is the
Downloaded from www.ajronline.org by 202.80.213.249 on 08/29/19 from IP address 202.80.213.249. Copyright ARRS. For personal use only; all rights reserved
degree of mobility is mainly a function of the next imaging modality of choice given its
Imaging discrepancy in sizes of the articular surfac- high diagnostic performance in the evalua-
The initial imaging evaluation typically es of the joint with the much larger humer- tion of radiographically occult bone trauma
consists of radiographs of the sternoclavicular al head articulating with the smaller glenoid, and associated capsulolabral injuries that
joints and sternum, both anteroposterior and similar to the relationship between a golf ball may require surgical repair [18, 19].
lateral views. A serendipity view, which is an and a tee. Failure of the stabilizing mecha-
oblique view centered on the sternum and ori- nism will lead to shoulder instability. Long-Term Follow-Up and Complications
ented 40° of vertical that shows both sterno- Posterior shoulder dislocations are much Delay in the diagnosis of posterior dis-
clavicular joints for comparison, should also less common than anterior dislocations (1.1 vs location can result in persistent pain, de-
be included [7]. These images can be diffi- 23.9 cases/100,000 population per year) but creased function, and glenohumeral osteo-
cult to evaluate for several reasons, including are much more frequently misdiagnosed at ini- arthrosis [14]. Osteonecrosis of the humeral
overlap of bones and soft tissues around the tial presentation (up to 79% of the time) [11]. head has also been described in the setting of
joints and positioning, which may be limited The most common cause for posterior shoulder posterior dislocation and fracture of the hu-
because of the patient’s condition. dislocation is high-energy trauma that results meral neck [20]. Unlike in the setting of an-
High suspicion for injury in this location in a force directed onto the shoulder placed in terior shoulder dislocation, recurrent posteri-
should prompt further evaluation with CT, a flexed, adducted, and internally rotated po- or dislocation is less common because of the
the current imaging reference standard for sition [12–16]. Seizures are another common protracted positioning of the scapula, which
assessment of the sternoclavicular joints [6, cause (31% of the time) for posterior instabili- enhances the role of the posterior glenoid as
8]. CT allows a complete evaluation of the ty, related to asymmetric sustained contraction a barrier to instability [11, 21, 22].
sternoclavicular joints and any associated of the internal rotator muscles pulling the hu-
injuries, including fractures and soft-tissue meral head posteriorly [11]. Pearls
injuries. CT is especially important when In any patient with shoulder trauma (es-
there is concern for a posterior dislocation of Imaging pecially with suspected instability), the re-
the medial clavicle head, a finding that can The imaging evaluation should begin with lationship between the humeral head and
be easily missed on radiographs, because it anteroposterior internal, anteroposterior exter- glenoid is important to review. An axillary
can result in an emergent and possibly life- nal, scapular Y, and axillary views of the in- view or transscapular Y view is mandatory to
threatening vascular injury [4, 6] (Fig. 1). jured shoulder. The relationship between the evaluate the joint and rule out malalignment.
humeral head and glenoid is best evaluated on The presence of a sclerotic line (or lines)
Long-Term Follow-Up and Complications the axillary and scapular Y views because the parallel to the anterior humeral head cortex
The predominant long-term complication humeral head is seen along the posterior mar- is suggestive of an impaction fracture. This
of a sternoclavicular dislocation is the de- gin of the glenoid, inferior to the acromion, in finding should then lead to a careful evalua-
velopment of osteoarthrosis and associated the setting of a posterior dislocation (Fig. 2). tion of the posterior glenoid rim for possible
chronic pain [3]. The degenerative change Evaluation of the glenohumeral joint align- fracture and to confirm the diagnosis of prior
may also present as swelling over the sterno- ment is more difficult on the anteroposterior posterior dislocation.
clavicular joint, which can be confused for a views because the humeral head may not look
soft-tissue or bone mass, resulting in an ad- displaced. Posterior dislocation can be sus- Scapular Fractures
ditional workup [3]. pected when the humeral head appears to be Background
internally rotated on both anteroposterior in- The scapula is a flat triangular bone that is
Pearls ternal and external rotation views, related to protected superficially and anteriorly by the
There are two keys to making a correct di- the fixed position of the dislocated head. rib cage. In addition, the surrounding muscu-
agnosis of a sternoclavicular joint injury. First, The diagnosis can become more difficult lature, most notably the rotator cuff muscles,
a high index of suspicion is necessary. Make if the patient’s shoulder has relocated by the serve as a protective layer, dissipating the
sure to evaluate the sternoclavicular joints in time of presentation for imaging. A search forces that may be directed toward the scap-
any patient with a history of direct trauma to for osseous injuries related to posterior in- ula. For these reasons, fractures of the scap-
the anterior neck and chest. Second, know stability can provide clues to the diagnosis. ula are rare injuries, accounting for less than
the limitations of radiographs for this diagno- The impaction fracture of the humeral head 1% of all fractures and 5% of all shoulder
sis. The degree of overlap from the surround- is seen as a vertically oriented linear region fractures [23, 24]. Scapular fractures are of-
ing bones and soft tissues limits the ability to of sclerosis along the anterior half of the ten the result of high-energy trauma, where
evaluate these joints. If the history and physi- humeral head, parallel to the anterior cor- there is a direct force impacting the scapula
cal examination findings fit, recommend a CT tex, and is referred to as the “trough line” or [23, 24]. Indirect forces, such as a humeral
of the sternoclavicular joints to make sure this “trough sign” [17] (Fig. 2A). The reciprocal head colliding with the glenoid, can also re-
diagnosis is not missed. injury would be a fracture of the posterior sult in fractures. Finally, various avulsion in-
478 AJR:203, September 2014
Errors in Reading Upper Extremity Trauma Radiographs
juries can occur, including avulsions of the Greater Tuberosity Fractures tings, MRI can also be used to evaluate for
coracoid process at the origin of the con- Background associated pathologic abnormalities involving
joint tendon and of the acromion at the ori- The greater tuberosity is the largest tuber- the rotator cuff, labrum, and glenoid, which
gin of the deltoid muscle [23, 24]. The most cle found at the humeral head, with three fac- are not as well assessed on radiographs.
common location for fracture is the scapu- ets (superior, middle, and inferior) serving as
lar body or spine (50%), followed by the gle- the insertion sites for the supraspinatus, infra- Pearls
Downloaded from www.ajronline.org by 202.80.213.249 on 08/29/19 from IP address 202.80.213.249. Copyright ARRS. For personal use only; all rights reserved
noid neck (25%), glenoid articular surface spinatus, and teres minor tendons. Fractures Careful evaluation of the greater tuberos-
(10%), and coracoid process and acromion of the greater tuberosity encompass 19% of ity on anteroposterior external radiographs
(7% each) [23, 24]. all humeral fractures [26]. Both its size and is the key to this diagnosis, especially if the
its role as a tendon attachment site predispose fracture is not displaced or only minimally
Imaging the greater tuberosity to injury, which typical- displaced. The profile view of the tuberosity
There is a tendency for these fractures to ly occurs in one of two ways. The first mecha- will give the radiologist the best opportunity
be missed initially because the clinical focus nism, direct impaction, occurs when a direct to evaluate the tuberosity cortex and to ac-
is on other more serious injuries that tend to blow results in impaction of the tuberosity curately assess the degree of displacement.
occur at the same time as the initial trauma against the adjacent scapula [27, 28]. Depend-
[23, 24]. The imaging evaluation should be- ing on the direction of force and position of Radial Head Fractures
gin with anteroposterior and lateral views the shoulder, the greater tuberosity can impact Background
of the scapula and an axillary view of the the acromion, the superior glenoid, or, most The radial head plays an important role in
shoulder. Evaluation can be difficult because commonly, the anterior glenoid in the setting stabilization of the elbow and forearm [32].
of the complex scapular anatomy and osse- of anterior shoulder instability. The second It serves as an important stabilizer against
ous and soft-tissue overlap. This is why the mechanism is related to avulsion of the great- valgus-directed forces, especially when the
radiologist should systematically review the er tuberosity in the setting of anterior shoulder ulnar collateral ligament is insufficient or
different parts of the scapula on each view, dislocation as the rotator cuff contracts in an torn [33]. The radiocapitellar joint serves
including the coracoid process, glenoid, and attempt to offset the displacement of the hu- as an important stabilizer against axial or
acromion, as well the three scapular articu- meral head [27, 28]. compressive forces, both preventing proxi-
lations (scapulothoracic, glenohumeral, and mal migration of the radius and maintain-
acromioclavicular) for any incongruity (Fig. Imaging ing normal compressive load distribution at
3). If the radiographs fail to reveal a signif- The diagnosis of a greater tuberosity the wrist along with the interosseous mem-
icant pathologic abnormality but there is a fracture is difficult on the basis of clinical brane and triangular fibrocartilage complex
persistent concern for a scapular fracture, CT grounds only. The imaging evaluation of the [34, 35]. The radial head also serves as a sec-
with 3D reconstructions should be consid- patient with shoulder trauma typically con- ond stabilizer against posterolateral directed
ered as the next imaging tool [25]. CT will sists of anteroposterior internal and external forces along with the lateral joint capsule and
best reveal the presence and extent of a frac- views, scapular Y, and axillary view of the in- ligaments (radial collateral and lateral ulnar
ture and any associated injuries or impend- jured extremity. The anteroposterior external collateral ligaments) [32].
