Professional Documents
Culture Documents
Imaging of Postpartum Complications: A Multimodality Review
Uploaded by
Gabriela Serra del CarpioCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Imaging of Postpartum Complications: A Multimodality Review
Uploaded by
Gabriela Serra del CarpioCopyright:
Available Formats
Wo m e n ’s I m a g i n g • R ev i ew
Plunk et al.
Imaging of Postpartum Complications
Women’s Imaging
Review
Downloaded from www.ajronline.org by 89.128.37.34 on 09/14/22 from IP address 89.128.37.34. Copyright ARRS. For personal use only; all rights reserved
Imaging of Postpartum
FOCUS ON:
Complications: A Multimodality
Review
Matthew Plunk1 OBJECTIVE. The purpose of this article is to review common and uncommon compli-
Jean H. Lee cations of postpartum and posttermination patients and their imaging findings. A variety
Kimia Kani of imaging modalities, including ultrasound, CT, MRI, and angiography, will be presented.
Majiri Dighe Knowledge of the spectrum of normal and abnormal imaging findings as well as recognition
of the common and uncommon complications are essential for accurate diagnosis.
Plunk M, Lee JH, Kani K, Dighe M CONCLUSION. Obstetric complications are a common source of morbidity and mor-
tality for women of reproductive age. Imaging, particularly with ultrasound, is often supple-
mentary to the clinical history and examination in assessing and treating women during the
postpartum period. Radiologists should be familiar with the common abnormalities that pres-
ent in this period and their imaging findings, as well as the wide range of normal appearances
the postpartum uterus can assume.
T
he postpartum period is defined as Imaging the Postpartum Uterus
beginning immediately after the The postpartum uterus typically requires
delivery of the infant and placenta 6–8 weeks to involute and return to its typ-
and typically is considered to con- ical nongravid size and appearance on ul-
tinue for 6–8 weeks as the physiologic changes trasound [7]. Although ultrasound is often
of pregnancy slowly revert to baseline. The pe- performed in this period to evaluate for ab-
riod after a spontaneous or elective abortion is normalities such as RPOC, imaging of the
less well defined, but complications are often postpartum uterus is complicated: the post-
grouped into early complications occurring partum uterus has a variable appearance,
immediately or within the first days after the and there is significant overlap between the
procedure and delayed complications occur- normal and abnormal uterus (Fig. 1). For ex-
ring beyond that time [1, 2]. ample, echogenic material is frequently seen
Keywords: accreta, cesarean, endometritis, postpartum, Pregnancy remains a major cause of mor- within the uterus in patients with bleeding,
retained products of conception tality in the 21st century in the United States. but this was found in one study not to be pre-
A recent analysis placed the pregnancy-relat- dictive of need for further intervention [8]. In
DOI:10.2214/AJR.12.9637
ed mortality rate at 14.5 deaths/100,000 live a prospective study of asymptomatic wom-
Received July 17, 2012; accepted after revision births, with more than three quarters of deaths en with physiologic levels of vaginal bleed-
September 12, 2012. occurring in the postpartum period (most com- ing after delivery, an echogenic endometri-
1
monly related to hemorrhagic or embolic con- al mass was present in half of the patients 7
All authors: Body Imaging Section, Radiology Department,
University of Washington Medical Center, 1959 NE Pacific
ditions) [3]. In addition to these life-threaten- days postpartum and in 21% of subjects at 2
St, Box 357115, Seattle, WA 98195-7115. Address ing complications, other conditions such as weeks [9]. The entire postpartum uterus can
correspondence to M. Plunk (mrplunk@uw.edu). endometritis and retained products of concep- appear hypervascular on color Doppler im-
tion (RPOC) are relatively common after birth ages, which will typically spontaneously re-
CME/SAM or termination and may require hospitalization solve without incident [10]. The presence of
This article is available for CME/SAM credit.
or additional procedures [4, 5]. Finally, almost gas within the endometrial cavity, either on
WEB one third of births in the United States are now CT or as echogenic shadowing foci on ultra-
This is a Web exclusive article. performed by cesarean section, which results sound, may also be a normal finding for sev-
in the possibility for both immediate and de- eral weeks after delivery [10, 11].
AJR 2013; 200:W143–W154
layed complications [6]. Because of their prev-
0361–803X/13/2002–W143 alence, a radiologist must be familiar with the RPOC and Postpartum Hemorrhage
various postpartum complications and the role RPOC is a nonspecific term that encom-
© American Roentgen Ray Society imaging plays in their clinical evaluation. passes residual fetal or placental tissue re-
AJR:200, February 2013 W143
Plunk et al.
maining after delivery, miscarriage, or ter- sensitivity and specificity of 79% and 89%, cently, because hypervascular masses that
mination. The frequency of RPOC has been respectively [16]. Increased color Doppler simulate the appearance of a true vascular
variably described. It most commonly occurs flow, which can also be physiologic in the malformation can develop around RPOC
with spontaneous abortions, with a frequency postpartum period, was found in the same in the endometrial cavity or myometrium.
of up to 22% [4]. However, RPOC are quite study to be more prevalent with RPOC than The possibility of a vascular malformation
uncommon after elective termination [12]. without it (79% vs 40%) (Figs. 2 and 3). An- in postpartum patients may delay curettage
Primary postpartum hemorrhage is de- other cohort study of 265 women found that for fear of provoking hemorrhage, despite a
Downloaded from www.ajronline.org by 89.128.37.34 on 09/14/22 from IP address 89.128.37.34. Copyright ARRS. For personal use only; all rights reserved
fined as blood loss greater than 500 mL after the presence of an intrauterine mass on rou- lack of definitive evidence to suggest this as
vaginal birth and greater than 1000 mL after tine postpartum ultrasound in asymptomatic a complication [25]. Conservative therapy
cesarean section. The most common cause is women with uneventful deliveries was found and observation have been suggested for sta-
an atonic uterus, which does not contract to to be predictive of future hemorrhage and the ble patients with a suspected vascular mal-
halt hemorrhage. Atony can result from nu- need for surgical intervention [17]. Howev- formation, and embolization or hysterectomy
merous causes, such as extended labor, multi- er, a smaller study did not show this result is recommended only for unstable patients.
ple gestations or a large fetus, or use of oxyto- [8]. The significance of apparent endometri- A traumatic pseudoaneurysm may appear
cin for induction or augmentation. Incomplete al stripe thickening, typically greater than 10 and behave similarly but is likewise quite
delivery of the placenta is an important cause or 13 mm, has been reported in one study to rare. Turbulent bidirectional flow within the
of uterine atony and is often suspected when be a useful indicator of RPOC [18], whereas pseudoaneurysm may resemble the Chinese-
the placenta fails to deliver, delivers incom- multiple others have not [8, 17, 19, 20]. Taoist yin and yang symbol (yin-yang sign)
pletely, or has evidence of fragmentation. The most important message regarding on color Doppler images, as pseudoaneu-
Secondary postpartum hemorrhage occurs RPOC is that no single factor has perfect positive rysms do elsewhere in the body [26].
when bleeding begins more than 24 hours af- or negative predictive values. Because both
ter delivery; it is less common than primary clinical signs and symptoms and ultrasound Interventional Radiology and Postpartum
hemorrhage but can cause significant mor- findings have high false-positive rates, being Hemorrhage
bidity and mortality [13]. RPOC is an im- conservative in diagnosing RPOC and not In cases of life-threatening postpartum
portant cause of secondary hemorrhage, and relying on a single indicator are important hemorrhage that does not respond to uterine
ultrasound is often requested for evaluation, principles that should guide reporting [21]. massage and medical therapy, the tradition-
whereas RPOC causing primary hemorrhage al method of treatment has been hysterecto-
are often suspected and treated at the time of Uncommon Causes of Hemorrhage my. Although definitive, it is an invasive pro-
delivery without imaging. Subinvolution of the placental site is a cedure that sacrifices future fertility. Uterine
Placenta accreta is a spectrum of condi- likely underrecognized cause of postpar- artery embolization is an alternative method
tions involving a placenta that is abnormally tum hemorrhage because it can be diagnosed for treatment of postpartum hemorrhage [27].
