You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Contract and Its Application On TaDocument3 pagesContract and Its Application On TasathishsayeeNo ratings yet
- Scoring Rubric OutputDocument1 pageScoring Rubric OutputNathaniel JuanNo ratings yet
- Human Diseases Detection Based On Machine Learning Algorithms: A ReviewDocument13 pagesHuman Diseases Detection Based On Machine Learning Algorithms: A Reviewmaxproooooo9No ratings yet
- Application Research On VSC-HVDC in Urban Power NetworkDocument5 pagesApplication Research On VSC-HVDC in Urban Power NetworkjorgeNo ratings yet
- Business Plan 28Document21 pagesBusiness Plan 28TintrintinNo ratings yet
- Reading 1 SlideDocument21 pagesReading 1 SlidePhương LêNo ratings yet
- New Org Chart - LNT PowerDocument1 pageNew Org Chart - LNT Powerpunitg_2No ratings yet
- NURS FPX 6414 Assessment 3 Tool Kit For BioinformaticsDocument6 pagesNURS FPX 6414 Assessment 3 Tool Kit For Bioinformaticsfarwaamjad771No ratings yet
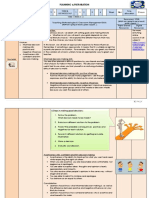
- Lesson Plan Gr. 9 Life Orientation T1 W 3&4Document4 pagesLesson Plan Gr. 9 Life Orientation T1 W 3&4jenoNo ratings yet
- Devolopment of Alternative Energy in Thailand-FinalDocument76 pagesDevolopment of Alternative Energy in Thailand-FinalsomkiatsutiratanaNo ratings yet
- Ellipse Technical OverviewDocument33 pagesEllipse Technical OverviewAlejandro MartínezNo ratings yet
- 9 IriDocument2 pages9 IriEnrique PauliniNo ratings yet
- The Premium Dilemma Page 240-245 AnalysisDocument6 pagesThe Premium Dilemma Page 240-245 AnalysisSAKSHI MORENo ratings yet
- Sociology in Modules 2Nd Edition Schaefer Test Bank Full Chapter PDFDocument54 pagesSociology in Modules 2Nd Edition Schaefer Test Bank Full Chapter PDFdandyizemanuree9nn2y100% (9)
- Cheat SheetDocument1 pageCheat SheetHinaJamilNo ratings yet
- Villanova PowerpointDocument14 pagesVillanova Powerpointapi-387888664No ratings yet
- The Derveni Papyrus: An Interim TextDocument63 pagesThe Derveni Papyrus: An Interim TextРужа ПоповаNo ratings yet
- Ajay ChauhanDocument18 pagesAjay ChauhanAjay ChauhanNo ratings yet
- The Future of Japans Tourism Full ReportDocument48 pagesThe Future of Japans Tourism Full ReportSam DyerNo ratings yet
- Problem Set Chapter 1,2 and 4Document3 pagesProblem Set Chapter 1,2 and 4audursua1025No ratings yet
- Application Form (M&Eas) : InstructionsDocument3 pagesApplication Form (M&Eas) : InstructionsHamza YousafNo ratings yet
- Case StudyDocument22 pagesCase StudyAru Verma0% (1)
- Working at Heights Step Ladder ChecklistDocument1 pageWorking at Heights Step Ladder ChecklistAku DaudNo ratings yet
- VSEPRDocument44 pagesVSEPRAhmad NaumanNo ratings yet
- MD-11 Systems Description-Aircraft GeneralDocument20 pagesMD-11 Systems Description-Aircraft GeneralJohn BallekomNo ratings yet
- Aditi Jadhav Wellness RetreatDocument17 pagesAditi Jadhav Wellness RetreatSasha BlouseNo ratings yet
- Inspection Report For HDPE Dated 07-02-2023-FSDocument1 pageInspection Report For HDPE Dated 07-02-2023-FSakshay babuNo ratings yet
- Aluminator-1000 Low ResDocument2 pagesAluminator-1000 Low ResAARON HERRERANo ratings yet
- Is 1726 1991Document17 pagesIs 1726 1991RaykochiNo ratings yet
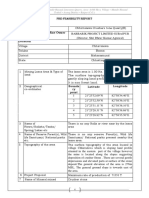
- Pre-Feasibility Report 1. Project Name of Company / Mine Owner LocationDocument10 pagesPre-Feasibility Report 1. Project Name of Company / Mine Owner Locationvarun2860No ratings yet