ing complications to the surrounding mus- view is of special interest and may provide Radial head fractures are the most com-
cles and neurovascular structures [25]. the best opportunity to diagnose a fracture, mon fracture at the elbow, encompassing ap-
especially when it is subtle [29] (Fig. 4). The proximately one third of all the fractures that
Long-Term Follow-Up and Complications greater tuberosity is held in profile on this occur at the elbow and 3% of fractures over-
Most scapular fractures are treated con- view, which allows a clear depiction of its all in the adult population [32, 36, 37]. Frac-
servatively without surgery because the de- cortex and any superior or lateral displace- tures of the radial head typically occur in the
gree of displacement, which can affect the ment of the fracture fragments, an important setting of a fall on an outstretched hand, oc-
healing potential of a fracture, is usually characteristic because of its treatment impli- curring in isolation or after elbow dislocation.
kept to a minimum by the adjacent muscu- cations [29]. Similarly, the axillary view can
lature [24]. A good healing response with- show lateral displacement of the fragments. Imaging
out significant impaired function is expected The axillary view along with the scapular Y The initial imaging evaluation typical-
usually within 6 weeks [24]. and anteroposterior internally rotated views ly includes anteroposterior, lateral, and
are also used to assess for associated inju- Greenspan views of the injured elbow.
Pearls ries, including glenohumeral dislocation and The Greenspan view is a type of lateral
The key to this diagnosis is to systemati- glenoid fracture. view taken with 45° angulation of the x-ray
cally review the different parts of the scapula If further characterization of the greater beam toward the radial head [38]. This re-
on each of the available radiographic views. tuberosity fracture is needed for treatment sults in an isolated view of the radial head,
If suspicion persists despite negative radio- purposes (i.e., extent, comminution, and dis- free of osseous overlap (i.e., coronoid proc-
graphs, CT with 3D reconstructions is in- placement), a CT should be ordered [30, 31]. ess). Nondisplaced fractures may not be ap-
dicated for definitive evaluation. Although MRI is typically performed when the radio- parent on the initial radiographs, but sec-
most of these injuries are treated conserva- graphs are negative but there is high suspi- ondary signs of a fracture can be seen. The
tively, the diagnosis of a scapular fracture cion for fracture, in cases with poor clinical presence of a joint effusion in a patient with
may explain a person’s shoulder pain when response, and when anterior glenohumeral in- recent trauma should make the radiologist
other causes have been ruled out or treated. stability injuries are suspected. In these set- look at the images carefully for a fracture.
AJR:203, September 2014 479
Gyftopoulos et al.
If one is not seen, then a “radiographically Coronoid Process Fractures characterize the location or type of frac-
occult” fracture should be considered and Background ture, CT is the next best imaging modality
the patient should be treated as such (Fig. The coronoid process forms the anteri- to recommend. CT will show the extent of
5). Follow-up radiographs obtained 7–10 or half of the greater sigmoid notch of the the fracture, displacement of the fragments,
days after this initial set of views may bet- ulna, articulating with the humeral trochlea. and intraarticular bodies. MRI is also ex-
ter show the fracture because of the heal- The process is often subdivided into differ- cellent for radiographically occult fractures
Downloaded from www.ajronline.org by 202.80.213.249 on 08/29/19 from IP address 202.80.213.249. Copyright ARRS. For personal use only; all rights reserved
ing-related changes (i.e., bone resorption at ent segments, including the tip, anteromedial and to evaluate associated injuries of the
the fracture site), which make the fracture facet (which includes the sublime tubercle), capsuloligamentous structures (Fig. 6).
lines more obvious [39]. MRI could be con- and anterolateral facet. The coronoid proc-
sidered for the patient with suspected radi- ess plays an important role in elbow stabil- Pearls
al head fracture with negative radiographs, ity, serving as one of the primary restraints It is important to carefully evaluate the
given its proficiency in diagnosing radio- against varus-directed forces and, along with coronoid process on the lateral view, espe-
graphically occult fractures [18]. CT can the radius, valgus-directed forces. A coro- cially if there is evidence of a radial head
also be used in the evaluation of the radi- noid process fracture can occur in low-ener- fracture, because of the surgical implica-
al head fracture, but usually when a frac- gy trauma, such as a fall on an outstretched tions. A cortical disruption or deficiency is
ture is known and further characterization hand, or in high-energy trauma. The location likely posttraumatic in nature. An under-
is needed for treatment planning. of the fracture fragment can provide impor- standing of the size and location of the frac-
tant information on the underlying mecha- ture is also helpful in terms of defining the
Long-Term Follow-Up and Complications nism of injury and prognosis [42, 43]. underlying mechanism of injury and possible
Nondisplaced or minimally displaced ra- A fracture of the coronoid tip is typically associated soft-tissue and osseous injuries.
dial head fractures tend not to have asso- secondary to posterolateral rotatory instabil-
ciated soft-tissue or bone injuries, whereas ity, which results in shearing of the tip from Galeazzi and Monteggia Fracture-
more comminuted displaced fractures tend abnormal contact between the coronoid and Dislocations
to have associated injuries to the capsule, trochlea related to tearing of the lateral cap- Background
surrounding ligaments (ulnar collateral lig- sule [42]. The “terrible triad” is when the tip The radius and ulna form the osseous
ament and lateral collateral ligament), and fracture is found in the setting an elbow dis- components of the forearm with articula-
surrounding bones (capitellum and coro- location, with a fracture of the radial head tions proximally at the elbow and distally at
noid process fractures) [40]. To maintain [42]. This is a constellation of findings that the wrist. The main stabilizer of the proxi-
the stabilizing forces provided by the ra- invariably needs surgical stabilization and mal joint is the annular ligament, a compo-
dial head, surgical management is consid- has been consistently associated with poor nent of the lateral collateral ligament com-
ered when fragment displacement is greater outcomes [44]. A fracture of the anterome- plex, with a contribution from the quadrate
than 2 mm and in the presence of commi- dial process is typically seen in the setting of ligament. The triangular fibrocartilage com-
nution and decreased range of motion [32, posteromedial elbow instability and results plex stabilizes the distal joint. The remainder
35, 41]. Repair of associated capsuloliga- from abnormal contact between the medial of the radius and ulna are stabilized by the
mentous and bone injuries should also be trochlea and anteromedial facet as the olec- interosseous membrane.
considered at the same time as the radial ranon is subluxed or dislocated posteriorly Galeazzi and Monteggia fracture-dis-
head treatment to decrease the risk of insta- [45]. In this clinical setting (as opposed to the locations describe distinct injuries to the
bility and prevent the long-term complica- posterolateral instability), a radial head frac- bones and joints of the forearm. The Gale-
tions of chronic pain, decreased function, ture and tearing of the medial capsule are un- azzi fracture extends through the junction of
and osteoarthrosis [35]. likely and a different type of surgical fixation the middle and distal thirds of the distal ra-
is necessary to maintain stability [45]. dius with disruption of the distal radioulnar
Pearls joint [46] (Fig. 7). The Monteggia fracture
The use of a Greenspan view to evaluate Imaging propagates across the proximal third of the
the radial head is helpful, revealing frac- The initial imaging evaluation should ulna with dislocation of the radiocapitellar
tures that may not be apparent on the other consist of anteroposterior and lateral views joint [47] (Fig. 8). Although the fractures are
views. The presence of a joint effusion in of the elbow (and a Greenspan view if there usually easily diagnosed on radiographs, the
the patient with recent trauma is an impor- is suspicion for an associated radial head joint dislocations may be missed initially, af-
tant red flag for fracture when no cortical fracture). A fracture of the coronoid process fecting patient outcome and treatment [48].
disruption or impaction is present. In this can be easily missed on radiographs. Over- Fracture-dislocations of the forearm typical-
scenario, the patient should be considered lap on the anteroposterior and lateral views ly occur with an axial load, such as a fall on
as having a “radiographically occult frac- limits visualization of the coronoid process, an outstretched hand. In the setting of a Ga-
ture” and should be asked to get additional making it difficult to diagnose a fracture, leazzi fracture, the force is strong enough to
views in 7–10 days’ time when the diagno- especially when it is nondisplaced (Fig. 6). fracture the distal radius and tear the interos-
sis of a fracture should be more definitive. A fracture of the process may also be mis- seous membrane at the same time. In the set-
Care should be taken in the patient without interpreted as a radial head fracture on the ting of a Monteggia fracture, the force frac-
trauma, because the effusion may be related lateral view because of their close proxim- tures the proximal ulna and tears the annular
to a synovially based process, such as rheu- ity. If there is suspicion for a coronoid pro- and quadrate ligaments, which results in dis-
matoid arthritis. cess fracture or if there is a need to better location of the radial head.