adherent to the endometrium and is an impor- only by pathologic analysis after hysterec- Embolization has been used to treat uterine
tant cause of RPOC and postpartum hemor- tomy or sufficient uterine curettage. In this atony resulting from multiple causes. Embo-
rhage [14]. Placenta accreta vera occurs when condition, even in the absence of a cause lization is the therapy of choice for rare vas-
the chorionic villi contact but do not invade such as RPOC, the uteroplacental arteries cular causes of postpartum hemorrhage, such
the myometrium, placenta increta occurs fail to regress and result in significant bleed- as uterine pseudoaneurysms and vascular
when there is myometrial invasion, and pla- ing. There may be an immunologic basis for malformations. Embolization as well as bal-
centa percreta involves invasion to or through this condition through a common mediator loon occlusion of the iliac arteries has also
the uterine serosa. Placenta accreta typically that causes these vessels to regress prema- been used in prophylaxis and treatment of
develops where there is a deficiency of the de- turely in eclampsia [22]. This condition has placenta accreta. Embolization has been re-
cidua basalis (e.g., cesarean scar) and is par- no characteristic imaging findings. ported to be efficacious in small case series,
ticularly likely in patients with placental pre- Uterine arteriovenous malformations especially when performed as a prophylactic
via or multiple cesarean sections. However, (AVMs) are an exceedingly rare cause of measure when the diagnosis is known [28,
it can also occur after termination and prior postpartum bleeding. They can be congeni- 29]. The role of balloon occlusion of the il-
uterine procedures and with advanced mater- tal or acquired as a result of hormonal stimu- iac arteries is more controversial, with vary-
nal age, uterine anomalies, Asherman syn- lation, but the most common cause is likely ing efficacy reported in the literature [30, 31].
drome, or subserosal fibroids [15]. The imag- iatrogenic. A mass in the postpartum uterus The rate of successful treatment with em-
ing of placenta accreta will be discussed in with vascularity on ultrasound is much more bolization is high (near 90%) and appears
greater detail later in this article (see the De- likely to represent RPOC than AVM. AVM to have a negligible effect on future fertil-
layed Cesarean Complications subsection). can be considered when RPOC have been ex- ity [25]. Often, uterine artery embolization
cluded and the mass is hypoechoic on B mode can successfully control hemorrhage even if
Ultrasound Appearance of RPOC images and located within the myometrium there is no evidence of active extravasation
Although it can be also be a normal post- [23] (Fig. 4). The presence of low-resistance (Fig. 5). Because uterine fibroid emboliza-
partum finding, the presence of an echogen- waveforms and peak velocities greater than tion has emerged as a modality for treatment
ic mass in the endometrium appears to be 80 cm/s have been described as features sug- of symptomatic uterine leiomyoma, interven-
the most accurate sign of RPOC, as deter- gestive of AVM over other causes [24]. tional radiologists are likely to be increasing-
mined by a retrospective review of 163 pa- Some authors think that uterine vascular ly comfortable utilizing similar techniques
tients with suspicion for RPOC that reported malformations have been overdiagnosed re- for the control of postpartum hemorrhage.
W144 AJR:200, February 2013
Imaging of Postpartum Complications
Endometritis and Postpartum ulation factors, as well as systemic up-reg- sinus thrombosis is relatively low (25–64%).
Infection ulation of plasma prothrombotic mediators. Venous sinus thrombosis should be suspected
Endometritis, or infection of the uterine This synergizes with the slowed lower ex- as a potential underlying cause of brain paren-
decidua, is the most common cause of post- tremity venous velocities that develop in the chymal abnormalities (e.g., edema or hemor-
partum fever. Although a low-grade fever third trimester to predispose patients to deep rhage) in the postpartum period [45] (Fig. 8).
is expected in the first 24 hours after vagi- vein thrombosis and pulmonary embolism Finally, amniotic fluid embolism is a rare
nal delivery or cesarean section, fever after [35]. Complications of venous thromboem- but feared complication of labor. Because of
Downloaded from www.ajronline.org by 89.128.37.34 on 09/14/22 from IP address 89.128.37.34. Copyright ARRS. For personal use only; all rights reserved
this period is suspicious for endometrial in- bolism are the leading cause of mortality of trauma to the ovarian veins during labor, am-
fection. Endometritis is more common after pregnant and recently pregnant women with- niotic fluid is able to enter the venous circu-
cesarean section, with rates up to 30 times in the developed world [36]. lation [46]. The classic clinical presentation
higher than that after spontaneous vaginal Like other changes of pregnancy, the pro- is rapid onset of shock and respiratory col-
delivery [32]. The rates are higher when pro- thrombotic state of pregnancy does not im- lapse. Chest radiographs will typically show
phylactic antibiotics are not used, such as for mediately revert to normal after delivery. new bilateral pulmonary opacities that ap-
emergent cesarean sections or some cases of The rate of pulmonary embolism has been pear similar to acute pulmonary edema.
therapeutic abortions [6, 33]. found to be highest in the postpartum peri-
Endometritis is a clinical diagnosis, but uter- od, and it requires 4 weeks for the risk of ve- Cesarean Delivery and Other
ine imaging is sometimes requested to guide nous thromboembolism to return to normal Surgical Complications
therapeutic decisions. Typically, endometritis population levels after delivery [37]. Immediate or Early Complications
is treated with broad spectrum antibiotics, but The evaluation of pregnant and postpar- As discussed earlier, the rate of cesarean
if RPOC, infected hematoma, or uterine ab- tum women with suspected pulmonary em- delivery has increased substantially in the
scess are present, evacuation may be required. bolism has been extensively discussed and past two decades and is now the most com-
Not surprisingly, the evaluation of endo- remains a controversial topic [38, 39]. In the monly performed surgical procedure in U.S.
metritis is fraught with the same issues as for postpartum period, concerns about fetal ex- hospitals [6]. The potential reasons for this
other postpartum imaging, with considerable posure to ionizing radiation or gadolinium increase include changing patient demo-
overlap between physiologic and abnormal is no longer a factor. However, ionizing ra- graphics (such as increased frequency of
findings. Patients with clinical endometritis diation exposure to actively dividing and lac- multiple births), but it is more likely a reflec-
can have normal ultrasound findings, echo- tating breast tissue remains an important is- tion of changes in patient and physician pref-
genic material within the uterus can be normal sue. Many practicing radiologists continue to erence and medicolegal concerns.
in postpartum women and may not reflect in- recommend CT angiography because of its Cesarean section has a much higher rate
fected hematoma or RPOC, and endometrial high sensitivity and specificity and its abil- of endometritis compared with vaginal de-
gas can be a normal finding for up to 3 weeks ity to evaluate for other causes of dyspnea livery, and endometritis is the most common
after delivery and does not always indicate in- or chest pain [38, 40]. However, ventilation- complication after cesarean section [47]. The
fection [34] (Fig. 6). Again, not being overly perfusion or perfusion-only scintigraphy has risks common to any surgical procedure are
reliant on or definitive according to a single advantages, including a lower dose to breast also present after cesarean section, such as
finding and integrating the imaging findings tissue [41, 42]. In addition, in pregnant pa- significant bleeding and hematoma or wound
into the complete clinical picture is crucial. tients, there is a reported higher rate of non- infection. Wound infection has been esti-
One potential but rare complication of en- diagnostic CT angiograms potentially due to mated to occur in about 5% of cases, most of
dometrial infection is pelvic septic thrombo- alterations in maternal cardiac output [43]; which will be diagnosed and treated clinical-
phlebitis. This occurs in approximately one in this could extend into the postpartum peri- ly without requiring imaging [48].
