You might also like
- Signal and Systems: Ab Vaqar (COMPANY NAME) (Company Address)Document72 pagesSignal and Systems: Ab Vaqar (COMPANY NAME) (Company Address)Abdul RehmanNo ratings yet
- Fourier Transform of Discrete Time Signals: Spring 2014Document5 pagesFourier Transform of Discrete Time Signals: Spring 2014Abdul RehmanNo ratings yet
- Trigonometric Fourier Series & Fourier Series Properties: Spring 2014 Type The Document TitleDocument10 pagesTrigonometric Fourier Series & Fourier Series Properties: Spring 2014 Type The Document TitleAbdul RehmanNo ratings yet
- Lab 11Document5 pagesLab 11Abdul RehmanNo ratings yet
- Characteristics of RLC Series Ac Circuit Objective: Connect The Circuit According To Circuit DiagramDocument4 pagesCharacteristics of RLC Series Ac Circuit Objective: Connect The Circuit According To Circuit DiagramAbdul RehmanNo ratings yet
- Deep Learning in Liver Biopsies Using Convolutional Neural NetworksDocument4 pagesDeep Learning in Liver Biopsies Using Convolutional Neural NetworksAbdul RehmanNo ratings yet
- Liver Patient Classifi Cation Using Logistic RegressionDocument5 pagesLiver Patient Classifi Cation Using Logistic RegressionAbdul RehmanNo ratings yet
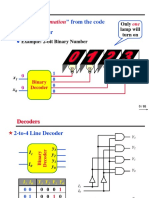
- Information: Extract " " From The Code Binary DecoderDocument6 pagesInformation: Extract " " From The Code Binary DecoderAbdul RehmanNo ratings yet
- VHDL Code MUX and DeMUX PDFDocument2 pagesVHDL Code MUX and DeMUX PDFAbdul RehmanNo ratings yet
- Combinational CircuitsDocument26 pagesCombinational CircuitsAbdul RehmanNo ratings yet
- Open Ended LabDocument2 pagesOpen Ended LabAbdul RehmanNo ratings yet
- MUX and DEMUXDocument12 pagesMUX and DEMUXAbdul RehmanNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Lebanese International University: CSCI 250 - Introduction To Programming - TEST-2: Student Name: Student IDDocument5 pagesLebanese International University: CSCI 250 - Introduction To Programming - TEST-2: Student Name: Student IDralf tamerNo ratings yet
- 6002 Notes 08 L1Document11 pages6002 Notes 08 L1Srinivasan RajenderanNo ratings yet
- KW Kwh/YrDocument3 pagesKW Kwh/YrHaris BaigNo ratings yet
- Tesis de Pared de BloquesDocument230 pagesTesis de Pared de BloquesRobert FinqNo ratings yet
- Onion Ring Magic SquareDocument8 pagesOnion Ring Magic SquareMJ Foust100% (2)
- Lecture Slides: Shigley's Mechanical Engineering DesignDocument95 pagesLecture Slides: Shigley's Mechanical Engineering DesignpurnaNo ratings yet
- Button - Head - Socket - Screws - Metric - Spec - SheetDocument1 pageButton - Head - Socket - Screws - Metric - Spec - SheetXto PeregrinNo ratings yet
- MPM2D CPT: Knights of The Night Station: Include All Your Work For Each Part On Their Own .PDF File orDocument5 pagesMPM2D CPT: Knights of The Night Station: Include All Your Work For Each Part On Their Own .PDF File orKavya Pandya100% (2)
- 01 Process CapabilityDocument33 pages01 Process CapabilitySrinivasagam Venkataramanan100% (1)
- Petroleum Formation Evaluation Questions AnswersDocument2 pagesPetroleum Formation Evaluation Questions AnswersdeusdedithaugustokiaNo ratings yet
- L05 - DumitriuDocument9 pagesL05 - DumitriuLouisaMjjNo ratings yet
- What Is Not Said: Metaphor and The Deflationary Account: Chris GenovesiDocument13 pagesWhat Is Not Said: Metaphor and The Deflationary Account: Chris GenovesimiprofesorjaviNo ratings yet
- Brochure Cementindustrie PfeifferDocument24 pagesBrochure Cementindustrie Pfeifferdoxa maria0% (1)
- Low Delay Based QSD MultiplierDocument6 pagesLow Delay Based QSD MultiplierInternational Journal of Innovative Science and Research Technology100% (2)
- Technical DataDocument246 pagesTechnical DataABDUL GHAFOORNo ratings yet
- Invers Transf LaplaceDocument13 pagesInvers Transf LaplaceMeriska AhmadNo ratings yet
- Structure HarvesterDocument3 pagesStructure HarvesterOliva R. SeguraNo ratings yet
- Revised Draft Ammendment To IRS T29 MAR13Document11 pagesRevised Draft Ammendment To IRS T29 MAR13Shipra MishraNo ratings yet
- Aveva Pdms v12.0 Sp6.25 Full Software 2014 DownloadDocument1 pageAveva Pdms v12.0 Sp6.25 Full Software 2014 DownloadMegatoreNo ratings yet
- Open-Air Theatre in The Centre of The City: Acoustic Design and Noise Environment ControlDocument3 pagesOpen-Air Theatre in The Centre of The City: Acoustic Design and Noise Environment ControlArchitectural Visualizations ArchitecturelandsNo ratings yet
- Zanussi Zou 342 User ManualDocument12 pagesZanussi Zou 342 User Manualadatok2No ratings yet
- 30 MT Tyre Mounted Crane SpecificationsDocument4 pages30 MT Tyre Mounted Crane SpecificationsramyaNo ratings yet
- Syllabus For Admission Test For Admission To Class Xi 2020-21 Physics ChemistryDocument2 pagesSyllabus For Admission Test For Admission To Class Xi 2020-21 Physics ChemistryAdhara MukherjeeNo ratings yet
- Ec1102n - Mimi Nur Nabila Binti Alias - 2019293128 - Final ExamDocument17 pagesEc1102n - Mimi Nur Nabila Binti Alias - 2019293128 - Final ExammimiNo ratings yet
- Matrix Stiffness Method EnglishDocument14 pagesMatrix Stiffness Method Englishsteam2021No ratings yet
- Carbon BlackDocument15 pagesCarbon BlackBoonyarit Lurdgrienggraiying100% (1)
- The Effects of GeoGebra Software On Pre-Service Mathematics Teachers' Attitudes and Views Toward Proof and ProvingDocument22 pagesThe Effects of GeoGebra Software On Pre-Service Mathematics Teachers' Attitudes and Views Toward Proof and ProvingLidra Ety Syahfitri Harahap lidraety.2022No ratings yet
- On Predicting Roller Milling Performance Part II. The Breakage FunctionDocument13 pagesOn Predicting Roller Milling Performance Part II. The Breakage FunctionKenneth AdamsNo ratings yet
- EO Gaddis Java Chapter 06 6e-ClassesObjectsPart2Document48 pagesEO Gaddis Java Chapter 06 6e-ClassesObjectsPart2nyle90009No ratings yet
- For More ACCA Study Materials, Tutor Support, Exam Tips VisitDocument2 pagesFor More ACCA Study Materials, Tutor Support, Exam Tips VisitNeel KostoNo ratings yet