480 AJR:203, September 2014
Errors in Reading Upper Extremity Trauma Radiographs
Imaging Distal radial fractures require careful evalua- CT has been advocated by some authors for
The initial radiographic assessment of tion of the distal radioulnar joint, whereas the the evaluation of scaphoid fractures because
these patients should include evaluation of radiocapitellar joint should be carefully as- it provides a better representation of the ex-
the elbow, forearm, and wrist. Anteroposte- sessed in proximal ulnar fractures. act location of the fracture and the degree of
rior and lateral radiographs of the forearm displacement of the fracture fragments. MRI
should show the location and extent of the Scaphoid Fracture can also be used to show radiographically
Downloaded from www.ajronline.org by 202.80.213.249 on 08/29/19 from IP address 202.80.213.249. Copyright ARRS. For personal use only; all rights reserved
fracture. The elbow study, usually consist- Background occult fractures and associated injuries. In
ing of anteroposterior, lateral, and oblique The scaphoid plays an important role in sta- a recent study, the use of early MRI in pa-
views, will show the alignment of the joints bility of the carpus. Named after the Greek tients with suspected scaphoid fracture with
and any intraarticular injuries. The wrist ra- word for “boat” because of its oblong shape, negative radiographs also proved to be cost
diographs, consisting of posteroanterior, the scaphoid’s complex anatomy can be di- effective, reducing the patients’ immobiliza-
oblique, and lateral views, show the align- vided into different segments, including the tion time, sick leave, and nonhospital costs
ment and any carpal injuries. The location proximal pole, scaphoid waist, dorsal ridge, when compared with an algorithm consisting
of the fracture on the forearm radiographs and distal tubercle. The scaphoid is unique in of only radiographic follow-up [57].
should direct the reader to the most impor- that most of its surface is covered by articular
tant joint to evaluate next. A fracture within cartilage, which limits the entry points for nu- Long-Term Follow-Up and Complications
the distal radius should bring the reader’s at- trient vessels to the nonarticular dorsal ridge Prompt treatment is crucial, with the onus
tention toward the alignment of the distal ra- and the distal end of the scaphoid [54]. on the clinician or radiologist to make the
dioulnar joint. Findings that would suggest a The scaphoid is the most commonly frac- correct diagnosis. A delayed or missed diag-
joint disruption include widening of the dis- tured bone in the wrist [55]. This fracture is nosis of a scaphoid fracture will prevent the
tal radioulnar joint space with lack of over- typically seen in younger active patients and initiation of proper therapy, which usually
lap of the ulnar head over the distal radius results from a combination of axial and hy- consists of surgical fixation [58]. This delay
on the posteroanterior view, dislocation of perextension forces on the wrist. The loca- increases the likelihood of a poor outcome,
the ulnar head relative to the radius on the tion of the fracture and degree of displace- including persistent pain and limited mobil-
lateral view, and shortening of the distal ra- ment play a major role in patient treatment ity related to malunion, nonunion, or osteo-
dius by more than 5 mm. Comparative wrist and outcome. The more proximal the frac- necrosis with subsequent development of ra-
views can be helpful to assess for asymme- ture location within the scaphoid, and the diocarpal and intercarpal osteoarthritis [59].
try. A fracture of the proximal ulna should more displacement present at the fracture
direct the reader’s attention to the radiocapi- site, the higher the risk for poor healing in Pearls
tellar joint alignment. A line drawn through the form of malunion and nonunion [55, 56]. It is important to evaluate the scaphoid on
the center of the proximal radius should in- This poor healing potential is related to dis- all radiographic views. An additional scaph-
tersect the capitellum on all the views, giv- ruption of the tenuous blood supply to the oid view is indicated if the level of suspicion
en any degree of flexion or extension. Cross- proximal portion of the bone and the devel- is high but the initial radiographs are nega-
sectional imaging is not typically needed in opment of osteonecrosis [55, 56]. tive. For patients with negative radiographs
either of these settings because most treat- but a high index of suspicion, follow-up ra-
ment-related information is derived from the Imaging diographs in 7–10 days are recommended,
radiographs only. The initial imaging evaluation consists of because the fracture line would be made
posteroanterior, oblique, and lateral views more obvious secondary to the healing re-
Long-Term Follow-Up and Complications and a posteroanterior ulnar deviated view sponse. Because of the repercussions of a
A delayed or missed diagnosis of a Ga- with 45° of extension (i.e., the “scaphoid missed fracture, the use of MRI should be
leazzi fracture can lead to progressive sub- view”). The scaphoid’s curved shape and strongly considered if a radiographically oc-
luxation of the distal radioulnar joint, pain, palmar inclination can make its radiograph- cult scaphoid fracture is suspected.
limited range of motion, and eventual osteo- ic evaluation difficult, especially the eval-
arthritis [49–51]. Persistent radiocapitellar uation of the distal tubercle and waist seg- Scapholunate Instability
dislocation can result in chronic valgus in- ments. These portions of the bone are best Background
stability, because of the loss of the stabiliz- seen on the oblique view. The scaphoid view The primary stabilizer of the scapholunate
ing force provided by the radial head, and in can also improve visualization of these seg- joint is the scapholunate ligament, which has
radiocapitellar osteoarthrosis [52, 53]. If the ments, because the extended ulnar deviated three components—dorsal, volar, and mem-
radial head remains anteriorly dislocated, it position elongates the scaphoid and reduces branous. The dorsal component is the stron-
can also result in radial neuropathy second- the bone’s natural flexed position, limiting gest and most important component in terms
ary to nerve impingement [53]. osseous overlap (Fig. 9). of providing stability to the joint, whereas
Nondisplaced fractures of the scaphoid the volar component contributes to rotational
Pearls can be particularly challenging. The frac- stability [60]. The membranous component
Close attention to the location of a radial ture line and breaks in the cortexes may be has a minimal contribution to stability [60].
or ulnar fracture is important because it will subtle or absent on the initial radiographs. The secondary stabilizers of the scapholu-
guide the reader in terms of what to look for Even when a diagnosis of a fracture is made, nate joint are the extrinsic ligaments found
next on the present radiographs and to deter- the degree of displacement may not be ac- along the volar and dorsal aspects of the joint
mine whether additional imaging is necessary. curately characterized on the radiographs. [60]. The radioscaphocapitate, long radiolu-
AJR:203, September 2014 481
Gyftopoulos et al.
nate (radiolunotriquetral), and short radio- ial loading from the grip, and provides a com- Long-Term Follow-Up and Complications
lunate ligaments are found along the volar parison with the contralateral wrist. Diastasis A chronically unstable scaphoid can eventu-
margin, whereas the dorsal radiotriquetral of the joint on the stress views with negative ally result in scapholunate advanced collapse
and intercarpal (scaphotriquetral) ligaments static views is a common imaging presenta- [71]. This is a progressive degenerative proc-
are found over the dorsum. These extrinsic tion in the subacute setting [64]. ess that begins at the articulation of the radi-
ligaments play an important role in main- The progressive tearing of the extrinsic lig- al styloid with the scaphoid. The degenerative
Downloaded from www.ajronline.org by 202.80.213.249 on 08/29/19 from IP address 202.80.213.249. Copyright ARRS. For personal use only; all rights reserved
taining normal scapholunate kinematics. aments along with the scapholunate ligament changes progress to involve the radioscaphoid,
Scapholunate instability is defined as an will result in changes in alignment on the stat- lunatocapitate, and scaphotrapezius joints.
injury to the stabilizing forces of the scaph- ic radiographs, including diastasis, rotatory
olunate joint that contributes to a wrist that subluxation, and the “signet ring” sign, re- Pearls
is symptomatic, has difficulty bearing loads, sulting from the overlap of the distal scaphoid Dynamic radiographic evaluation can be
and shows abnormal kinematics during at pole cortical outline and the scaphoid waist crucial for the diagnosis of scapholunate in-
least a portion of its normal motion [61]. A secondary to flexion (i.e., rotary subluxation) stability, especially in differentiating be-
patient’s clinical history, physical examina- and foreshortening of the scaphoid. tween intrinsic and extrinsic ligament injury
tion results, and imaging findings all contrib- Malalignment of the scaphoid and lunate and estimating the stage of injury.
ute to this diagnosis. can be assessed on the lateral view by mea-
The scapholunate ligament is most com- suring the scapholunate angle (Fig. 11). This Perilunate Dislocation
monly injured in the setting of a fall on an out- angle, formed by drawing a line along the vo- Background
stretched hand with most of the force centered lar margin of the scaphoid and a perpendicu- The lunate is the carpal keystone, serving
onto the thenar region [62]. Imaging plays an lar line to the volar and dorsal distal margins as the center of a network of ligaments and ar-
important complementary role to physical ex- of the lunate, normally measures between ticulations that stabilize the proximal and dis-
amination in the diagnosis of acute, subacute, 30° and 60°. An increased angle is sugges- tal carpal rows. “Perilunate dislocation” is a
and chronic scapholunate ligament injury. tive of abnormal alignment and ligamentous term that describes a continuum of carpal in-
injury. Evidence of widening on the static stability related to injury to the ligaments sur-
Imaging and dynamic imaging and rotary subluxation rounding the lunate, which result in disloca-
Radiographic evaluation is the primary im- of the scaphoid are suggestive of injury to the tion of some or all of the surrounding carpal
aging tool in all three clinical scenarios and extrinsic ligaments in addition to the scaph- bones. Perilunate, or “lesser arc,” disruption
should include posteroanterior, oblique, later- olunate ligament, a common presentation in or dislocation typically occurs in the setting of
al, and navicular views and, in some instanc- the chronic setting [65, 66]. With time, more a high-energy trauma that results in 3D load-
es, the contralateral wrist for comparison extensive tearing and degenerative change of ing: hyperextension, intercarpal supination,
[62]. These “static” views allow the evalua- the primary and secondary stabilizers result and ulnar deviation [72, 73]. The resulting
tion of fractures and alignment abnormalities. in a global disorder in the carpus, which is ligament trauma will be dependent on the de-
The radiographic findings will depend on termed “dorsal intercalated segment insta- gree of load, the dominant component of the
the degree and the chronicity of the injury. bility” and is characterized by proximal and 3D injury, and the mechanical properties of
With an isolated partial or complete tear of dorsal subluxation of the distal carpal row the ligaments [72, 73]. The rate of undetected
the scapholunate ligament, static radiographs and extension and palmar translation of the perilunate dislocation is high, with up to 25%
may appear normal because of the stabiliza- lunate [63]. missed on initial evaluation [74].