2000 deliveries and 1–2% of cases of endo- od as well. Because of this continued debate, When endometritis is diagnosed, either
metritis; it appears to be more prevalent when provider and patient preference will likely clinically or with the aid of imaging, the typ-
the infection spreads to the parametrial tis- decide which test is favored in an institution. ical treatment is antibiotics. The majority of
sues [32]. CT or MRI is preferred over ultra- Additional thrombotic complications in women will do well on this treatment, al-
sound in the evaluation of patients for whom pregnancy include ovarian vein thrombosis though a low percentage of cases (8–10%) will
conventional antibiotic therapy has failed and and thrombophlebitis, as mentioned previ- be complicated by pelvic abscess or thrombo-
who are suspected of having underlying con- ously in this article. Thrombosis of a dural phlebitis [32, 49]. A rare but feared compli-
ditions, such as septic thrombophlebitis or sinus or cerebral vein is a rare but important cation of endometrial infection is uterine rup-
an abscess. Both modalities will typically cause of postpartum headache, altered men- ture due to infection and necrosis. Analogous
show an expanded ovarian vein with internal tal status, seizure, and other neurologic symp- to infectious dehiscence of a fascial incision
thrombus (Fig. 7). Enhancement of the vessel toms and occurs more frequently in the post- or surgical anastomosis, the myometrial inci-
wall may also be present. Treatment is anti- partum period than during pregnancy [44]. sion can become infected and dehisce, result-
coagulation in addition to antibiotic therapy. These patients tend to have better outcomes ing in uterine rupture. This condition is rare,
when treated, compared with other patient with an estimated incidence of one in every
Thrombotic Complications groups with venous sinus thrombosis. CT or 700–2400 cesarean births [50]. Uterine de-
Pregnancy has long been recognized as a MR venography should be considered for the hiscence may be suspected if the discontinu-
prothrombotic state. The mechanism of this evaluation of new neurologic symptoms in the ity is felt on bimanual examination.
thrombophilia is thought to be due to in- postpartum period. The sensitivity of unen- For this condition, MRI appears to have
creased levels of fibrin and the other coag- hanced head CT for the detection of venous superior accuracy over CT, which may not be
AJR:200, February 2013 W145
Plunk et al.
able to differentiate phlegmon or abscess in weeks or months after delivery or until future well-defined borders than normal venous
the region of the scar from true dehiscence pregnancies. These complications are primar- lakes and often will show turbulent flow
[51]. Findings that have been described on ily related to the uterine scar. Although long- on color Doppler images. They have been
MRI include a lack of apposition of the en- term complications secondary to bowel or uri- described as giving the placenta a “Swiss
dometrium and serosa at the incision site and nary tract injury are possible, they are rare. cheese” or “moth-eaten” appearance. Sever-
discontinuity of the myometrium with associ- al additional signs have been described that
ated fluid collection, hematoma, or regions of Endometriosis at Cesarean Section Scar include loss of the retroplacental clear space,
Downloaded from www.ajronline.org by 89.128.37.34 on 09/14/22 from IP address 89.128.37.34. Copyright ARRS. For personal use only; all rights reserved
low signal intensity suggestive of gas. Con- Endometriosis can develop in the abdomi- gap in the retroplacental blood flow, thinning
servative management in cases of partial de- nal incision site after cesarean section (also and distortion of the myometrium, irregular-
hiscence has been proposed with some suc- known as a scar endometrioma). Scar endo- ity of the bladder-uterine interface, and bulg-
cess, but most patients undergo hysterectomy. metriosis is a rare complication with a re- ing of the placenta into the urinary bladder.
Although smaller bladder wall hematomas ported incidence ranging from 0.03% to If placenta accreta is convincing on ul-
have been seen in normal cesarean section, 1.5% [55]. However, it is still the most com- trasound, many clinicians will proceed with
the presence of large hematomas (> 5 cm) has mon manifestation of extragenital endome- cesarean section and potential hysterec-
been associated with infective uterine rup- triosis [56]. This condition can have a va- tomy. If the finding is unclear, MRI of the
ture. Although detection of uterine discon- riety of clinical presentations. Pain can be pelvis has been suggested as an alternative
tinuity has been described on ultrasound, its constant or cyclically related to the menstru- modality. The value of MRI has been vari-
sensitivity compared with that of MRI or CT al cycle. A palpable mass may or may not be ably reported: studies have shown superior
has not been established in the literature. present. Patients will often not have a history sensitivity and specificity [62] and equiva-
Intraoperative complications of cesar- of preexisting endometriosis, and delays in lent sensitivity and specificity to ultrasound,
ean section are not rare, especially when diagnosis are not rare. which may be helpful in indeterminate cas-
the indication is emergent; one study found On ultrasound, scar endometriomas can es [63], but another study failed to show that
a 12.1% rate of intraoperative complica- have a varied appearance based on size [55]. the information obtained by MRI changed
tions. The majority of these complications Small-to-moderate endometriomas in the clinical management or outcomes [64]. The
are blood loss and inadvertent injury to the abdominal wall are solid masses that have most well-described MRI findings for pla-
uterus, along with cervical lacerations; inju- less-well-defined borders and are less ho- cental invasion are bulging of the placenta
ry to the bladder, ureter, and bowel are more mogeneously hypoechoic than pelvic endo- that distorts the normal uterine contour, the
rare (≤ 1%) [52]. Patients who require peri- metriomas. As they become larger (> 3 cm), presence of dark intraplacental bands on T2-
partum hysterectomy (i.e., hysterectomy per- more cystic regions and even less-well-de- weighted images, and a heterogeneous ap-
formed immediately after a delivery or as fined borders have been described. Flow may pearance of the placenta [65] (Fig. 10).
part of a surgical delivery) need special at- be present on Doppler images in endometrio-
tention. Peripartum hysterectomy can be ei- mas of any size. Cesarean Scar Implantation or Ectopic
ther planned, as in the case of suspected ab- Pregnancy
normal placentation, or emergent, because of Postcesarean Placenta Accreta A pregnancy that develops within a pri-
bleeding complications. Peripartum hyster- The frequency of placenta accreta has or cesarean section scar has previously been
ectomy is associated with much higher rates been increasing in the last decades likely as considered one of the rarest forms of abnor-
of intraoperative bleeding, urinary tract inju- a result of increased utilization of cesarean mal implantation [66]. It has been suggest-
ries, infections, and the need for additional section. Accreta now affects one in 500 preg- ed that these are not ectopic pregnancies be-
operation or procedures [53, 54] (Fig. 9). nancies; there is a high association with pla- cause they can, in rare circumstances, be
When imaging is requested to evaluate centa previa as well [57]. Making the diag- carried to term; however, these are consid-
for postcesarean or other surgical complica- nosis of placenta accreta before the delivery ered as ectopic pregnancies for the purpose
tions, the standard contrast-enhanced CT of is crucial because it has been shown to re- of this discussion because there is implanta-
the abdomen and pelvis acquired in venous duce maternal morbidity [58, 59]. tion outside of the normal decidua and a high
phase is often sufficient if the clinical con- At the time of the fetal anatomy scan (18– rate of complications.
cern is infection. If significant abdominal as- 20 weeks), dedicated evaluation of the pla- Although rare, the incidence of cesarean
cites is known or identified on the examina- centa and lower uterine segment is suggested scar implantation appears to be increasing.
tion, obtaining a series in the excretory phase for any patient with a history of repeated ce- Again, this is likely because of the increas-
or performing a CT cystogram should be sarean sections or with placenta previa. The ing rate of cesarean delivery and increased
considered to evaluate for ureteral or blad- sensitivity of ultrasound for the detection of recognition [67]. On ultrasound, care must
der injury. If uterine dehiscence is suspected accreta has been reported to be as high as be taken to definitively identify the gesta-
either clinically or on prior CT, contrast-en- 90% [58] and as low as 30% in a small study tional sac within the low transverse incision
hanced pelvic MRI appears to be the superi- of 13 patients [60]. Several ultrasound fea- and not in the adjacent adnexa, which can
or diagnostic modality. tures have been identified to suggest placenta simulate this condition (Fig. 11). Recogni-
accreta. The most sensitive sign is the pres- tion of ectopic pregnancy within the uterus
Delayed Cesarean Complications ence of multiple placental lacunae [61]. The itself is crucial because of the risk of uterine
In addition to the complications already pathophysiology of lacunae are unknown, rupture and catastrophic bleeding.
