You might also like
- Forms 18 E1 & E2Document4 pagesForms 18 E1 & E2curdapia06No ratings yet
- BU F GS 14 Application For Comprehensive ExaminationDocument1 pageBU F GS 14 Application For Comprehensive Examinationmhegan07No ratings yet
- Script Late NightDocument8 pagesScript Late NightpiperNo ratings yet
- Ched E-Forms A B-C and E7Document4 pagesChed E-Forms A B-C and E7intsuya0% (1)
- 7 July - Rules The 3rd AUAP Student English Speech CompetitionDocument2 pages7 July - Rules The 3rd AUAP Student English Speech CompetitionAhmed MansoorNo ratings yet
- Acquaintance Party 2014Document3 pagesAcquaintance Party 2014John Michael MerinNo ratings yet
- Guidelines and Criteria For Poster Making ContestDocument1 pageGuidelines and Criteria For Poster Making ContestAljhon Cagaanan BacoNo ratings yet
- Mechanics Poem Recitation Contest: Criteria For JudgingDocument1 pageMechanics Poem Recitation Contest: Criteria For JudgingAbegail A. Alangue-CalimagNo ratings yet
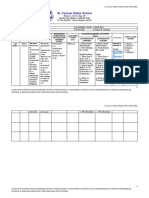
- St. Carmen Salles School: Subject: English Academic Year: 2020-2021 Grade Level: 10 Teacher Reyan B. BallasoDocument2 pagesSt. Carmen Salles School: Subject: English Academic Year: 2020-2021 Grade Level: 10 Teacher Reyan B. BallasoReyan Bantolo BallasoNo ratings yet
- Certificate of Appearance Title DefenseDocument1 pageCertificate of Appearance Title Defensecristito inovalNo ratings yet
- Contest MechanicsDocument4 pagesContest MechanicsrgjavinezNo ratings yet
- ACSCU-Accrediting Agency 2011Document35 pagesACSCU-Accrediting Agency 2011Em TyNo ratings yet
- General Education Reviewer EnglishDocument11 pagesGeneral Education Reviewer EnglishArnel Jr AmbrocioNo ratings yet
- MAED Foundations of Special Education SyllabusDocument6 pagesMAED Foundations of Special Education SyllabusBernadette Sambrano Embien100% (1)
- CS Form No. 212 Attachment Work Experience SheetDocument1 pageCS Form No. 212 Attachment Work Experience SheetLove LotsNo ratings yet
- Ms. Mythical Icon 2016: Posted by OnDocument11 pagesMs. Mythical Icon 2016: Posted by OnRodalyn May LacpaoNo ratings yet
- Annex 1 HG Class Observation Tool Sample SY 2021 2022Document3 pagesAnnex 1 HG Class Observation Tool Sample SY 2021 2022Bernardo MacaranasNo ratings yet
- Call To Order ScriptDocument1 pageCall To Order ScriptLOUISE ANNE NAGAL100% (1)
- Education System in Philippines and HongkongDocument24 pagesEducation System in Philippines and HongkongTeofian Amparo LuibNo ratings yet
- Stand Up and Deliver MechanicsDocument2 pagesStand Up and Deliver MechanicsJakie Ubina100% (1)
- Application & Mechanics For Harana Competition 2016Document3 pagesApplication & Mechanics For Harana Competition 2016LesterSanchezCuevaNo ratings yet
- Citizen's Charter - VSU Garden Beach ResortDocument3 pagesCitizen's Charter - VSU Garden Beach ResortvisayasstateuNo ratings yet
- Pinoy HenyoDocument2 pagesPinoy HenyoChabibot GalopeNo ratings yet
- The Tertiary Education Subsidy (TES) Status Form For Student Grantees in MIMAROPADocument3 pagesThe Tertiary Education Subsidy (TES) Status Form For Student Grantees in MIMAROPAKarenn Estrañero Luzon100% (1)
- SHS VP Processing of Billing Documents and Monitoring of SchoolsDocument27 pagesSHS VP Processing of Billing Documents and Monitoring of Schoolsolpccsan manuelNo ratings yet
- Letter of Academic Concern: Yolanda T. ReyesDocument2 pagesLetter of Academic Concern: Yolanda T. ReyesStBernadette DivineAcademy100% (1)
- Form 138 Sf9 BackDocument1 pageForm 138 Sf9 BackMaestro GallaNo ratings yet
- SG-2 Status Report in Early Grades EducationDocument7 pagesSG-2 Status Report in Early Grades EducationcarolynNo ratings yet
- ECCD Checklist SampleDocument2 pagesECCD Checklist SampleAginaya Dinumla-CabanayanNo ratings yet
- School Form 4 Monthly Learners' Movement and Attendance For Senior High School (SF4-SHS)Document32 pagesSchool Form 4 Monthly Learners' Movement and Attendance For Senior High School (SF4-SHS)Japeth PurisimaNo ratings yet
- A Tracer Study On The 2019-2021 Graduates of Bachelor of Arts in Community Development Program of Iloilo Science and Technology UniversityDocument8 pagesA Tracer Study On The 2019-2021 Graduates of Bachelor of Arts in Community Development Program of Iloilo Science and Technology UniversityPsychology and Education: A Multidisciplinary JournalNo ratings yet