tion provided by the extrinsic ligaments [60]. MRI plays a confirmatory role in the work- Perilunate injuries typically progress in a
In this setting, the history and physical exam- up for patients with suspected scapholunate stepwise manner from the radial to the ul-
ination findings are crucial to the correct di- ligament injury. MRI reveals the compo- nar aspects of the lunate [73]. In stage I, the
agnosis and patient management. If there is a nents of the scapholunate ligament and the injury is found along the radial aspect of the
high suspicion of scapholunate ligament in- extrinsic ligaments and can provide a more wrist with tearing of the scapholunate liga-
jury, “stress” (dynamic) views should be per- detailed assessment of the extent of injury. ment resulting in scapholunate dissociation.
formed. The most common stress view is the Associated pathologic abnormalities involv- In stage II, an increased load will progress
clenched fist frontal view, which allows imag- ing the surrounding bones and articular sur- to involve the volar radioscaphocapitate lig-
ing of the wrist in a frontal position with su- faces can also be seen. MR arthrography has ament with resulting dorsal dislocation of
perimposed axial loading. This loading pro- also been shown to be an effective diagnostic the capitate and widening of the space of
vides additional stress on the joint, which is tool, in some cases better than unenhanced Poirier, known as perilunate dislocation.
thought to make it more likely to reveal scaph- MRI, for the evaluation of the scapholunate In stage III, continued loading of the wrist
olunate diastasis, defined as widening of the ligament, combining the mechanical advan- with a degree of intercarpal supination will
scapholunate interval by greater than 4 mm tages of arthrography with the detail pro- lead to tearing of the long radiolunate liga-
width at the central portion of the joint or vided by MRI [67, 68]. At this point, MRI ment and disruption of the triquetrolunate
twice as wide an interval as compared with cannot provide functional information. Ul- joint, known as midcarpal dislocation. In
other intercarpal joints, in particular the capi- trasound has also been shown to be an ac- stage IV, a persistent maximum force will
tolunate joint [63] (Fig. 10). The pencil grip curate tool in the evaluation of the scapholu- lead to disruption of the dorsal radiotrique-
posteroanterior view is another stress radio- nate ligament, with several studies showing tral ligament and rotation and palmer dislo-
graph that can reveal an occult injury. This its ability to visualize the ligament and to di- cation of the lunate from the rest of the car-
view places both wrists in pronation, adds ax- agnose pathologic abnormalities [69, 70]. pus, known as lunate dislocation.
482 AJR:203, September 2014
Errors in Reading Upper Extremity Trauma Radiographs
Imaging minimi and opponens digiti minimi). Partic- agnoses. The awareness of the specific inju-
Routine posteroanterior and lateral ra- ipants in racket and club sports, such as golf, ries presented here and an understanding of
diographs typically are all that is needed tennis, and baseball, are a population at risk their underlying pathophysiology will give
to make the correct diagnosis. The radio- for this type of injury [80, 81]. the reader the best opportunity to make the
graphic appearance of stage I is identical A fractured hook of the hamate occurs af- important imaging findings and guide appro-
to the appearance of scapholunate disso- ter direct impact or avulsion at the transcar- priate treatment.
Downloaded from www.ajronline.org by 202.80.213.249 on 08/29/19 from IP address 202.80.213.249. Copyright ARRS. For personal use only; all rights reserved
ciation. In stage II, there is disruption of pal ligament insertion [81, 82]. This can be
the arcs of Gilula along the lunate margins a difficult diagnosis to make clinically given References
on the posteroanterior view. Asymmetric the nonspecific symptoms, including chron- 1. Groh GI, Wirth MA. Management of traumatic
widening of the surrounding joint spaces ic pain along the volar or ulnar aspect of the sternoclavicular joint injuries. J Am Acad Orthop
can also be seen, in the capitolunate joint wrist, especially during a tight grip. Physical Surg 2011; 19:1–7
space in particular. The lunate maintains examination may elicit pain with palpation 2. Panzica M, Zeichen J, Hankemeier S, et al. Long-
its alignment with the radius in the lateral over the hook. term outcome after joint reconstruction or medial
view, but there is dorsal displacement of the resection arthroplasty for anterior SCJ instability.
capitate (Fig. 12). In stage III, the lunate is Imaging Arch Orthop Trauma Surg 2010; 130:657–665
completely separated from the remainder Imaging plays a crucial role in this sce- 3. Martetschläger F, Warth RJ, Millett PJ.
of the carpus. Thus, its position can vary. nario, typically beginning with postero- Instability and degenerative arthritis of the ster-
On the posteroanterior view, the findings anterior, oblique, and lateral views of the noclavicular joint: a current concepts review. Am
are similar to those seen in stage II with arc wrist. The hook may be difficult to visual- J Sports Med 2014; 42:999–1007
disruption and asymmetric joint gapping. ize on these views because of the overlap by 4. Chaudhry FA, Killampalli VV, Chowdhry M,
However, on the lateral view, the lunate is the surrounding bones. The carpal tunnel Holland P, Knebel RW. Posterior dislocation of
tilted and possibly partially subluxed volar- view, a specialized 20° supine oblique view, the sternoclavicular joint in a young rugby player.
ly, whereas the capitate is dorsally dislocat- may aid in the diagnosis because it isolates Acta Orthop Traumatol Turc 2011; 45:376–378
ed but not to the same degree as in stage the hook from the remainder of the carpus 5. Perron AD. Chest pain in athletes. Clin Sports
II. In stage IV, the lunate may have a trian- (Fig. 13). If there is persistent suspicion for Med 2003; 22:37–50
gular or “pie-shaped” appearance (this can a fracture in this location and negative ra- 6. Iannotti JP, Williams GR. Disorders of the shoul-
also be seen in earlier stages, but less often) diographs, CT should be the next imaging der: diagnosis and management. Philadelphia, PA:
on the posteroanterior view with surround- modality selected because it should reveal Lippincott Williams & Wilkins, 1999:765–813
ing arc disruption and joint gapping. On the the fracture and any associated displace- 7. Wirth MA, Rockwood CA. Disorders of the ster-
lateral view, the lunate is dislocated volarly, ment (Fig. 12). MRI could also be consid- noclavicular joint. In: The shoulder, 4th ed. Rock-
and the capitate is aligned with the radius. ered, especially if there is concern for as- wood CA Jr, Matsen FA III, Wirth MA, Lippitt
sociated ligamentous, tendinous, or ulnar SB, eds. Philadelphia, PA: Saunders Elsevier,
Long-Term Follow-Up and Complications nerve injuries. 2009: 527–560
Given the severity of injury that occurs 8. Van Holsbeeck M, Van Melkebeke J, Dequeker J,
in perilunate dislocation, prompt diagno- Long-Term Follow-Up and Complications Pennes DR. Radiographic findings of spontane-
sis and treatment are important to improve For the athlete, whether professional or ous subluxations of the sternoclavicular joint. Clin
a patient’s outcome [75]. Delays in diagnosis recreational, an undiagnosed fracture of the Rheumatol 1992; 11:376–381
and appropriate management almost invari- hook of the hamate can result in persistent 9. Lippitt S, Matsen F. Mechanism of glenohumeral
ably will result in decreased range of motion pain and chronic disability at the wrist [81]. joint stability. Clin Orthop Relat Res 1993;
and grip strength loss and in the development This can, in turn, lead to more time away 291:20–28
of posttraumatic osteoarthrosis involving the from the sport and in decreased performance 10. Abboud JA, Soslowsky LJ. Interplay of the static
radiocarpal and midcarpal joints [76–79]. on returning [83]. and dynamic restraints in glenohumeral instabili-
ty. Clin Orthop Relat Res 2002; 400:48–57
Pearls Pearls 11. Robinson CM, Seah M, Akhtar MA. The epide-
Familiarity with the normal alignment of A high index of suspicion is key to mak- miology, risk of recurrence, and functional out-
the carpal bones, specifically the arcs of Gi- ing the diagnosis of a fracture of the hook come after an acute traumatic posterior disloca-
lula on the posteroanterior and oblique views of the hamate. An awareness of the limita- tion of the shoulder. J Bone Joint Surg Am 2011;
and the radius-lunate-capitate articulation on tions of the typical wrist radiographic views 93:1605–1613
the lateral view, is crucial to the diagnosis of in evaluating the hamate is also important. 12. Kowalsky MS, Levine WN. Traumatic posterior
perilunate dislocation. When there is high suspicion for fracture, but glenohumeral dislocation: classification, pathoa-
negative radiographs, there are two options: natomy, diagnosis, and treatment. Orthop Clin
Hook of Hamate Fracture a carpal tunnel projection to help make the North Am 2008; 39:519–533
Background diagnosis or proceed directly to CT. 13. Hatzis N, Kaar TK, Wirth MA, et al. The often-
The hook of the hamate is a volar excres- overlooked posterior dislocation of the shoulder.
cence extending from the distal hamate. It Conclusion Tex Med 2001; 97:62–67
serves as an attachment site for several liga- Radiographs play an indispensable role in 14. Hawkins RJ, Neer CS 2nd, Pianta RM, et al.
ments (including the pisohamate and trans- the evaluation of patients with upper extrem- Locked posterior dislocation of the shoulder. J
carpal ligaments) and tendons (flexor digit ity trauma, especially for certain difficult di- Bone Joint Surg Am 1987; 69:9–18
AJR:203, September 2014 483
Gyftopoulos et al.
