You might also like
- Problem-based Approach to Gastroenterology and HepatologyFrom EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNo ratings yet
- Primary Health CareDocument7 pagesPrimary Health CareJesena SalveNo ratings yet
- Philippines TB CP Guidelines 2006Document151 pagesPhilippines TB CP Guidelines 2006wiltechworksNo ratings yet
- Pediatrics:: History Taking and Physical Examination of AdolescentsDocument14 pagesPediatrics:: History Taking and Physical Examination of AdolescentsJüdith Marie Reyes BauntoNo ratings yet
- PEDIA para 08AMDocument17 pagesPEDIA para 08AMpedia blue bookNo ratings yet
- MPNST Diagnosis and TreatmentDocument27 pagesMPNST Diagnosis and TreatmentrahadiyantiNo ratings yet
- HydroceleDocument15 pagesHydroceleFernand Son Dela CruzNo ratings yet
- Difficulty Breathing Case ReportDocument6 pagesDifficulty Breathing Case ReportRaian SuyuNo ratings yet
- Blooddonation 140928122550 Phpapp02Document11 pagesBlooddonation 140928122550 Phpapp02Kranthi KonduruNo ratings yet
- PPS Orals List of Topics Case StudiesDocument3 pagesPPS Orals List of Topics Case StudiesEdna M. AtanganNo ratings yet
- Approach To The Child With Anemia - UpToDateDocument41 pagesApproach To The Child With Anemia - UpToDateDaniel Enrique CardenasNo ratings yet
- RDU On Poisoning and CancerDocument24 pagesRDU On Poisoning and CancerATHENA MINERVA MORDENONo ratings yet
- TB CPG (PPS)Document28 pagesTB CPG (PPS)Chandice CuaNo ratings yet
- Renal Failure and Pancytopenia Linked to HyperparathyroidismDocument3 pagesRenal Failure and Pancytopenia Linked to HyperparathyroidismIvan VeriswanNo ratings yet
- Beta ThalassaemiaDocument10 pagesBeta ThalassaemiaJoyce TeoNo ratings yet
- Undescended TestisDocument2 pagesUndescended TestisdyarraNo ratings yet
- Pedia DrugsDocument1 pagePedia DrugseyakoyNo ratings yet
- 2 0CommDiseaseIMPTVisionDocument3 pages2 0CommDiseaseIMPTVisionAndrea Patricia DaquialNo ratings yet
- Uti PediaDocument8 pagesUti PediaNeenya SisonNo ratings yet
- Pedia CardDocument4 pagesPedia CardPatricia Kate RegalaNo ratings yet
- Blood ComponentsDocument51 pagesBlood ComponentsMandy A. Delfin100% (1)
- Tuberculosis For Dec 1Document23 pagesTuberculosis For Dec 1Tony Rose Reataza-BaylonNo ratings yet
- PPHCH 2012Document41 pagesPPHCH 2012Jill P100% (1)
- Pediatric Neurologic Exam Primitive ReflexesDocument22 pagesPediatric Neurologic Exam Primitive ReflexesRice CookerNo ratings yet
- Acronyms and Definitions for Managing Moderate Acute MalnutritionDocument144 pagesAcronyms and Definitions for Managing Moderate Acute MalnutritionJames Abram GuardiarioNo ratings yet
- Staphylococcus Infections: Clinical Manifestations, Diagnosis and TreatmentDocument25 pagesStaphylococcus Infections: Clinical Manifestations, Diagnosis and Treatmentpedia blue bookNo ratings yet
- Osce Cranial Nerves PDFDocument42 pagesOsce Cranial Nerves PDFriczen vilaNo ratings yet
- Pediatrics 2 LaboratoryDocument40 pagesPediatrics 2 LaboratoryAmaetenNo ratings yet
- Oral Cases Study Guide - PediatricsDocument68 pagesOral Cases Study Guide - PediatricsJohn100% (1)
- Pelod 2Document14 pagesPelod 2gaatgaatNo ratings yet
- HAB ManualDocument102 pagesHAB ManualSven OrdanzaNo ratings yet
- Pulmonary Tuberculos IS: PGI Aquino Ruel Aldrin PGI Andaman Greg JinichiDocument79 pagesPulmonary Tuberculos IS: PGI Aquino Ruel Aldrin PGI Andaman Greg JinichiIggs AndamanNo ratings yet