- The Philippine Informal Reading Inventory (2018) .Pptx4Document17 pagesThe Philippine Informal Reading Inventory (2018) .Pptx4Ařčhäńgël KäśtïelNo ratings yet
- Room Assignment Occidental Mindoro (LET)Document65 pagesRoom Assignment Occidental Mindoro (LET)TheSummitExpressNo ratings yet
- 2020 - Certificate of Enrolment and Attendance CompletionDocument1 page2020 - Certificate of Enrolment and Attendance CompletionMichael LumanogNo ratings yet
- Program For GraduationDocument3 pagesProgram For Graduationzero kakumaruNo ratings yet
- Academic Integrity and Non Disclosure AgreementDocument1 pageAcademic Integrity and Non Disclosure AgreementAubrey BorjaNo ratings yet
- MR - Ms - IntramuralsDocument5 pagesMR - Ms - IntramuralsIvy May Baterna100% (1)
- DAILY LESSON LOG in English 2nd Week 2nd QuarterDocument6 pagesDAILY LESSON LOG in English 2nd Week 2nd QuarterTyron KimNo ratings yet
- Toga Rental LetterDocument1 pageToga Rental LetterPrincess EscovidalNo ratings yet
- Reflection PNUDocument2 pagesReflection PNUJohn Carlo DomantayNo ratings yet
- English DLP FormatDocument2 pagesEnglish DLP FormatPaula ParkNo ratings yet
- Fact and Opinion Lesson PlanDocument2 pagesFact and Opinion Lesson Planapi-247211131100% (1)
- LDM 2 Submission Links and Evaluation GuideDocument12 pagesLDM 2 Submission Links and Evaluation GuideLynji PedrosaNo ratings yet
- Campus Journalism and Its Effects On Daily Life AntipuestoDocument5 pagesCampus Journalism and Its Effects On Daily Life AntipuestoMar Angelo FlorescaNo ratings yet
- Demo Teaching CriteriaDocument1 pageDemo Teaching CriteriaRoshio Tsuyu TejidoNo ratings yet
- RUBRICSDocument2 pagesRUBRICSAndreigh A. AradaNo ratings yet
- Graduation Exercises SY 2015-2016Document1 pageGraduation Exercises SY 2015-2016Resa Consigna MagusaraNo ratings yet
- Navarro Jan Albert Reaction Paper Japanese Educational SystemDocument3 pagesNavarro Jan Albert Reaction Paper Japanese Educational SystemAbet NavarroNo ratings yet
- Mr. & Mrs. Danilo M. Manabat: Foundation DAY AnniversaryDocument2 pagesMr. & Mrs. Danilo M. Manabat: Foundation DAY AnniversaryGem Lam SenNo ratings yet
- Ambahan Digi Photog Rubric 2019-2020 - 4n1Document1 pageAmbahan Digi Photog Rubric 2019-2020 - 4n1Benjamin Medina100% (1)
- CriteriaDocument1 pageCriteriaPark SungNo ratings yet
- Budget of Work For Gr.5Document19 pagesBudget of Work For Gr.5Mathew Angelo Perez GamboaNo ratings yet
- BSCS New CurriculumDocument3 pagesBSCS New CurriculumLex Acads100% (1)
- Annual Physical Checking of Property Furniture and Equipment Dep EDDocument5 pagesAnnual Physical Checking of Property Furniture and Equipment Dep EDJay ArNo ratings yet
- Scouts Got Talent Score SheetDocument2 pagesScouts Got Talent Score SheetAriel PunzalanNo ratings yet
- SPJ Requirements and ManagementDocument42 pagesSPJ Requirements and ManagementVan Russel RoblesNo ratings yet
- Comparative Data of Enrollment SampleDocument3 pagesComparative Data of Enrollment SampleDanschiel RamosNo ratings yet
- Field Trip Permission Slip ApprovalDocument1 pageField Trip Permission Slip ApprovalAsti WeoNo ratings yet
- Parental Consent Form NetballDocument2 pagesParental Consent Form Netballapi-500494073No ratings yet
- Program Sequence DANADocument3 pagesProgram Sequence DANAJunjun GonzalesNo ratings yet
- Subject: Berkeley Baguio Graduation Package: Space 4 Bpo B Ayalaland Technohub Camp John Hay, Baguio CityDocument2 pagesSubject: Berkeley Baguio Graduation Package: Space 4 Bpo B Ayalaland Technohub Camp John Hay, Baguio CityJunjun GonzalesNo ratings yet
- Andy Stanley Leadership Podcast March 2021 Application GuideDocument1 pageAndy Stanley Leadership Podcast March 2021 Application GuidePorras AugustoNo ratings yet
- Formative AssessmentDocument59 pagesFormative AssessmentLjupka Pop-TodorovaNo ratings yet
- 2018 2019 The Final Cai 1 PDFDocument32 pages2018 2019 The Final Cai 1 PDFTahani Awar GurarNo ratings yet
- Ceelo Policy Report Formative AssessmentDocument24 pagesCeelo Policy Report Formative AssessmentRich ClahaNo ratings yet
- CSE Pdf-EditedDocument59 pagesCSE Pdf-EditedMa. Elena Ailes100% (3)
- Every Heart Victory Worship Song ChartDocument1 pageEvery Heart Victory Worship Song ChartJunjun GonzalesNo ratings yet