15. McLaughlin HL. Posterior dislocation of the current concepts. Injury 2008; 39:284–298 fracture. Int Orthop 1991; 15:193–196
shoulder. J Bone Joint Surg Am 1952; 24-A- 32. Lapner M, King GJ. Radial head fractures. J Bone 52. Lloyd-Roberts GC, Bucknill TM. Anterior dislo-
3:584–590 Joint Surg Am 2013; 95:1136–1143 cation of the radial head in children: aetiology,
16. Rouleau DM, Hebert-Davies J. Incidence of asso- 33. Morrey BF, Tanaka S, An KN. Valgus stability of the natural history and management. J Bone Joint
ciated injury in posterior shoulder dislocation: elbow: a definition of primary and secondary con- Surg Br 1977; 59-B:402–407
systematic review of the literature. J Orthop Trau- straints. Clin Orthop Relat Res 1991; 265:187–195 53. Ring D, Jupiter JB, Waters PM. Monteggia frac-
Downloaded from www.ajronline.org by 202.80.213.249 on 08/29/19 from IP address 202.80.213.249. Copyright ARRS. For personal use only; all rights reserved
ma 2012; 26:246–251 34. Johnson JA, Beingessner DM, Gordon KD, Dun- tures in children and adults. J Am Acad Orthop
17. Cisternino SJ, Rogers LF, Stufflebam BC, Kruglik ning CE, Stacpoole RA, King GJ. Kinematics and Surg 1998; 6:215–224
GD. The trough line: a radiographic sign of poste- stability of the fractured and implant-reconstruct- 54. Gelberman RH, Menon J. The vascularity of the
rior shoulder dislocation. AJR 1978; 130:951–954 ed radial head. J Shoulder Elbow Surg 2005; scaphoid bone. J Hand Surg Am 1980; 5:508–513
18. Yao L, Lee JK. Occult intraosseous fracture: de- 14:195S–201S 55. Dobyns JH, Linscheid RL. Fractures and disloca-
tection with MR imaging. Radiology 1988; 35. Tejwani NC, Mehta H. Fractures of the radial tions of the wrist. In: Rockwood CA Jr, Green DP,
167:749–751 head and neck: current concepts in management. J eds. Fractures in adults, 3rd ed. Philadelphia, PA:
19. Palmer WE, Brown JH, Rosenthal DI. Labral-lig- Am Acad Orthop Surg 2007; 15:380–387 Lippincott, 1984:411–509
amentous complex of the shoulder: evaluation with 36. Mason ML. Some observations on fractures of the 56. Gelberman RH, Wolock BS, Siegel DB. Fractures
MR arthrography. Radiology 1994; 190:645–651 head of the radius with a review of one hundred and non-unions of the carpal scaphoid. J Bone
20. Ogawa K, Yoshida A, Inokuchi W. Posterior shoul- cases. Br J Surg 1954; 42:123–132 Joint Surg Am 1989; 71:1560–1565
der dislocation associated with fracture of the hu- 37. Duckworth AD, Clement ND, Jenkins PJ, Aitken 57. Hansen TB, Petersen RB, Barckman J, Uhre P,
meral anatomic neck: treatment guidelines and SA, Court-Brown CM, McQueen MM. The epide- Larsen K. Cost-effectiveness of MRI in managing
long-term outcome. J Trauma 1999; 46:318–323 miology of radial head and neck fractures. J Hand suspected scaphoid fractures. J Hand Surg Eur
21. Robinson CM, Aderinto J. Posterior shoulder dis- Surg Am 2012; 37:112–119 Vol 2009; 34:627–630
locations and fracture-dislocations. J Bone Joint 38. Greenspan A, Norman A. The radial head, capi- 58. MacLennan A. The treatment of fracture of the
Surg Am 2005; 87:639–650 tellum view: useful technique in elbow trauma. carpal scaphoid and the indications for operation.
22. DePalma AF. Shoulder dislocation. In: DePalma AJR 1982; 138:1186–1188 BMJ 1911; ii:1089–1090
AF, ed. Surgery of the shoulder, 3rd ed. Philadel- 39. Einhorn TA. The cell and molecular biology of frac- 59. Vender MI, Watson HK, Wiener BD, Black DM.
phia, PA: Lippincott William & Wilkins, ture healing. Clin Orthop 1998; 355(suppl):S7–S21 Degenerative change in symptomatic scaphoid
1983:428–511 40. Furry KL, Clinkscales CM. Comminuted fractures nonunion. J Hand Surg Am 1987; 12:514–519
23. Goss TP. Scapular fractures and dislocations: di- of the radial head: arthroplasty versus internal fixa- 60. Kitay A, Wolfe SW. Scapholunate instability: cur-
agnosis and treatment. J Am Acad Orthop Surg tion. Clin Orthop Relat Res 1998; 353:40–52 rent concepts in diagnosis and management. J
1995; 3:22–33 41. Hotchkiss RN. Displaced fractures of the radial Hand Surg Am 2012; 37:2175–2196
24. Goss TP, Owens BD. Fractures of the scapula. In: head: internal fixation or excision? J Am Acad Or- 61. [No authors listed.] Definition of carpal instability:
Rockwood CA Jr, Matsen FA III, Wirth MA, Lip- thop Surg 1997; 5:1–10 The Anatomy and Biomechanics Committee of the
pitt SB, eds. The shoulder, 4th ed. Philadelphia, 42. Doornberg JN, Ring D. Coronoid fracture pat- International Federation of Societies for Surgery of
PA: Saunders Elsevier, 2009:333–335 terns. J Hand Surg Am 2006; 31:45–52 the Hand. J Hand Surg Am 1999; 24:866–867
25. Armitage BM, Wijdicks CA, Tarkin IS, et al. 43. Steinmann SP. Coronoid process fracture. J Am 62. Mayfield JK, Johnson RP, Kilcoyne RK. Carpal
Mapping of scapular fractures with three-dimen- Acad Orthop Surg 2008; 16:519–529 dislocations: pathomechanics and progressive peri-
sional computed tomography. J Bone Joint Surg 44. Hotchkiss RN. Fractures and dislocations of the lunar instability. J Hand Surg Am 1980; 5:226–241
Am 2009; 91:2222–2228 elbow. In: Rockwood CA Jr, Green DP, Bucholz 63. Gilula LA, Mann FA, Dobyns JH, Yin Y; IWI
26. Kim E, Shin HK, Kim CH. Characteristics of an RW, Heckman JD, eds. Rockwood and Green’s Terminology Committee. Wrist terminology as
isolated greater tuberosity fracture of the humer- fractures in adults, 4th ed. Philadelphia, PA: Lip- defined by the International Wrist Investigators’
us. J Orthop Sci 2005; 10:441–444 pincott-Raven, 1996:929–1024 Workshop (IWIW). J Bone Joint Surg Am 2002;
27. Bahrs C, Lingenfelter E, Fischer F, Walters EM, 45. Doornberg JN, Ring D. Fracture of the anterome- 84(suppl 1):S1–S66
Schnabel M. Mechanism of injury and morpholo- dial facet of the coronoid process. J Bone Joint 64. Walsh JJ, Berger RA, Cooney WP. Current status
gy of the greater tuberosity fracture. J Shoulder Surg Am 2006; 88:2216–2224 of scapholunate interosseous ligament injuries. J
Elbow Surg 2006; 15:140–147 46. Sebastin SJ, Chung KC. A historical report on Ric- Am Acad Orthop Surg 2002; 10:32–42
28. George MS. Fractures of the greater tuberosity of cardo Galeazzi and the management of Galeazzi 65. Lavernia CJ, Cohen MS, Taleisnik J. Treatment of
the humerus. J Am Acad Orthop Surg 2007; fractures. J Hand Surg Am 2010; 35:1870–1877 scapholunate dissociation by ligamentous repair and
15:607–613 47. Bado JL. The Monteggia lesion. Clin Orthop capsulodesis. J Hand Surg Am 1992; 17:354–359
29. Parsons BO, Klepps SJ, Miller S, Bird J, Gladstone Relat Res 1967; 50:71–86 66. Dobyns JH, Linscheid RL. A short history of the
J, Flatow E. Reliability and reproducibility of radio- 48. Perron AD, Hersh RE, Brady WJ, Keats TE. Or- wrist joint. Hand Clin 1997; 13:1–12
graphs of greater tuberosity displacement: a cadav- thopedic pitfalls in the ED: Galeazzi and Monteg- 67. Zanetti M, Bram J, Hodler J. Triangular fibrocar-
eric study. J Bone Joint Surg Am 2005; 87:58–65 gia fracture-dislocation. Am J Emerg Med 2001; tilage and intercarpal ligaments of the wrist: does
30. Castagno AA, Shuman WP, Kilcoyne RF, Haynor 19:225–228 MR arthrography improve standard MRI? J Magn
DR, Morris ME, Matsen FA. Complex fractures 49. Mikić ZD. Galeazzi fracture-dislocations. J Bone Reson Imaging 1997; 7:590–594
of the proximal humerus: role of CT in treatment. Joint Surg Am 1975; 57:1071–1080 68. Scheck RJ, Kubitzek C, Hierner R, et al. The
Radiology 1987; 165:759–762 50. Kraus B, Horne G. Galeazzi fractures. J Trauma scapholunate interosseous ligament in MR ar-