discussed, there are complications of cesare- but they appear as hypoechoic foci that rep- Although the rate of cesarean scar ectopic
an section that may not become apparent until resent abnormal clusters of vessels with less- pregnancy appears to be increasing, defini-
W146 AJR:200, February 2013
Imaging of Postpartum Complications
tive guidelines for management have yet to be 10. Kamaya A, Ro K, Benedetti NJ, Chang PL, Dess- 25. Müngen E. Vascular abnormalities of the uterus:
outlined. A variety of treatment options have er TS. Imaging and diagnosis of postpartum com- have we recently over-diagnosed them? Ultra-
been used, ranging from observation, medical plications: sonography and other imaging modali- sound Obstet Gynecol 2003; 21:529–531
treatment either systemic or locally injected, ties. Ultrasound Q 2009; 25:151–162 26. Nanjundan P, Rohilla M, Raveendran A, Jain V,
local resection utilizing hysteroscopy or lapa- 11. Brown DL. Pelvic ultrasound in the postabortion and Khandelwal N. Pseudoaneurysm of uterine ar-
roscopy, laparotomy either for local resection postpartum patient. Ultrasound Q 2005; 21:27–37 tery: a rare cause of secondary postpartum hem-
of the gestational sac or total hysterectomy, 12. Thonneau P, Fougeyrollas B, Ducot B, et al. Com- orrhage, managed with uterine artery embolisa-
Downloaded from www.ajronline.org by 89.128.37.34 on 09/14/22 from IP address 89.128.37.34. Copyright ARRS. For personal use only; all rights reserved
treatment with uterine artery embolization, to plications of abortion performed under local anes- tion. J Clin Imaging Sci 2011; 1:14
a combination of these approaches. thesia. Eur J Obstet Gynecol Reprod Biol 1998; 27. Josephs SC. Obstetric and gynecologic emergencies:
81:59–63 a review of indications and interventional tech-
Conclusion 13. Hoveyda F, MacKenzie IZ. Secondary postpar- niques. Semin Intervent Radiol 2008; 25:337–346
The significant overlap between the patho- tum haemorrhage: incidence, morbidity and cur- 28. Diop AN, Chabrot P, Bertrand A, et al. Placenta
logic and physiologic changes of the postpar- rent management. BJOG 2001; 108:927–930 accreta: management with uterine artery emboli-
tum uterus presents many difficulties to in- 14. Oyelese Y, Smulian JC. Placenta previa, placenta zation in 17 cases. J Vasc Interv Radiol 2010;
terpreting ultrasound examinations in the accreta, and vasa previa. Obstet Gynecol 2006; 21:644–648
postpartum period. In addition, increasing 107:927–941 29. Bouvier A, Sentilhes L, Thouveny F, et al.
rates of delivery by cesarean section have the 15. Al-Serehi A, Mhoyan A, Brown M, Benirschke Planned caesarean in the interventional radiology
possibility to increase the frequency of ear- K, Hull A, Pretorius DH. Placenta accreta: an as- cath lab to enable immediate uterine artery embo-
ly and late complications. It is crucial for ra- sociation with fibroids and Asherman syndrome. J lization for the conservative treatment of placenta
diologists to be aware of the most common Ultrasound Med 2008; 27:1623–1628 accreta. Clin Radiol 2012 [Epub ahead of print]
postpartum complications on which they 16. Durfee SM, Frates MC, Luong A, Benson CB. 30. Thon S, McLintic A, Wagner Y. Prophylactic en-
will be asked to consult and the strengths The sonographic and color Doppler features of dovascular placement of internal iliac occlusion
and limitations of the various imaging mo- retained products of conception. J Ultrasound balloon catheters in parturients with placenta ac-
dalities, so that they could assist in the ap- Med 2005; 24:1181–1186 creta: a retrospective case series. Int J Obstet
propriate care of these patients. 17. Shaamash AH, Ahmed AG, Abdel Latef MM, Anesth 2011; 20:64–70
Abdullah SA. Routine postpartum ultrasonogra- 31. Dilauro MD, Dason S, Athreya S. Prophylactic
References phy in the prediction of puerperal uterine compli- balloon occlusion of internal iliac arteries in
1. Stubblefield PG, Carr-Ellis S, Borgatta L. Meth- cations. Int J Gynaecol Obstet 2007; 98:93–99 women with placenta accreta: literature review
ods for induced abortion. Obstet Gynecol 2004; 18. Ustunyurt E, Kaymak O, Iskender C, Ustunyurt OB, and analysis. Clin Radiol 2012; 67:515–520
104:174–185 Celik C, Danisman N. Role of transvaginal sonogra- 32. Maharaj D. Puerperal pyrexia: a review. Part I.
2. Mulcaire-Jones G. Complications of first-trimes- phy in the diagnosis of retained products of concep- Obstet Gynecol Surv 2007; 62:393–399
ter abortion: a report of 170,000 cases. Obstet Gy- tion. Arch Gynecol Obstet 2008; 277:151–154 33. Low N, Mueller M, Van Vliet HA, Kapp N. Peri-
necol 1990; 76:1145–1146 19. Sawyer E, Ofuasia E, Ofili-Yebovi D, Helmy S, operative antibiotics to prevent infection after
3. Berg CJ, Callaghan WM, Syverson C, Henderson Gonzalez J, Jurkovic D. The value of measuring first-trimester abortion. Cochrane Database Syst
Z. Pregnancy-related mortality in the United endometrial thickness and volume on transvagi- Rev 2012; 3:CD005217
States, 1998 to 2005. Obstet Gynecol 2010; nal ultrasound scan for the diagnosis of incom- 34. Zuckerman J, Levine D, McNicholas MM, et al.
116:1302–1309 plete miscarriage. Ultrasound Obstet Gynecol Imaging of pelvic postpartum complications. AJR
4. Sotiriadis A, Makrydimas G, Papatheodorou S, 2007; 29:205–209 1997; 168:663–668
Ioannidis JP. Expectant, medical, or surgical 20. Creinin MD, Harwood B, Guido RS, Fox MC, 35. Marik PE, Plante LA. Venous thromboembolic
management of first-trimester miscarriage: a me- Zhang J; NICHD Management of Early Pregnan- disease and pregnancy. N Engl J Med 2008;
ta-analysis. Obstet Gynecol 2005; 105:1104–1113 cy Failure Trial. Endometrial thickness after 359:2025–2033
5. Smaill F, Hofmeyr GJ. Antibiotic prophy- misoprostol use for early pregnancy failure. Int J 36. James AH, Jamison MG, Brancazio LR, Myers
laxis for cesarean section. Cochrane Database Gynaecol Obstet 2004; 86:22–26 ER. Venous thromboembolism during pregnancy
Syst Rev 2002; 3:CD000933 21. Sadan O, Golan A, Girtler O, et al. Role of sonog- and the postpartum period: incidence, risk fac-
6. Menacker F, Hamilton BE. Recent trends raphy in the diagnosis of retained products of con- tors, and mortality. Am J Obstet Gynecol 2006;
in cesarean delivery in the United States. NCHS ception. J Ultrasound Med 2004; 23:371–374 194:1311–1315
Data Brief 2010; 35:1–8 22. Weydert JA, Benda JA. Subinvolution of the pla- 37. Morris JM, Algert CS, Roberts CL. Incidence and
7. Wachsberg RH, Kurtz AB, Levine CD, Solomon cental site as an anatomic cause of postpartum risk factors for pulmonary embolism in the post-
P, Wapner RJ. Real-time ultrasonographic analy- uterine bleeding: a review. Arch Pathol Lab Med partum period. J Thromb Haemost 2010; 8:998–
sis of the normal postpartum uterus: technique, 2006; 130:1538–1542 1003
variability, and measurements. J Ultrasound Med 23. Grivell RM, Reid KM, Mellor A. Uterine arterio- 38. Wang PI, Chong ST, Kielar AZ, et al. Imaging of
1994; 13:215–221 venous malformations: a review of the current pregnant and lactating patients. Part 2: Evidence-
8. Sokol ER, Casele H, Haney EI. Ultrasound literature. Obstet Gynecol Surv 2005; 60:761–767 based review and recommendations. AJR 2012;
examination of the postpartum uterus: what is nor- 24.