- Gestational Trophoblastic Neoplasia TreatmentDocument75 pagesGestational Trophoblastic Neoplasia TreatmentAbdullah KesalNo ratings yet
- Physician Licensure Exam Feb 2010 Top Performing SchoolsDocument2 pagesPhysician Licensure Exam Feb 2010 Top Performing SchoolsSandy Chiong MaganitoNo ratings yet
- PSGNDocument23 pagesPSGNalpha mae beltranNo ratings yet
- Clinical Practice Guideline For CataractDocument27 pagesClinical Practice Guideline For CataractNaufal FarisatriantoNo ratings yet
- Clinical Practice Guidelines for Acute Otitis Media in ChildrenDocument45 pagesClinical Practice Guidelines for Acute Otitis Media in ChildrenJan Marvin Lichauco MendozaNo ratings yet
- CDSS Tool Detects Early Breast CancerDocument6 pagesCDSS Tool Detects Early Breast CancerJohn Mervin OliverosNo ratings yet
- Rational Drug Use Program methodology for migraine treatmentDocument3 pagesRational Drug Use Program methodology for migraine treatmentKandysse de OcampoNo ratings yet
- Congenital and Childhood Atrioventricular Blocks: Pathophysiology and Contemporary ManagementDocument14 pagesCongenital and Childhood Atrioventricular Blocks: Pathophysiology and Contemporary ManagementIvan VeriswanNo ratings yet
- Rabies Lay ForumDocument40 pagesRabies Lay ForumCarlos H. AcuñaNo ratings yet
- Common Cases in Ambulatory Care Clinic For Lu6Document106 pagesCommon Cases in Ambulatory Care Clinic For Lu6Joy SantosNo ratings yet
- Case Presentation: NeurologyDocument19 pagesCase Presentation: NeurologySydrex SarmientoNo ratings yet
- Hap VapDocument18 pagesHap VapAgita GintingNo ratings yet
- Emerging and Reemerging Infectious DiseasesDocument25 pagesEmerging and Reemerging Infectious DiseasesNorberto Francisco BaldiNo ratings yet
- Critical Appraisal RCTDocument7 pagesCritical Appraisal RCTAisya FikritamaNo ratings yet
- Fluminant Pertussis PDFDocument11 pagesFluminant Pertussis PDFDooriitha Pérez Peralta100% (1)
- ROJoson PEP Talk: COLORECTAL CANCER AWARENESSDocument54 pagesROJoson PEP Talk: COLORECTAL CANCER AWARENESSrojosonNo ratings yet
- CPG Managment of Neonatal Jaundice (Second Edition) NewDocument62 pagesCPG Managment of Neonatal Jaundice (Second Edition) NewHafiz HamidiNo ratings yet
- But Direct Antiglobulin Test-Negative Neonates Isoimmunization Is Unlikely To Be The Cause of Hemolysis in ABO-IncompatibleDocument6 pagesBut Direct Antiglobulin Test-Negative Neonates Isoimmunization Is Unlikely To Be The Cause of Hemolysis in ABO-Incompatiblelore12No ratings yet
- Thalassemias and HemoglobinopathiesDocument63 pagesThalassemias and HemoglobinopathiesMahmod_Al_Bust_4830No ratings yet
- 11.0 Pediatrics Flashcards Oct 2023Document13 pages11.0 Pediatrics Flashcards Oct 2023Shane Laika Bay DugayNo ratings yet
- Protein Energy MalnutritionDocument16 pagesProtein Energy MalnutritionAisha Abdullah ManzurNo ratings yet
- PulmoconDocument64 pagesPulmoconapi-3704562100% (1)
- Pediatric History TemplateDocument3 pagesPediatric History TemplateJoel TamayoNo ratings yet
- Nasal Cavity and Paranasal Sinuses AnatomyDocument19 pagesNasal Cavity and Paranasal Sinuses AnatomyLicensed to HealNo ratings yet
- Thesis Format IDC211Document16 pagesThesis Format IDC211Ronneil BilbaoNo ratings yet
- OBSTETRIC FORMDocument4 pagesOBSTETRIC FORMKhylamarie VillalunaNo ratings yet