31. Gruson KI, Ruchelsman DE, Tejwani NC. Isolat- 1985; 25:1093–1095 thrography of the wrist: correlation with non-en-
ed tuberosity fractures of the proximal humerus: 51. Bhan S, Rath S. Management of the Galeazzi hanced MRI and wrist arthroscopy. Skeletal Ra-
484 AJR:203, September 2014
Errors in Reading Upper Extremity Trauma Radiographs
diol 1997; 26:263–271 perilunate injury: 3 case reports with introduction wire fixation. J Hand Surg Am 2007; 32:318–325
69. Jacobson JA, Oh E, Propeck T, Jebson PJ, Jama- of the translunate arc concept. J Hand Surg Am 79. Forli A, Courvoisier A, Wimsey S, Corcella D,
dar DA, Hayes CW. Sonography of the scapholu- 2008; 33:1770–1776 Moutet F. Perilunate dislocations and transscaph-
nate ligament in four cadaveric wrists: correlation 75. Johnson RP. The acutely injured wrist and its re- oid perilunate fracture-dislocations: a retrospec-
with MR arthrography. AJR 2002; 179:523–527 siduals. Clin Orthop Relat Res 1980; 149:33–44 tive study with minimum ten-year follow-up. J
70. Finlay K, Lee R, Friedman L. Ultrasound of in- 76. Hildebrand KA, Ross DC, Patterson SD, Roth JH, Hand Surg Am 2010; 35:62–68
Downloaded from www.ajronline.org by 202.80.213.249 on 08/29/19 from IP address 202.80.213.249. Copyright ARRS. For personal use only; all rights reserved
trinsic wrist ligament and triangular fibrocarti- MacDermid JC, King GJ. Dorsal perilunate dislo- 80. Morgan WJ, Slowman LS. Acute hand and wrist
lage injuries. Skeletal Radiol 2004; 33:85–90 cations and fracture-dislocations: questionnaire, injuries in athletes: evaluation and management. J
71. Watson HK, Ballet FL. The SLAC wrist: scaph- clinical, and radiographic evaluation. J Hand Am Acad Orthop Surg 2001; 9:389–400
olunate advanced collapse pattern of degenerative Surg Am 2000; 25:1069–1079 81. Bryan RS, Dobyns JH. Fractures of the carpal
arthritis. J Hand Surg Am 1984; 9:358–365 77. Sotereanos DG, Mitsionis GJ, Giannakopoulos PN, bones other than lunate and navicular. Clin Or-
72. Mayfield JK. Mechanism of carpal injuries. Clin Tomaino MM, Herndon JH. Perilunate dislocation thop Relat Res 1980; 149:107–111
Orthop 1980; 149:45–54 and fracture dislocation: a critical analysis of the vo- 82. Cohen MS. Fractures of the carpal bones. Hand
73. Mayfield JK. Patterns of injury to carpal liga- lar-dorsal approach. J Hand Surg Am 1997; 22:49–56 Clin 1997; 13:587–599
ments. Clin Orthop 1984; 187:36–42 78. Souer JS, Rutgers M, Andermahr J, Jupiter JB, 83. Buterbaugh GA, Brown TR, Horn PC. Ulnar-sid-
74. Bain GI, McLean JM, Turner PC, Sood A, Pour- Ring D. Perilunate fracture-dislocations of the ed wrist pain in athletes. Clin Sports Med 1998;
giezis N. Translunate fracture with associated wrist: comparison of temporary screw versus K- 17:567–583
B
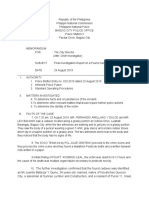
Fig. 1—19-year-old man after motor vehicle crash.
A, Portable anteroposterior radiograph of clavicles shows asymmetric widening of right sternoclavicular joint
with inferior displacement of medial aspect of right clavicle (arrow). CT was recommended for further evaluation.
B, Axial image from CT of chest with IV contrast agent shows posterior displacement of right clavicle that nears
but does not contact brachiocephalic artery (arrow).
AJR:203, September 2014 485
Gyftopoulos et al.
Fig. 2—63-year-old man with shoulder pain after fall.
A, Anteroposterior internal rotation radiograph of
shoulder shows “trough sign,” vertically oriented
linear area of sclerosis parallel to anterior cortex
(arrows), representing impaction fracture of
anterior humeral head. Glenohumeral joint appears
maintained.
B, Axillary radiograph of shoulder shows posterior
Downloaded from www.ajronline.org by 202.80.213.249 on 08/29/19 from IP address 202.80.213.249. Copyright ARRS. For personal use only; all rights reserved
dislocation of humeral head with impacted humeral
head engaged along posterior glenoid margin (curved
arrow). Major strength of axillary view is to provide
better assessment of glenohumeral joint and any
alignment abnormalities.
A B
A B C
Fig. 3—76-year-old woman with shoulder pain after
fall and dislocation.
A–C, Anteroposterior (A), scapular Y (B), and
axillary (C) radiographs of left shoulder show
evidence of prior anterior shoulder dislocation with
moderate-sized Hill-Sachs impaction deformity along
posterosuperior aspect of humeral head (arrow, C).
There is minimal cortical irregularity along coracoid
process on scapular Y view (arrow, B), which is
obscured by overlapping ribs and is not confirmed on
other two views.
D and E, Axial (D) and sagittal (E) images of left
shoulder from CT scan done on same day show
nondisplaced fracture of coracoid process (arrows).
D E
486 AJR:203, September 2014
Errors in Reading Upper Extremity Trauma Radiographs
Fig. 4—39-year-old man after fall backward down
flight of stairs.
A, Anteroposterior external rotation view of shoulder
shows linear lucency involving greater tuberosity
(arrow), representing nondisplaced fracture.
B, Coronal CT image confirms presence of
nondisplaced greater tuberosity fracture (arrow).
Downloaded from www.ajronline.org by 202.80.213.249 on 08/29/19 from IP address 202.80.213.249. Copyright ARRS. For personal use only; all rights reserved
A B
A B
Fig. 5—36-year-old man with elbow pain after
snowboarding injury 3 weeks prior.
A and B, Anteroposterior (A) and lateral (B) views
of left elbow show faint linear lucency extending
through anterolateral margin of radial articular
surface (black arrows, A and B) and large joint
effusion (gray arrows, B).
C and D, Lucency is more apparent on Greenspan
view (arrow, C) and is suggestive of mildly
impacted fracture, which is confirmed on sagittal
fat-suppressed T1-weighted image (D) from MR
arthrogram performed day after radiographs
(curved arrow).
C D
AJR:203, September 2014 487
Gyftopoulos et al.
Downloaded from www.ajronline.org by 202.80.213.249 on 08/29/19 from IP address 202.80.213.249. Copyright ARRS. For personal use only; all rights reserved
A B C
Fig. 6—63-year-old woman with history of recent fall.
A and B, Anteroposterior (A) and lateral (B) radiographs of left elbow show large joint effusion (gray arrows, B) and nondisplaced fracture through anteromedial facet of
coronoid process (black arrows, A and B).
C, Coronal fat-suppressed T2-weighted image shows nondisplaced coronoid fracture (straight black arrow) and tears of lateral capsule (white arrow) and common
extensor tendon (curved black arrow). This constellation of findings is consistent with recent episode of posteromedial elbow instability.
A B C
Fig. 7—65-year-old woman after fall.
A–C, Posteroanterior (A), oblique (B), and lateral (C) views of left wrist show mildly displaced fracture through distal third of radius (gray arrows, A–C) and nondisplaced
fracture of ulnar styloid (white arrow, A). Careful inspection of these views also shows offset of distal radioulnar joint (straight black arrows, A and B) with dorsal
displacement of distal ulna (curved arrow, C), consistent with Galeazzi fracture-dislocation.
488 AJR:203, September 2014
Errors in Reading Upper Extremity Trauma Radiographs
Fig. 8—9-year-old boy after fall.
A and B, Anteroposterior (A) and lateral (B) views of
right forearm show nondisplaced fracture through
proximal third of ulna (black arrows). Proximal radius
(white lines) does not align with capitellum (white
arrows) on either view, consistent with dislocation
and Monteggia injury.