Timmerman D, Wauters J, Van Calenbergh 198:785–792
mal? J Matern Fetal Neonatal Med 2004; 15:95–99 S, et al. Color Doppler imaging is a valuable tool for 39. Remy-Jardin M, Pistolesi M, Goodman LR, et al.
9. Edwards A, Ellwood DA. Ultrasonographic eval- the diagnosis and management of uterine vascular Management of suspected acute pulmonary em-
uation of the postpartum uterus. Ultrasound Ob- malformations. Ultrasound Obstet Gynecol 2003; bolism in the era of CT angiography: a statement
stet Gynecol 2000; 16:640–643 21:570–577 from the Fleischner society. Radiology 2007;
AJR:200, February 2013 W147
Plunk et al.
245:315–329 Control Hosp Epidemiol 2008; 29:477–484; discus- ings. RadioGraphics 2008; 28:1905–1916
40. Schuster ME, Fishman JE, Copeland JF, Hatabu sion, 485–486 58. Warshak CR, Ramos GA, Eskander R, et al. Ef-
H, Boiselle PM. Pulmonary embolism in pregnant 49. DePalma RT, Cunningham FG, Leveno KJ, Roark fect of predelivery diagnosis in 99 consecutive
patients: a survey of practices and policies for CT ML. Continuing investigation of women at high cases of placenta accreta. Obstet Gynecol 2010;
pulmonary angiography. AJR 2003; 181:1495– risk for infection following cesarean delivery: 115:65–69
1498 three-dose perioperative antimicrobial therapy. 59. Eller AG, Porter TF, Soisson P, Silver RM. Opti-
41. Parker MS, Hui FK, Camacho MA, Chung JK, Obstet Gynecol 1982; 60:53–59 mal management strategies for placenta accreta.
Downloaded from www.ajronline.org by 89.128.37.34 on 09/14/22 from IP address 89.128.37.34. Copyright ARRS. For personal use only; all rights reserved
Broga DW, Sethi NN. Female breast radiation ex- 50. Rivlin ME, Carroll CS Sr, Morrison JC. Infec- BJOG 2009; 116:648–654
posure during CT pulmonary angiography. AJR tious necrosis with dehiscence of the uterine re- 60. Lam G, Kuller J, McMahon M. Use of magnetic
2005; 185:1228–1233 pair complicating cesarean delivery: a review. resonance imaging and ultrasound in the antena-
42. O’Neill J, Murchison JT, Wright L, Williams J. Obstet Gynecol Surv 2004; 59:833–837 tal diagnosis of placenta accreta. J Soc Gynecol
Effect of the introduction of helical CT on radia- 51. Maldjian C, Milestone B, Schnall M, Smith R. Investig 2002; 9:37–40
tion dose in the investigation of pulmonary embo- MR appearance of uterine dehiscence in the post- 61. Comstock CH. Antenatal diagnosis of placenta
lism. Br J Radiol 2005; 78:46–50 cesarean section patient. J Comput Assist Tomogr accreta: a review. Ultrasound Obstet Gynecol
43. Ridge CA, McDermott S, Freyne BJ, Brennan DJ, 1998; 22:738–741 2005; 26:89–96
Collins CD, Skehan SJ. Pulmonary embolism in 52. Bergholt T, Stenderup JK, Vedsted-Jakobsen A, 62. Warshak CR, Eskander R, Hull AD, et al. Accu-
pregnancy: comparison of pulmonary CT angiog- Helm P, Lenstrup C. Intraoperative surgical com- racy of ultrasonography and magnetic resonance
raphy and lung scintigraphy. AJR 2009; 193:1223– plication during cesarean section: an observation- imaging in the diagnosis of placenta accreta. Ob-
1227 al study of the incidence and risk factors. Acta stet Gynecol 2006; 108:573–581
44. Cantú C, Barinagarrementeria F. Cerebral venous Obstet Gynecol Scand 2003; 82:251–256 63. Dwyer BK, Belogolovkin V, Tran L, et al. Prena-
thrombosis associated with pregnancy and puerperi- 53.
Briery CM, Rose CH, Hudson WT, et al. tal diagnosis of placenta accreta: sonography or
um: review of 67 cases. Stroke 1993; 24:1880–1884 Planned vs emergent cesarean hysterectomy. Am J magnetic resonance imaging? J Ultrasound Med
45. Linn J, Pfefferkorn T, Ivanicova K, et al. Noncon- Obst Gynecol 2007; 197:154.e1–154.e5 2008; 27:1275–1281
trast CT in deep cerebral venous thrombosis and 54. Castaneda S, Karrison T, Cibils LA. Peripartum 64. McLean LA, Heilbrun ME, Eller AG, Kennedy
sinus thrombosis: comparison of its diagnostic hysterectomy. J Perinat Med 2000; 28:472–481 AM, Woodward PJ. Assessing the role of mag-
value for both entities. AJNR 2009; 30:728–735 55. Francica G, Scarano F, Scotti L, Angelone G, netic resonance imaging in the management of
46. Han D, Lee KS, Franquet T, et al. Thrombotic and Giardiello C. Endometriomas in the region of a gravid patients at risk for placenta accreta. Acad
nonthrombotic pulmonary arterial embolism: scar from cesarean section: sonographic appear- Radiol 2011; 18:1175–1180
spectrum of imaging findings. RadioGraphics ance and clinical presentation vary with the size 65. Leyendecker JR, DuBose M, Hosseinzadeh K, et
2003; 23:1521–1539 of the lesion. J Clin Ultrasound 2009; 37:215–220 al. MRI of pregnancy-related issues: abnormal
47. Duff P. Pathophysiology and management of post- 56. Douglas C, Rotimi O. Extragenital endometriosis: placentation. AJR 2012; 198:311–320
cesarean endomyometritis. Obstet Gynecol 1986; a clinicopathological review of a Glasgow hospi- 66. Ash A, Smith A, Maxwell D. Caesarean scar
67:269–276 tal experience with case illustrations. J Obstet pregnancy. BJOG 2007; 114:253–263
48.
Olsen MA, Butler AM, Willers DM, Devkota Gynaecol 2004; 24:804–808 67. Litwicka K, Greco E. Caesarean scar pregnancy:
P, Gross GA, Fraser VJ. Risk factors for surgical site 57. Baughman WC, Corteville JE, Shah RR. Placenta a review of management options. Curr Opin Ob-
infection after low transverse cesarean section. Infect accreta: spectrum of US and MR imaging find- stet Gynecol 2011; 23:415–421
A B C
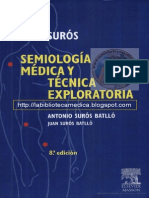
Fig. 1—Spectrum of potentially normal postpartum findings in three different patients who were treated expectantly after these examinations, with resolution of their symptoms.
A, 26-year-old woman with postpartum bleeding after spontaneous vaginal delivery. Sagittal transvaginal ultrasound shows echogenic material (arrow) in endometrial cavity.
B, 31-year-old woman with abdominal pain and bleeding after vaginal delivery. Sagittal transabdominal ultrasound shows minimally echoic fluid distending endometrial cavity.
C, 28-year-old woman with bleeding and abdominal pain 1 week after cesarean section. Contrast-enhanced CT shows that uterus is enlarged and endometrial cavity
contains mixed-density fluid and gas.
W148 AJR:200, February 2013
Imaging of Postpartum Complications
Downloaded from www.ajronline.org by 89.128.37.34 on 09/14/22 from IP address 89.128.37.34. Copyright ARRS. For personal use only; all rights reserved
A B
Fig. 2—29-year-old woman with continued bleeding after spontaneous abortion (retained products of conception).
A, Sagittal transabdominal ultrasound shows heterogeneous echogenic material expanding endometrial cavity.
B, Color Doppler sonography shows increased vascularity in anterior portion of endometrial mass (arrow), representing mix of retained products of conception anteriorly
with blood clot or necrotic placental tissue more posteriorly. Gestational trophoblastic disease was considered in differential diagnosis on ultrasound, but pathologic
examination found mixed hemorrhage and chorionic villi without fetal parts or other evidence of molar pregnancy.
