You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- A List of Prioritized Nursing DiagnosisDocument3 pagesA List of Prioritized Nursing DiagnosisRica DiazNo ratings yet
- AccuRay D5 - 6 Service&Installation Manual - E-5 - ' - 20190515-1 - º ¡Document209 pagesAccuRay D5 - 6 Service&Installation Manual - E-5 - ' - 20190515-1 - º ¡Trình BiomedicNo ratings yet
- Most ImportantDocument3 pagesMost ImportantVenkata Ramana Murthy Vasupilli100% (1)
- Handbook of Diabetes Technology 2019 PDFDocument125 pagesHandbook of Diabetes Technology 2019 PDFPradeep100% (1)
- Natural History of DiseaseDocument31 pagesNatural History of Diseasegabo dasNo ratings yet
- Nursing Practice I: Foundation of Nursing Practice Situation: Nursing IsDocument84 pagesNursing Practice I: Foundation of Nursing Practice Situation: Nursing Isiyoda_05100% (5)
- Affidavit: For Palarong Pambansa OnlyDocument12 pagesAffidavit: For Palarong Pambansa Onlyanno domini67% (3)
- Cac Ham ExcelDocument206 pagesCac Ham ExcelTrình BiomedicNo ratings yet
- CL-50 Plus Product Brochure-TADocument2 pagesCL-50 Plus Product Brochure-TATrình BiomedicNo ratings yet
- Công Cụ Quản Lí Rủi Ro Cho Bệnh ViệnDocument63 pagesCông Cụ Quản Lí Rủi Ro Cho Bệnh ViệnTrình BiomedicNo ratings yet
- Product Data - Accuray D6Document6 pagesProduct Data - Accuray D6Trình BiomedicNo ratings yet
- DR CatalogueDocument2 pagesDR CatalogueTrình BiomedicNo ratings yet
- HTI CL-500 Urine Analyzer: Quality Products and Service For Healthcare ProfessionalsDocument2 pagesHTI CL-500 Urine Analyzer: Quality Products and Service For Healthcare ProfessionalsTrình BiomedicNo ratings yet
- Micra MC1VR01 SpecDocument3 pagesMicra MC1VR01 SpecTrình BiomedicNo ratings yet
- CL-50 Plus Product Brochure-TADocument2 pagesCL-50 Plus Product Brochure-TATrình BiomedicNo ratings yet
- Euroanaesthesia 2015 Abstract BookDocument481 pagesEuroanaesthesia 2015 Abstract BookTrình BiomedicNo ratings yet
- Elisee 350 Product Brochure EngDocument4 pagesElisee 350 Product Brochure EngWidad Mardin Mas JayaNo ratings yet
- Nephro Gudie For HODocument22 pagesNephro Gudie For HOSarmad AsifNo ratings yet
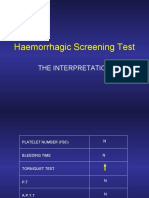
- Haemorrhagic Screening Test: The InterpretationDocument40 pagesHaemorrhagic Screening Test: The InterpretationAngel 冯晓君No ratings yet
- MoclodemideDocument1 pageMoclodemideArnzz AgbulosNo ratings yet
- Bala Murugan E - , MSC Nursing AIIMSDocument33 pagesBala Murugan E - , MSC Nursing AIIMSBalaMuruganNo ratings yet
- Labeling of The Normal Newborn at Risk, High Risk, Sick Client - GARBOSA, RMDocument4 pagesLabeling of The Normal Newborn at Risk, High Risk, Sick Client - GARBOSA, RMRej Garbosa100% (1)
- Model Answer: Important Instructions To ExaminersDocument31 pagesModel Answer: Important Instructions To Examinersmannuu00No ratings yet
- Pain Management, The Veterinary Technicians PerspectyveDocument14 pagesPain Management, The Veterinary Technicians PerspectyveClínica Veterinaria TODOVETNo ratings yet
- Logbook GIDocument15 pagesLogbook GIAna BorodinaNo ratings yet
- HazradDocument16 pagesHazradPhan AnNo ratings yet
- TOG Evolution in Screening For Down SyndromeDocument7 pagesTOG Evolution in Screening For Down SyndromeMarNo ratings yet
- Leo PlusDocument2 pagesLeo PluskbrinaldiNo ratings yet
- IvpDocument18 pagesIvpFranz SalazarNo ratings yet
- Infectious Agent Reservoir Portal of Exit Mode of Transmission Portal of Entry Susceptible HostDocument8 pagesInfectious Agent Reservoir Portal of Exit Mode of Transmission Portal of Entry Susceptible HostAldren BeliberNo ratings yet
- Burn Injury Differential DiagnosisDocument1 pageBurn Injury Differential DiagnosisAjay PhilipNo ratings yet
- Cassava Manioc HydroxiCoumarin - Scopoletin Suppresses Activation of Dendritic Cells and Pathogenesis of Experimental Autoimmune Encephalomyelitis by Inhibiting NF-κB SignalingDocument14 pagesCassava Manioc HydroxiCoumarin - Scopoletin Suppresses Activation of Dendritic Cells and Pathogenesis of Experimental Autoimmune Encephalomyelitis by Inhibiting NF-κB SignalingMiguel AngelNo ratings yet
- Neurocritical Care in The General Intensive Care UnitDocument17 pagesNeurocritical Care in The General Intensive Care UnitdanielNo ratings yet
- Polycystic Ovary Syndrome: Under Supervision ofDocument7 pagesPolycystic Ovary Syndrome: Under Supervision ofHend HamedNo ratings yet
- International HIV & AIDS Charity Donate Fundraising About AVERT AIDS Projects Help & Advice Contact Us Facebook NewsletterDocument22 pagesInternational HIV & AIDS Charity Donate Fundraising About AVERT AIDS Projects Help & Advice Contact Us Facebook NewsletterbasmashaddadNo ratings yet
- Diagnosis and Management of Late-Life Unipolar Depression - UpToDateDocument60 pagesDiagnosis and Management of Late-Life Unipolar Depression - UpToDatearthur argantaraNo ratings yet
- NURS FPX 6212 Assessment 2 Executive SummaryDocument4 pagesNURS FPX 6212 Assessment 2 Executive SummaryCarolyn HarkerNo ratings yet
- EndocrinoDocument15 pagesEndocrinoMichelle ElizaldeNo ratings yet
- CV-Alfred - AgaDocument6 pagesCV-Alfred - AgaAgostin CukajNo ratings yet
- Ce Lenk 2013Document4 pagesCe Lenk 2013RajabSaputraNo ratings yet