Downloaded from www.ajronline.org by 202.80.213.249 on 08/29/19 from IP address 202.80.213.249. Copyright ARRS. For personal use only; all rights reserved
A B
A B
Fig. 9—19-year-old female volleyball player with
chronic wrist pain after fall.
A and B, Posteroanterior (A) and oblique (B) views of
left wrist show focal region of lucency surrounded
by sclerosis along medial portion of scaphoid waist
(arrows). MRI was recommended to evaluate scaphoid.
C and D, Coronal T1-weighted (C) and fat-suppressed
T2-weighted (D) images show nondisplaced complete
fracture through scaphoid waist (arrows).
C D
AJR:203, September 2014 489
Fig. 10—31-year-old man after fall with radial-sided
Gyftopoulos et al. wrist pain.
A, Posteroanterior view of right wrist shows no
fracture or abnormal alignment. Specifically,
scapholunate internal (arrow) is maintained without
offset or disproportionate widening.
B, On pencil grip view, there is diastasis of
scapholunate interval with gap measuring greater
than 4 mm (arrow). Presence of widening on
dynamic view that was not present on static view is
suggestive of injury to scapholunate ligament and not
Downloaded from www.ajronline.org by 202.80.213.249 on 08/29/19 from IP address 202.80.213.249. Copyright ARRS. For personal use only; all rights reserved
surrounding extrinsic ligaments.
A B
A B
Fig. 11—24-year-old man with scapholunate dissociation after injury during karate practice.
A, Posteroanterior “pencil grip” radiograph of bilateral wrists shows severe widening of left scapholunate interval, indicating scapholunate
diastasis (white arrow). Right scapholunate interval (black arrow) is normal.
B, Lateral view of left wrist shows scapholunate malalignment with increased dorsal tilt of lunate and volar tilt of scaphoid. Scapholunate
angle (lines) is greater than 60°, in keeping with ligamentous injury and rotatory subluxation of scaphoid.
Fig. 12—21-year-old man with wrist pain after fall.
A, Posteroanterior radiograph of wrist shows
disruption of second carpal arc (arrow) and triangular
configuration of lunate (dotted line).
B, Lateral radiograph shows volar displacement and
tilting of lunate (arrow), whereas capitate remains
aligned with radius consistent with lunate dislocation.
A B
490 AJR:203, September 2014
Errors in Reading Upper Extremity Trauma Radiographs
Downloaded from www.ajronline.org by 202.80.213.249 on 08/29/19 from IP address 202.80.213.249. Copyright ARRS. For personal use only; all rights reserved
Fig. 13—23-year-old man with hook of hamate
fracture after fall on sidewalk.
A, Posteroanterior radiograph of wrist shows
maintenance of osseous alignment. Hook of hamate
(arrow) is seen without definitive evidence for fracture.
B, Carpal tunnel view shows subtle cortical step-off
at lateral margin of base of hook of hamate (arrow),
representing nondisplaced fracture.
C, Axial CT image confirms nondisplaced fracture at
base of hook of hamate (arrow).
C
AJR:203, September 2014 491
You might also like
- Openness To Experience: Intellect & Openness: Lecture Notes 8Document8 pagesOpenness To Experience: Intellect & Openness: Lecture Notes 8Danilo Pesic100% (1)
- Airs-Lms - Math-10 - q3 - Week 3-4 Module 3 Rhonavi MasangkayDocument19 pagesAirs-Lms - Math-10 - q3 - Week 3-4 Module 3 Rhonavi MasangkayRamil J. Merculio100% (1)
- Astm D 664 - 07Document8 pagesAstm D 664 - 07Alfonso MartínezNo ratings yet
- Request For Proposal Construction & Phase 1 OperationDocument116 pagesRequest For Proposal Construction & Phase 1 Operationsobhi100% (2)
- Cell Selection ReselectionDocument35 pagesCell Selection ReselectionThiaguNo ratings yet
- Pebc CompilationDocument14 pagesPebc CompilationAarti AroraNo ratings yet
- INVENTORY MANAGEMENT TechniquesDocument24 pagesINVENTORY MANAGEMENT TechniquesWessal100% (1)
- 2010 HSC Exam PhysicsDocument42 pages2010 HSC Exam PhysicsVictor345No ratings yet
- MATHEMATICAL ECONOMICSDocument54 pagesMATHEMATICAL ECONOMICSCities Normah0% (1)
- Project Report On Evaporative CoolerDocument12 pagesProject Report On Evaporative Coolersourabh singh tomerNo ratings yet
- C-Dot Max-XlDocument39 pagesC-Dot Max-XlGourav Roy100% (3)
- Philippine Police Report Suicide InvestigationDocument2 pagesPhilippine Police Report Suicide InvestigationPAUL ALDANA82% (34)
- Extein Et Al 2017 CT Findings of Traumatic Bucket Handle Mesenteric InjuriesDocument5 pagesExtein Et Al 2017 CT Findings of Traumatic Bucket Handle Mesenteric Injuries132 Naga VamsiNo ratings yet
- CTA ExtremityDocument8 pagesCTA Extremityrio trisonaNo ratings yet
- Shoulder USG Anatomy, Technique, Scanning PitfallDocument10 pagesShoulder USG Anatomy, Technique, Scanning PitfallRonaldNo ratings yet
- What The Radiologist Needs To Know About Urolithiasis: Part 1 - Pathogenesis, Types, Assessment, and Variant AnatomyDocument8 pagesWhat The Radiologist Needs To Know About Urolithiasis: Part 1 - Pathogenesis, Types, Assessment, and Variant AnatomyQonita Aizati QomaruddinNo ratings yet
- Use Only: Non-Commercial Non-CommercialDocument8 pagesUse Only: Non-Commercial Non-CommercialNurul SevenfoldNo ratings yet
- Rotator Cuff IntervalDocument10 pagesRotator Cuff IntervalHenry J. Hernández L.No ratings yet
- Eritema Multiforme Steven Johnson y Necrolisis Epidermica Toxica. DiagnosticoDocument6 pagesEritema Multiforme Steven Johnson y Necrolisis Epidermica Toxica. DiagnosticoViejo MolinaNo ratings yet
- Journal of Cranio-Maxillo-Facial SurgeryDocument6 pagesJournal of Cranio-Maxillo-Facial SurgeryGabriel LeviNo ratings yet
- Temporomandibular: Joint Displacement Without ReductionDocument5 pagesTemporomandibular: Joint Displacement Without ReductionleandrariosllNo ratings yet
- Radiology of Chest Wall MassesDocument11 pagesRadiology of Chest Wall MassesDevina BumiNo ratings yet
- NJMS 3 2Document8 pagesNJMS 3 2anca_adam_26No ratings yet
- Radiologist, Be Aware: Ten Pitfalls That Confound The Interpretation of Multiparametric Prostate MRIDocument12 pagesRadiologist, Be Aware: Ten Pitfalls That Confound The Interpretation of Multiparametric Prostate MRITurkiNo ratings yet
- Imaging of Postpartum Complications: A Multimodality ReviewDocument12 pagesImaging of Postpartum Complications: A Multimodality ReviewGabriela Serra del CarpioNo ratings yet
- Fmed 09 926573Document17 pagesFmed 09 926573anca_adam_26No ratings yet
- Pictorial Essay: Abnormal Appendiceal PositionDocument5 pagesPictorial Essay: Abnormal Appendiceal PositionsavinaumarNo ratings yet
- Comparison of Computed Tomography With Conventional Radiography For Midfacial FracturesDocument6 pagesComparison of Computed Tomography With Conventional Radiography For Midfacial FracturesadityailhamNo ratings yet
- Pyoderma Gangrenosum A Review of Orthopedic Case ReportsDocument4 pagesPyoderma Gangrenosum A Review of Orthopedic Case ReportsIga Nurwani RidwanNo ratings yet
- Hollerman Et Al 2013 Gunshot Wounds 2 RadiologyDocument12 pagesHollerman Et Al 2013 Gunshot Wounds 2 RadiologyMathisNo ratings yet
- The Patellar Tendinopathy in Athletes A Sonographic Grading Correlated To Prognosis and TherapyDocument6 pagesThe Patellar Tendinopathy in Athletes A Sonographic Grading Correlated To Prognosis and TherapyVojtěch ŠmídNo ratings yet
- Ajr 10 7226Document9 pagesAjr 10 7226cuenta de gmailNo ratings yet
- Imaging Analyses of Bone Tumors JBJSDocument11 pagesImaging Analyses of Bone Tumors JBJSVera VeraNo ratings yet
- GCT ThumbDocument10 pagesGCT ThumbMoeez AkramNo ratings yet
- Radiographic Pitfalls in Lower Extremity Trauma: Alice S. Ha Jack A. Porrino Felix S. ChewDocument9 pagesRadiographic Pitfalls in Lower Extremity Trauma: Alice S. Ha Jack A. Porrino Felix S. Chewadi tiarmanNo ratings yet