Fig. 3—34-year-old woman with persistent vaginal
bleeding 4 weeks after uneventful vaginal delivery
(retained products of conception).
A, Sagittal transvaginal ultrasound confirmed
presence of echogenic material (arrow) within
endometrial cavity. Internal flow was noted with
color Doppler images (not shown).
B, Echogenic material (arrow) is also present in cervix
on coronal image. Pathologic examination after dilation
and curettage confirmed necrotic chorionic villi.
A B
AJR:200, February 2013 W149
Plunk et al.
Downloaded from www.ajronline.org by 89.128.37.34 on 09/14/22 from IP address 89.128.37.34. Copyright ARRS. For personal use only; all rights reserved
A B C
D E F
Fig. 4—Uterine arteriovenous malformation (AVM) in two different patients.
A and B, 36-year-old woman who presented with persistent hemorrhage after dilation and curettage for retained products of conception (RPOC). Transverse images from
transvaginal ultrasound (A) show echogenic material within uterine cavity, with increased flow on color Doppler sonography (B). Spectral Doppler sonography shows low-
resistance waveform and peak systolic velocity of approximately 60 cm/s (not shown). Possibility of AVM was raised. Pathologic examination after hysterectomy revealed
adherent RPOC and no AVM.
C–F, 22-year-old woman who presented with intermittent heavy vaginal bleeding 6 weeks after elective first trimester termination. Physiologic bleeding was noted in first
month after procedure, which accelerated 2 weeks before presentation. Serum β-HCG was nondetectable. Transvaginal ultrasound (C) shows clot within endometrial
cavity with eccentric vascular mass in fundus. Waveform on spectral Doppler sonography was low resistance, with peak systolic velocity greater than 90 cm/s (not
shown). Vascular malformation was suspected, and patient was referred for angiography. Multiple images from pelvic angiogram show prominent right uterine arteries
(arrow, D). Subsequently, there is vascular blush of presumed AVM in fundus (arrow, E) and then early filling of draining vein (arrow, F). This was embolized with cessation
of patient bleeding. No pathologic analysis was available to confirm vascular malformation. Although history and angiographic features were suggestive of AVM, chronic
RPOC can simulate ultrasound and angiographic appearance of AVM and cannot be excluded as reason for bleeding in this case.
W150 AJR:200, February 2013
Imaging of Postpartum Complications
Fig. 5—28-year-old woman with severe primary
postpartum hemorrhage from uterine atony after
cesarean section. Patient had 5 L of estimated
blood loss but desired future fertility and wished to
avoid hysterectomy, so catheter embolization was
performed for postpartum hemorrhage.
A, Pelvic angiogram shows increased vascularity
of postpartum uterus but with smooth diffuse
narrowing of vessels representing vasospasm from
Downloaded from www.ajronline.org by 89.128.37.34 on 09/14/22 from IP address 89.128.37.34. Copyright ARRS. For personal use only; all rights reserved
hypovolemia.
B, Superselective catheterization of right uterine
artery identified active extravasation (arrow). Right
uterine artery was successfully embolized, as was
contralateral side. Patient tolerated procedure well
with cessation of further bleeding. No hysterectomy
was required.
A B
A B
Fig. 6—34-year-old woman with retained products of conception after vaginal delivery and failed medical therapy who presented with fever and cramping.
A and B, Sagittal (A) and coronal (B) images from transvaginal ultrasound show echogenic retained products of conception and foci of higher echogenicity representing
gas (arrows) in uterus. Endometritis was suggested on imaging and confirmed clinically. Patient was treated with dilation and evacuation.
AJR:200, February 2013 W151
Plunk et al.
Downloaded from www.ajronline.org by 89.128.37.34 on 09/14/22 from IP address 89.128.37.34. Copyright ARRS. For personal use only; all rights reserved
A B
Fig. 7—41-year-old woman with abdominal pain who had spontaneous vaginal
delivery at 27 weeks’ gestation 2 weeks before presentation.
A, Axial contrast-enhanced CT image shows small filling defect (arrow) at level of
right renal vein, in expected position of right ovarian vein.
B, More inferiorly, right ovarian vein is expanded by thrombus (arrow) with mild
surrounding fat stranding.
C, Thrombus (arrow) is still present in right ovarian vein at level of ovary
(arrowhead).
A B C
Fig. 8—21-year-old woman with history of recent vaginal delivery with headache and altered mental status.
A, Unenhanced head CT was initially interpreted as normal, but in retrospect showed hyperattenuation (arrow) of straight sinus and left transverse sinus.
B, CT venogram was ordered because of concern for venous sinus thrombosis. Images confirmed thrombosis in straight and left transverse sinuses (not shown). In
addition, observe filling defect (arrow) in superior sagittal sinus.
C, T2*-weighted gradient-recalled echo MRI shows extensive susceptibility artifact in posterior fossa bilaterally due to thrombosed superficial veins.
W152 AJR:200, February 2013
Imaging of Postpartum Complications
Downloaded from www.ajronline.org by 89.128.37.34 on 09/14/22 from IP address 89.128.37.34. Copyright ARRS. For personal use only; all rights reserved
A B
Fig. 9—34-year-old woman with history of postpartum hemorrhage secondary to placenta increta requiring
emergent peripartum hysterectomy who presented after discharge 8 days after surgery with shortness of
breath and abdominal pain.
A, Abdominal CT shows large amount of abdominal ascites, which was suspected clinically to be urine.
B, Delayed CT examination obtained next morning confirmed urinary tract injury with excreted contrast agent
in peritoneal cavity.
C, Image from retrograde urogram confirms right ureteral injury with extravasation of contrast agent (arrow)
into pelvis.
Fig. 10—43-year-old woman with two prior cesarean
sections.
A, Transabdominal ultrasound shows anterior-
inferior placenta that covers internal os. Placenta
has multiple irregular peripheral hypoechoic foci
consistent with lacunae. Lacunae (arrow) extend to
bladder surface without intervening myometrium.
B, Subsequent MRI confirms findings. Additionally,
there is loss of normal bladder mucosa (arrow)
consistent with placenta percreta.
A B
AJR:200, February 2013 W153
Plunk et al.
Downloaded from www.ajronline.org by 89.128.37.34 on 09/14/22 from IP address 89.128.37.34. Copyright ARRS. For personal use only; all rights reserved
A B
Fig. 11—34-year-old woman with pelvic pain and serum β-HCG.
A, Axial transvaginal ultrasound shows gestational sac with embryo located
eccentrically within left lower uterine segment.
B, Sagittal view of endometrium shows hypoechoic scar (arrow) from patient’s
prior low transverse cesarean section.
C, Sagittal image more laterally shows gestational sac situated within scar
(arrow). Gestational sac extended into left adnexa (not shown). Implantation into
cesarean scar was confirmed on hysterectomy.
F O R YO U R I N F O R M AT I O N
This article is available for CME/SAM credit. Log onto www.arrs.org; click on AJR (in the blue Publications box);
click on the article name; add the article to the cart; proceed through the checkout process.