- UNIT 6 - LESSON 1 - PART 3 - Pronunciation and SpeakingDocument4 pagesUNIT 6 - LESSON 1 - PART 3 - Pronunciation and SpeakingLê Thị HạnhNo ratings yet
- English K 2 Multi Age Year A Unit 1Document46 pagesEnglish K 2 Multi Age Year A Unit 1celine celineNo ratings yet
- Eating Disorders Reading AssignmentDocument2 pagesEating Disorders Reading AssignmentNasratullah sahebzadaNo ratings yet
- Tañada v. Angara Case DigestDocument12 pagesTañada v. Angara Case DigestKatrina PerezNo ratings yet
- American Ceramic: SocietyDocument8 pagesAmerican Ceramic: SocietyPhi TiêuNo ratings yet
- Women's Rights Issues and Breaking BarriersDocument2 pagesWomen's Rights Issues and Breaking BarriersMigaeaNo ratings yet
- Cebama 2016 03 D1.03 WP1 ExpStudies StateOfTheArtDocument192 pagesCebama 2016 03 D1.03 WP1 ExpStudies StateOfTheArtmihaela_filip_8No ratings yet
- Elllo Mixer #99 Do You Enjoy CookingDocument2 pagesElllo Mixer #99 Do You Enjoy CookingEnrique GarciaNo ratings yet
- REVLONDocument20 pagesREVLONUrika RufinNo ratings yet
- Comparative ResearchDocument22 pagesComparative Researchtshiringtmg7No ratings yet
- Science 5 Quiz Bee ReviewerDocument7 pagesScience 5 Quiz Bee ReviewerRommel Urbano Yabis50% (2)
- English Proficiency TrainingDocument21 pagesEnglish Proficiency TrainingDayang GNo ratings yet
- Syllabus - English (AU)Document5 pagesSyllabus - English (AU)Manasvi MehtaNo ratings yet
- Rights of Indigenous Peoples ActDocument29 pagesRights of Indigenous Peoples ActJella BandalanNo ratings yet
- Lloyd Vs Grace SmithDocument3 pagesLloyd Vs Grace SmithAkshay Bhasin60% (5)
- Unit 4.2Document69 pagesUnit 4.2ainhoa cNo ratings yet
- Cardiac Cath LabDocument2 pagesCardiac Cath Labapi-663643642No ratings yet
- Clsi Document c28 A2Document2 pagesClsi Document c28 A2Kristine Marie Pateño0% (1)
- Feasibility Studies: Presenter: Imee G. ApostolDocument35 pagesFeasibility Studies: Presenter: Imee G. ApostolKaye Anne TorresNo ratings yet
- What We Can Learn From Japanese ManagementDocument14 pagesWhat We Can Learn From Japanese Managementsinan5858No ratings yet
- Gr.8 Ch.5 Chapter Review AnswerDocument10 pagesGr.8 Ch.5 Chapter Review Answerson GokuNo ratings yet
- MOU Khusboo & NitishDocument4 pagesMOU Khusboo & NitishRimika ChauhanNo ratings yet
- SBA Observation Checklist SAMPLESDocument4 pagesSBA Observation Checklist SAMPLESPincianna WilliamsNo ratings yet
- Kolkata Thika Tenancy ActDocument15 pagesKolkata Thika Tenancy Actadv123No ratings yet
- Comparative Essay: The Sense of Closure in The Endings of A Streetcar Named Desire and Things Fall Apart - Google DocsDocument3 pagesComparative Essay: The Sense of Closure in The Endings of A Streetcar Named Desire and Things Fall Apart - Google DocsLucileNo ratings yet
- MC Sampler Pack PDFDocument195 pagesMC Sampler Pack PDFVedaste Ndayishimiye100% (2)
- Journal of Cleaner Production: Fabíola Negreiros de Oliveira, Adriana Leiras, Paula CerynoDocument15 pagesJournal of Cleaner Production: Fabíola Negreiros de Oliveira, Adriana Leiras, Paula CerynohbNo ratings yet
- Progress Test 7 PDFDocument2 pagesProgress Test 7 PDFTatiana FainaNo ratings yet
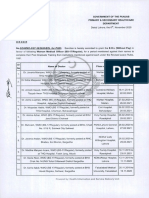
- Punjab govt grants EOL to doctors for postgraduate trainingDocument2 pagesPunjab govt grants EOL to doctors for postgraduate trainingMasroor HassanNo ratings yet
- Reena Mohamad NasirDocument122 pagesReena Mohamad NasirKedai Baju RaniaNo ratings yet