- Mri of Bone Tumors Advances in Diagnosis and Treatment AssessmentDocument29 pagesMri of Bone Tumors Advances in Diagnosis and Treatment Assessmentlailatul husnaNo ratings yet
- A Systematic Approach To Describing FracturesDocument7 pagesA Systematic Approach To Describing FracturesAlessio CasaleNo ratings yet
- Diagnostic Imaginf of TMJ - A ReviewDocument4 pagesDiagnostic Imaginf of TMJ - A ReviewRhea RejiNo ratings yet
- Fracture of The Distal Radius: Epidemiology and Premanagement Radiographic CharacterizationDocument9 pagesFracture of The Distal Radius: Epidemiology and Premanagement Radiographic CharacterizationodivarNo ratings yet
- IMRT: A Review and Preview: Physics in Medicine & BiologyDocument18 pagesIMRT: A Review and Preview: Physics in Medicine & BiologychatsashNo ratings yet
- Chest Radiography in Thoracic Polytrauma: Mai-Lan Ho Fernando R. GutierrezDocument14 pagesChest Radiography in Thoracic Polytrauma: Mai-Lan Ho Fernando R. GutierrezenrionickolasNo ratings yet
- Atlantoaxial SubluxationDocument7 pagesAtlantoaxial SubluxationamalNo ratings yet
- Sensitivity and Specificity of Ultrasonography in Early Diagnosis of Metatarsal Bone Stress Fractures A Pilot Study of 37 PatientsDocument5 pagesSensitivity and Specificity of Ultrasonography in Early Diagnosis of Metatarsal Bone Stress Fractures A Pilot Study of 37 PatientsJUAN DIEGONo ratings yet
- Subchondroplasty What TheDocument6 pagesSubchondroplasty What TheikhsanNo ratings yet
- Diagnostics 13 01928Document30 pagesDiagnostics 13 01928fahaxa7201No ratings yet
- 8 Ramirez Spinal Cord TraumaDocument6 pages8 Ramirez Spinal Cord TraumaAllan CastroNo ratings yet
- Ajnr A5528 FullDocument9 pagesAjnr A5528 FullMehranNasrallaNo ratings yet
- Imaging of Spine Trauma: Neuroradiology Review Series Neuroradiology Review SeriesDocument17 pagesImaging of Spine Trauma: Neuroradiology Review Series Neuroradiology Review SeriesSalman Alfarisy GaulNo ratings yet
- Ankle and Foot Injuries:: Analysis of MDCT FindingsDocument8 pagesAnkle and Foot Injuries:: Analysis of MDCT FindingsraditNo ratings yet
- What Is Your Diagnosis?: in Cooperation WithDocument3 pagesWhat Is Your Diagnosis?: in Cooperation WithLinda Lineros SilvaNo ratings yet
- Pancoast Tumour Presenting As Shoulder Pain With Horner's SyndromeDocument3 pagesPancoast Tumour Presenting As Shoulder Pain With Horner's SyndromesuzilaNo ratings yet
- Unusual Mandible Fracture Caused by Metallic Spear: Case Report and Literature ReviewDocument8 pagesUnusual Mandible Fracture Caused by Metallic Spear: Case Report and Literature ReviewlindaNo ratings yet
- MRI of The Peritoneum: Spectrum of AbnormalitiesDocument12 pagesMRI of The Peritoneum: Spectrum of AbnormalitiesasfwegereNo ratings yet
- 2309499017692700Document5 pages2309499017692700calinNo ratings yet
- Nonunion UlnarDocument2 pagesNonunion UlnarSMA N 1 TOROHNo ratings yet
- 1 s2.0 S1878875020301613 MainDocument6 pages1 s2.0 S1878875020301613 MainAnyi LNo ratings yet
- Burnout, Compassion Fatigue, Compassion Satisfaction, and Secondary Traumatic Stress in Trauma NursesDocument10 pagesBurnout, Compassion Fatigue, Compassion Satisfaction, and Secondary Traumatic Stress in Trauma NursesambreenNo ratings yet
- Classification of Common Acetabular Fractures: Radiographic and CT AppearancesDocument11 pagesClassification of Common Acetabular Fractures: Radiographic and CT AppearancesGeorge MathewNo ratings yet
- Chest Radiography in Thoracic Polytrauma: Mai-Lan Ho Fernando R. GutierrezDocument14 pagesChest Radiography in Thoracic Polytrauma: Mai-Lan Ho Fernando R. GutierrezSyedNo ratings yet
- a-critical-review-of-early-burn-excision-and-grafting-1-1Document5 pagesa-critical-review-of-early-burn-excision-and-grafting-1-1petersaviocruzNo ratings yet
- Jurnal Trigeminal Neuralgia 1Document12 pagesJurnal Trigeminal Neuralgia 1nabilla putriNo ratings yet
- Intracranial NeoplasiaDocument12 pagesIntracranial NeoplasiaJamille OliveiraNo ratings yet
- Fratura mandibulaDocument9 pagesFratura mandibulaCaio GonçalvesNo ratings yet
- MRI Scanning and OrthodonticsDocument4 pagesMRI Scanning and OrthodonticsAmit SagarNo ratings yet
- Magnetic Resonance Imaging of MeningiomasDocument9 pagesMagnetic Resonance Imaging of MeningiomasElisabeth TikalakaNo ratings yet
- Trigeminal Neuralgia - A Practical GuideDocument12 pagesTrigeminal Neuralgia - A Practical Guide전영우No ratings yet
- Orthognathic Surgery and TMJ PatientsDocument14 pagesOrthognathic Surgery and TMJ PatientsDIANA PAOLA FONTECHA GONZÁLEZNo ratings yet
- Focus: Tremor, Thalamotomy, and CognitionDocument2 pagesFocus: Tremor, Thalamotomy, and CognitionRafaelNo ratings yet
- Extranodal Lymphoma From Head To Toe: Part 2, The Trunk and ExtremitiesDocument8 pagesExtranodal Lymphoma From Head To Toe: Part 2, The Trunk and ExtremitiesAlfi Qomariyah MansurNo ratings yet
- CACHEXIA Nakano Urine Titin 21Document4 pagesCACHEXIA Nakano Urine Titin 21ediNo ratings yet
- TC de Penetración AbdominopélvicaTraumaDocument18 pagesTC de Penetración AbdominopélvicaTraumaGrado CristianNo ratings yet
- MRI of the Temporomandibular Joint: Correlation Between Imaging and PathologyFrom EverandMRI of the Temporomandibular Joint: Correlation Between Imaging and PathologyTiziana RobbaNo ratings yet
- Osteoid Osteoma Contemporary ManagementDocument12 pagesOsteoid Osteoma Contemporary ManagementShahid HussainNo ratings yet
- Ajr 10 6316 PDFDocument6 pagesAjr 10 6316 PDFrasyidNo ratings yet
- Tambahan Pemeriksan Usg PD PD Mamo NegatifDocument8 pagesTambahan Pemeriksan Usg PD PD Mamo NegatifrasyidNo ratings yet
- Aturan Baru THR 2019Document12 pagesAturan Baru THR 2019rasyidNo ratings yet
- Aturan Baru THR 2019 PDFDocument1 pageAturan Baru THR 2019 PDFrasyidNo ratings yet
- Serendipity - A Sociological NoteDocument2 pagesSerendipity - A Sociological NoteAmlan BaruahNo ratings yet
- AnhvancDocument108 pagesAnhvancvanchienha7766No ratings yet
- Aerospace Opportunities in SwitzerlandDocument5 pagesAerospace Opportunities in SwitzerlandBojana DekicNo ratings yet
- Guitar Chords:: Chorus: CF CF FCFC CFGC Verse: CF CF FCFC CFGCDocument17 pagesGuitar Chords:: Chorus: CF CF FCFC CFGC Verse: CF CF FCFC CFGCKhuanZumeNo ratings yet
- Kltdensito2 PDFDocument6 pagesKltdensito2 PDFPutuWijayaKusumaNo ratings yet
- Simulia Abaqus Standard DatasheetDocument3 pagesSimulia Abaqus Standard Datasheetuser923019231831No ratings yet
- TNTCL Cost Data 2021 22Document95 pagesTNTCL Cost Data 2021 22Akd DeshmukhNo ratings yet
- Smart EE June 2022 - PackageDocument19 pagesSmart EE June 2022 - PackageMercy FeNo ratings yet
- ProjectDocument86 pagesProjectrajuNo ratings yet
- OPHTHALDocument8 pagesOPHTHALVarun ChandiramaniNo ratings yet
- Body Shaming Among School Going AdolesceDocument5 pagesBody Shaming Among School Going AdolesceClara Widya Mulya MNo ratings yet
- Telecommunications TechnicianDocument4 pagesTelecommunications Technicianapi-78381064No ratings yet
- EPISIOTOMYDocument17 pagesEPISIOTOMYKaye Arriane TenorioNo ratings yet
- Eportfile 4Document6 pagesEportfile 4api-353164003No ratings yet
- X RayDocument16 pagesX RayMedical Physics2124No ratings yet
- Oral Medication PharmacologyDocument4 pagesOral Medication PharmacologyElaisa Mae Delos SantosNo ratings yet
- Environmental Threats Differentiated Reading Comprehension Ver 1Document20 pagesEnvironmental Threats Differentiated Reading Comprehension Ver 1Camila DiasNo ratings yet
- GKInvest Market ReviewDocument66 pagesGKInvest Market ReviewjhonxracNo ratings yet