W154 AJR:200, February 2013
You might also like
- How to Perform Ultrasonography in EndometriosisFrom EverandHow to Perform Ultrasonography in EndometriosisStefano GuerrieroNo ratings yet
- The Histofy of ObstetrictDocument19 pagesThe Histofy of ObstetrictKathyNogalesNo ratings yet
- What The Radiologist Needs To Know About Urolithiasis: Part 1 - Pathogenesis, Types, Assessment, and Variant AnatomyDocument8 pagesWhat The Radiologist Needs To Know About Urolithiasis: Part 1 - Pathogenesis, Types, Assessment, and Variant AnatomyQonita Aizati QomaruddinNo ratings yet
- Pictorial Essay: Abnormal Appendiceal PositionDocument5 pagesPictorial Essay: Abnormal Appendiceal PositionsavinaumarNo ratings yet
- Study Nipple DischargeDocument10 pagesStudy Nipple DischargeIvana_998No ratings yet
- Ajr 17 19378Document13 pagesAjr 17 19378heryanggunNo ratings yet
- Diagnostic Procedures in Gynecology (2023)Document3 pagesDiagnostic Procedures in Gynecology (2023)RONALDO CUANo ratings yet
- Anthony 2012Document6 pagesAnthony 2012Berry BancinNo ratings yet
- Rotator Cuff IntervalDocument10 pagesRotator Cuff IntervalHenry J. Hernández L.No ratings yet
- Ajr 12 8629Document12 pagesAjr 12 8629YAŞAR TÜRKNo ratings yet
- Fetal Urinary Tract Anomalies: Review of Pathophysiology, Imaging, and ManagementDocument12 pagesFetal Urinary Tract Anomalies: Review of Pathophysiology, Imaging, and ManagementAnonymous wdmpgxNo ratings yet
- Case-Based Review and Self-Assessment Module: Radiologic Signs in Thoracic ImagingDocument15 pagesCase-Based Review and Self-Assessment Module: Radiologic Signs in Thoracic ImagingdiniNo ratings yet
- Maging of Pregnant and Lactating Patients: Part 2Document8 pagesMaging of Pregnant and Lactating Patients: Part 2Gabriela Serra del CarpioNo ratings yet
- Voiding Dysfunction: What Can Radiologists Tell Patients and Pediatric Urologists?Document10 pagesVoiding Dysfunction: What Can Radiologists Tell Patients and Pediatric Urologists?restyyulandaNo ratings yet
- Adult GliomasDocument24 pagesAdult GliomasSofía UrbinaNo ratings yet
- Common and Uncommon Applications of Bowel Ultrasound With Pathologic Correlation in ChildrenDocument14 pagesCommon and Uncommon Applications of Bowel Ultrasound With Pathologic Correlation in Childrengrahapuspa17No ratings yet
- Hernia InguinalDocument11 pagesHernia InguinalFernando BurgoaNo ratings yet
- Anatomy in SurgeryDocument8 pagesAnatomy in SurgeryBandac AlexandraNo ratings yet
- Neonatal Lung Disorders: Pattern Recognition Approach To DiagnosisDocument12 pagesNeonatal Lung Disorders: Pattern Recognition Approach To DiagnosisMeiriyani LembangNo ratings yet
- Ultrasound Imaging of Bowel Pathology - Technique and Keys To Diagnosis in The Acute Abdomen, 2011Document9 pagesUltrasound Imaging of Bowel Pathology - Technique and Keys To Diagnosis in The Acute Abdomen, 2011Сергей СадовниковNo ratings yet
- Imaging in The Post-Partum Period: Clinical Challenges, Normal Findings, and Common Imaging PitfallsDocument13 pagesImaging in The Post-Partum Period: Clinical Challenges, Normal Findings, and Common Imaging PitfallsBesse Darmita Yuana PutriNo ratings yet
- Internal Hernia AjrDocument15 pagesInternal Hernia AjrdrvijeypsgNo ratings yet
- 8 Ortho Oncology - 210217 - 194331Document11 pages8 Ortho Oncology - 210217 - 194331Nabil AhmedNo ratings yet
- Pediatric Musculoskeletal Ultrasound: Practical Imaging ApproachDocument11 pagesPediatric Musculoskeletal Ultrasound: Practical Imaging ApproachcdatNo ratings yet
- Imaging and Staging of Transitional Cell Carcinoma: Part 1, Lower Urinary TractDocument7 pagesImaging and Staging of Transitional Cell Carcinoma: Part 1, Lower Urinary TractdrelvNo ratings yet
- Translate Medscape REF 02Document2 pagesTranslate Medscape REF 02Pridina SyadirahNo ratings yet
- 30 Gibbs - Barrow Quarterly 25-1-2013Document7 pages30 Gibbs - Barrow Quarterly 25-1-2013xcskijoeNo ratings yet
- Point of Care Ultrasound: The Critical Imaging Tool For The Critically UnwellDocument10 pagesPoint of Care Ultrasound: The Critical Imaging Tool For The Critically UnwellOswaldo OrtizNo ratings yet
- Oral Radiology Principles and Interpretation 7th Ed PDFDocument14 pagesOral Radiology Principles and Interpretation 7th Ed PDFLaura Victoria Alvarez RodriguezNo ratings yet
- Diagnostic of CancerDocument27 pagesDiagnostic of CancerAyoub ZeinEddinNo ratings yet
- Muscloskeletal UsDocument9 pagesMuscloskeletal UsJERAM SINKONDENo ratings yet
- Cme Reviewarticle: Uterine Inversion: A Review of A Life-Threatening Obstetrical EmergencyDocument7 pagesCme Reviewarticle: Uterine Inversion: A Review of A Life-Threatening Obstetrical EmergencyMochHabibEl-HuseinyNo ratings yet
- Diagnostic of Cancer 1Document27 pagesDiagnostic of Cancer 1222041No ratings yet
- Ovarian Masses and O-RADS - A Systematic Approach To Evaluating and Characterizing Adnexal Masses With MRIDocument12 pagesOvarian Masses and O-RADS - A Systematic Approach To Evaluating and Characterizing Adnexal Masses With MRIDanteAugustoVazquezGonzalezNo ratings yet
- MRI of Placenta AccretaDocument8 pagesMRI of Placenta AccretabebetteryesyoucanNo ratings yet
- Mesenteric Cyst in InfancyDocument27 pagesMesenteric Cyst in InfancySpica AdharaNo ratings yet
- Artroplastia de RodillaDocument15 pagesArtroplastia de RodillaAngela TorresNo ratings yet
- AJRAmJRoentgenol 2013Aug2012W206-14Document10 pagesAJRAmJRoentgenol 2013Aug2012W206-14asdfghjm.,nmnbvcxNo ratings yet
- Glaucoma Congenital CCDocument6 pagesGlaucoma Congenital CCAllyciaNo ratings yet
- Northern California Emergency Ultrasound Course ObjectivesDocument16 pagesNorthern California Emergency Ultrasound Course ObjectivesRobert MontgomeryNo ratings yet
- Imaging of The Female Pelvis: ReviewDocument11 pagesImaging of The Female Pelvis: ReviewDian Putri NingsihNo ratings yet
- ASCCP Colposcopy Standards Role of Colposcopy,.3Document7 pagesASCCP Colposcopy Standards Role of Colposcopy,.3Laura Milagros Apóstol A.No ratings yet
- JurnalDocument7 pagesJurnalradenbagasNo ratings yet
- Jurnal 8Document13 pagesJurnal 8sriwahyuutamiNo ratings yet
- The Accuracy of Magnetic Resonance Imaging For Preoperative Deep Myometrium Assessment in Endometrial CancerDocument5 pagesThe Accuracy of Magnetic Resonance Imaging For Preoperative Deep Myometrium Assessment in Endometrial CancerDeviat Ast AmierNo ratings yet
- Corpuz, Lorelyn S - NCP (Colostomy and Ileostomy)Document3 pagesCorpuz, Lorelyn S - NCP (Colostomy and Ileostomy)Lorelyn Santos CorpuzNo ratings yet
- Efficacy and Complications of Cataract Surgery in High MyopiaDocument8 pagesEfficacy and Complications of Cataract Surgery in High MyopiaouranpisNo ratings yet
- Cervical Spine Clearance in Adult Trauma Patients.2Document5 pagesCervical Spine Clearance in Adult Trauma Patients.2Arun A MohanNo ratings yet
- RG 232025065Document21 pagesRG 232025065rulitoss_41739No ratings yet
- Prognostic Factors of Postoperative Visual Outcomes in Tuberculum Sellae MeningiomaDocument4 pagesPrognostic Factors of Postoperative Visual Outcomes in Tuberculum Sellae MeningiomaBoukhenoufa Mouhammed ElamineNo ratings yet
