You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Citibank StatementDocument2 pagesCitibank Statementsfhui100% (2)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 50 Greyskull ConditioningDocument66 pages50 Greyskull ConditioningVicente Ambrosio Torres83% (6)
- Can People Change? - Bradford and HuckabayDocument4 pagesCan People Change? - Bradford and HuckabaysiriNo ratings yet
- Narrative Report FS2 Deployment - MillanoDocument4 pagesNarrative Report FS2 Deployment - MillanoCelyn MillanoNo ratings yet
- PPE MatrixDocument2 pagesPPE MatrixDhaval DobariyaNo ratings yet
- Patternmaking Principles 1Document22 pagesPatternmaking Principles 1SANDEEPNo ratings yet
- Example Design of Steel Roof Truss Filetype PDFDocument2 pagesExample Design of Steel Roof Truss Filetype PDFAmanda40% (10)
- Bond Valuation JiteshDocument83 pagesBond Valuation Jiteshjitesh_talesaraNo ratings yet
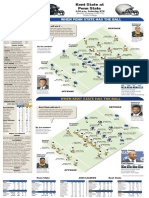
- Kent State at Penn StateDocument1 pageKent State at Penn StatedlevarseNo ratings yet
- Copy Ndsu PageDocument1 pageCopy Ndsu PageinforumdocsNo ratings yet
- Panera Bread Company Case AnalysisDocument18 pagesPanera Bread Company Case AnalysisAmmar Yahya82% (11)
- ME1202-Tutorial 2Document1 pageME1202-Tutorial 2manarajNo ratings yet
- Fequently Asked Questions (Faqs) On FcraDocument10 pagesFequently Asked Questions (Faqs) On FcraJATEENKAPADIA123No ratings yet
- Assessment of The Critically Ill Patients and Their FamiliesDocument48 pagesAssessment of The Critically Ill Patients and Their Familiesjhing_apdan100% (2)
- Instant Download Cengage Advantage Books Fundamentals of Business Law Today Summarized Cases 10th Edition Miller Test Bank PDF Full ChapterDocument33 pagesInstant Download Cengage Advantage Books Fundamentals of Business Law Today Summarized Cases 10th Edition Miller Test Bank PDF Full Chapterlilyadelaides4zo100% (13)
- Machina Arcana - Manual DraftDocument32 pagesMachina Arcana - Manual DraftgrimmNo ratings yet
- Sunrise SB9 Read OnlyDocument113 pagesSunrise SB9 Read OnlyAhmed SalahNo ratings yet
- Diamond DA42 Briefing HandoutDocument6 pagesDiamond DA42 Briefing HandoutTonyNo ratings yet
- The PAR Stock, Reorder Point and Safety Stock andDocument3 pagesThe PAR Stock, Reorder Point and Safety Stock andJorge Yeshayahu Gonzales-LaraNo ratings yet
- Kami ExportDocument9 pagesKami ExportAdam BurkeyNo ratings yet
- Naaikku Naalu Kaal Irukkalaam. Aana Adhala LOCAL Call, STD Call, ISD Call, Even MISSED Call Kooda Panna Mudiyathu!Document14 pagesNaaikku Naalu Kaal Irukkalaam. Aana Adhala LOCAL Call, STD Call, ISD Call, Even MISSED Call Kooda Panna Mudiyathu!balaengg1100% (1)
- IDS CatalogueDocument29 pagesIDS CataloguebadurallyNo ratings yet
- Bliss Manufacturing Company Internal Lab Scope: Laboratory PersonnelDocument2 pagesBliss Manufacturing Company Internal Lab Scope: Laboratory PersonnelsachNo ratings yet
- CA Final RTP Nov 2015 - CORPORATE AND ALLIED LAWSDocument58 pagesCA Final RTP Nov 2015 - CORPORATE AND ALLIED LAWSAyushNo ratings yet
- Tugas Bahasa Inggris "Roleplay Ambulation": OlehDocument3 pagesTugas Bahasa Inggris "Roleplay Ambulation": Olehnono NonoNo ratings yet
- Reviewer - Module 1: 4. Implement StrategyDocument3 pagesReviewer - Module 1: 4. Implement StrategyErika Mae LegaspiNo ratings yet
- Water Bodies Class 6Document3 pagesWater Bodies Class 6Sagar ThotaNo ratings yet
- Astm A888Document64 pagesAstm A888Nayan PatelNo ratings yet
- 2SC5200Document6 pages2SC5200Franz RamosNo ratings yet
- 201 To 243 IssuesDocument73 pages201 To 243 IssuesK Sree Harsha50% (2)