- Auto Article ProcessDocument6 pagesAuto Article ProcessJamshaid AhmedNo ratings yet
- Urine Dipstick Testing Everything You Need To.33Document4 pagesUrine Dipstick Testing Everything You Need To.33Brad GreyNo ratings yet
- VIBE MRI For Evaluating The Normal and Abnormal Gastrointestinal Tract in FetusesDocument6 pagesVIBE MRI For Evaluating The Normal and Abnormal Gastrointestinal Tract in FetusesakshhayaNo ratings yet
- Misses and Errors in Upper Extremity Trauma Radiographs: Soterios Gyftopoulos Munish Chitkara Jenny T. BencardinoDocument15 pagesMisses and Errors in Upper Extremity Trauma Radiographs: Soterios Gyftopoulos Munish Chitkara Jenny T. BencardinorasyidNo ratings yet
- Sonography of The Neonatal Spine: Part 2, Spinal Disorders: Lisa H. Lowe Andrew J. Johanek Charlotte W. MooreDocument6 pagesSonography of The Neonatal Spine: Part 2, Spinal Disorders: Lisa H. Lowe Andrew J. Johanek Charlotte W. MooredrmateensiddiquiNo ratings yet
- Papanikolaou Et AlDocument8 pagesPapanikolaou Et AlejiehNo ratings yet
- Diagnosis and Management of Pituitary Disease With Focus On The Role of Magnetic Resonance Imaging, 2020Document13 pagesDiagnosis and Management of Pituitary Disease With Focus On The Role of Magnetic Resonance Imaging, 2020CAMILO ARMANDO BENAVIDES BURBANONo ratings yet
- Vesicovaginal FistulaDocument54 pagesVesicovaginal FistuladanielNo ratings yet
- Jurnal B 1Document10 pagesJurnal B 1Nasayu Nadia Santika AyuNo ratings yet
- Craniopharyngioma-The Anesthetic, Critical Care and Syrgical Challenges in The Managemnet of CPNDocument5 pagesCraniopharyngioma-The Anesthetic, Critical Care and Syrgical Challenges in The Managemnet of CPNpitriaNo ratings yet
- Chronic Expanding Hematoma in The ExtremitiesDocument6 pagesChronic Expanding Hematoma in The ExtremitiesGabriela Serra del CarpioNo ratings yet
- Chronic Expanding Hematoma Following AbdominoplastyDocument4 pagesChronic Expanding Hematoma Following AbdominoplastyGabriela Serra del CarpioNo ratings yet
- Painful Suprapatellar Mass: DiscussionDocument4 pagesPainful Suprapatellar Mass: DiscussionGabriela Serra del CarpioNo ratings yet
- Hronic Expanding Hematoma of The Left FlankDocument6 pagesHronic Expanding Hematoma of The Left FlankGabriela Serra del CarpioNo ratings yet
- Extradigital Symplastic Glomus Tumor of The Hand: Report of 2 Cases and Literature ReviewDocument3 pagesExtradigital Symplastic Glomus Tumor of The Hand: Report of 2 Cases and Literature ReviewGabriela Serra del CarpioNo ratings yet
- A Pictorial Review of Postpartum ComplicationsDocument25 pagesA Pictorial Review of Postpartum ComplicationsGabriela Serra del CarpioNo ratings yet
- MR Imaging of Mater-Nal Diseases of TheAbdomen and PelvisDocument16 pagesMR Imaging of Mater-Nal Diseases of TheAbdomen and PelvisGabriela Serra del CarpioNo ratings yet
- Imaging During Pregnancy: What The Radiologist Needs To KnowDocument11 pagesImaging During Pregnancy: What The Radiologist Needs To KnowGabriela Serra del CarpioNo ratings yet
- Fundamentals of Skeletal Radiology - CompressDocument242 pagesFundamentals of Skeletal Radiology - CompressGabriela Serra del Carpio100% (1)
- Maging of Pregnant and Lactating Patients: Part 2Document8 pagesMaging of Pregnant and Lactating Patients: Part 2Gabriela Serra del CarpioNo ratings yet
- Semiologia - Suros 8°Document1,163 pagesSemiologia - Suros 8°LuisManu Zam VerNo ratings yet
- Early Onset Type 2 Diabetes: Risk Factors, Clinical Impact and ManagementDocument11 pagesEarly Onset Type 2 Diabetes: Risk Factors, Clinical Impact and ManagementMuhammad Hafidzul HairulNo ratings yet
- Forms Mental Health Act 2017Document8 pagesForms Mental Health Act 2017neethuNo ratings yet
- Effects of social distancing, self-quarantine and self-isolation on well-being during COVID-19Document9 pagesEffects of social distancing, self-quarantine and self-isolation on well-being during COVID-19naiaradafneNo ratings yet
- EMRAM Stages Model ExplainedDocument2 pagesEMRAM Stages Model ExplainedReinhard Harianja100% (1)
- Case 7 Needs Assesment 1Document54 pagesCase 7 Needs Assesment 1api-664989573No ratings yet
- Placenta Akreta Screening and DiagnosisDocument46 pagesPlacenta Akreta Screening and DiagnosisDwiweirkepPetNo ratings yet
- Ataxia TelangiectasiaDocument15 pagesAtaxia TelangiectasiaMarc Lloyd AlfonsoNo ratings yet
- Topic ProposalDocument4 pagesTopic Proposalapi-489415677No ratings yet
- Drug Abuse Prevention, Treatment, and RehabilitationDocument16 pagesDrug Abuse Prevention, Treatment, and RehabilitationNigel HopeNo ratings yet
- PLAUT-VINCENT ANGINA Borrelia Vincenti Tonsillitis PDFDocument2 pagesPLAUT-VINCENT ANGINA Borrelia Vincenti Tonsillitis PDFJosua MakerNo ratings yet
- Placental AbnormalitiesDocument7 pagesPlacental AbnormalitiesLrak SiaNo ratings yet
- Antiviral & Anthelmintic Drugs for Nursing StudentsDocument10 pagesAntiviral & Anthelmintic Drugs for Nursing StudentsG INo ratings yet
- Nursing Care Plan for Seizure DisorderDocument2 pagesNursing Care Plan for Seizure Disorderseeker009No ratings yet
- Miller, Neil Z. - Vaccine Safety Tricks and TipsDocument16 pagesMiller, Neil Z. - Vaccine Safety Tricks and TipsLeonard Michlin100% (1)
- Introduction To Health EconomicsDocument44 pagesIntroduction To Health EconomicsShuaynat PirbudagovaNo ratings yet
- Arora AKT 270 Day Programme April 2022 ExamDocument22 pagesArora AKT 270 Day Programme April 2022 ExamTomiNo ratings yet
- Supervised Consumption Services at Sheldon M. Chumir Health Centre FAQDocument4 pagesSupervised Consumption Services at Sheldon M. Chumir Health Centre FAQCTV CalgaryNo ratings yet
- InfertilitasDocument6 pagesInfertilitasmasdipoNo ratings yet
- Family Health Optima - RevisedDocument33 pagesFamily Health Optima - Revisedcuckoo1976No ratings yet
- OBSTETRICS Past Papers-1Document85 pagesOBSTETRICS Past Papers-1gm6282971No ratings yet
- Soal Final Nursing 2019-2020Document2 pagesSoal Final Nursing 2019-2020A.Tisna RamadhaniNo ratings yet
- 16.0 - OSH Requirements For People With Special Needs v3.0 English (Full Permission)Document12 pages16.0 - OSH Requirements For People With Special Needs v3.0 English (Full Permission)Amal JagadiNo ratings yet
- PFA FinalDocument44 pagesPFA FinalAL Babaran CanceranNo ratings yet
- Instructions To Disembarking CrewDocument8 pagesInstructions To Disembarking CrewNelfa Dela CruzNo ratings yet
- Azithromycin Nursing ConsiderationsDocument2 pagesAzithromycin Nursing ConsiderationsKristine YoungNo ratings yet
- Diabetes Mellit-Wps OfficeDocument8 pagesDiabetes Mellit-Wps OfficeSulthana Rasiya NNo ratings yet
- Nis Puf17 DugDocument202 pagesNis Puf17 DugbarrytayNo ratings yet
- Exposing the Opioid Epidemic Crisis in the USDocument16 pagesExposing the Opioid Epidemic Crisis in the USsepehrghfNo ratings yet
- Bangladesh College of Physicians and Surgeons (BCPS)Document2 pagesBangladesh College of Physicians and Surgeons (BCPS)Faruk HossainNo ratings yet
- Stratethon Case PDFDocument3 pagesStratethon Case PDFRajat YadavNo ratings yet