You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5808)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (843)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- TokoJAV.comDocument166 pagesTokoJAV.comKsatrio Pinayung Rizqi50% (2)
- A Immediate Implant With Provisionaliztion Journal of Clinical PeriodontologyDocument12 pagesA Immediate Implant With Provisionaliztion Journal of Clinical PeriodontologyAhmed BadrNo ratings yet
- Prioritization - FNCPDocument10 pagesPrioritization - FNCPJeffer Dancel67% (3)
- Two Handed Process Chart & Ergonomics in Textile and ApparelDocument32 pagesTwo Handed Process Chart & Ergonomics in Textile and ApparelVaanazhaganNo ratings yet
- Lenmed Health BrochureDocument7 pagesLenmed Health Brochuremaputohospital100% (13)
- DO PBL Paper Case 16 HIV OSCEDocument4 pagesDO PBL Paper Case 16 HIV OSCESmelly RaccoonNo ratings yet
- What Is The Best Indicator To Determine Anatomic PDocument12 pagesWhat Is The Best Indicator To Determine Anatomic PjhidalgomdNo ratings yet
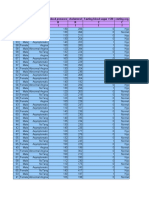
- Age Sex Chest Pain Type Blood Pressure Cholesterol Fasting Blood Sugar 120 Resting Ecg R C C R R C C I I I I I I IDocument14 pagesAge Sex Chest Pain Type Blood Pressure Cholesterol Fasting Blood Sugar 120 Resting Ecg R C C R R C C I I I I I I Isantu4_1111No ratings yet
- REGULATIONS AND CURRICULUM1.0 - CompressedDocument50 pagesREGULATIONS AND CURRICULUM1.0 - CompressedneethuNo ratings yet
- BGHMC Investment Needs For 2023 Non-Functional Specialty CentersDocument19 pagesBGHMC Investment Needs For 2023 Non-Functional Specialty CenterslykangelirNo ratings yet
- Newborn NotesDocument3 pagesNewborn NotesSharlotte EbayNo ratings yet
- Dufour 2006 - Biocultural Approaches in Human Biology PDFDocument9 pagesDufour 2006 - Biocultural Approaches in Human Biology PDFFlor DarkoNo ratings yet
- Leadership & Management Ethical - LegalDocument51 pagesLeadership & Management Ethical - Legalamasoud96 amasoud96No ratings yet
- Health Dissertation TopicsDocument6 pagesHealth Dissertation TopicsUK100% (1)
- F561M - 0818 Grapadora de PedalDocument56 pagesF561M - 0818 Grapadora de PedalSST- EshkolNo ratings yet
- Media and Information Literacy The Influence of Media and Information To Communication Learning Activity Sheet No. 1Document41 pagesMedia and Information Literacy The Influence of Media and Information To Communication Learning Activity Sheet No. 1amaya dxeuNo ratings yet
- Example of Group Forum (SCRIPT)Document7 pagesExample of Group Forum (SCRIPT)Michael Arushe50% (2)
- Healthy Heart-3Document1 pageHealthy Heart-3api-309564044No ratings yet
- GHS Format-sds-Gp CleanDocument8 pagesGHS Format-sds-Gp CleanAlan TanNo ratings yet
- Try Scribd FREE For 30 Days To Access Over 125 Million Titles Without Ads or Interruptions!Document1 pageTry Scribd FREE For 30 Days To Access Over 125 Million Titles Without Ads or Interruptions!eyaNo ratings yet
- 107 RLE Group 5 1F Newborn Delivery Final OutputDocument79 pages107 RLE Group 5 1F Newborn Delivery Final OutputJr CaniaNo ratings yet
- Impact of Occupational Stress On Quality WorkDocument9 pagesImpact of Occupational Stress On Quality WorkJasmin NayakNo ratings yet
- Beta Alanine Supplementation PresentationDocument11 pagesBeta Alanine Supplementation Presentationapi-576308167No ratings yet
- Rescue Solutions Brochure 88489Document16 pagesRescue Solutions Brochure 88489ursulaNo ratings yet
- Specimen Collection Manual For Laboratory Serivces LRHDocument100 pagesSpecimen Collection Manual For Laboratory Serivces LRHPasan MaheshaNo ratings yet
- 1577un 2026-01Document79 pages1577un 2026-01ngovantienNo ratings yet
- GRADES 1 To 12 Daily Lesson Log Monday Tuesday Wednesday Thursday FridayDocument13 pagesGRADES 1 To 12 Daily Lesson Log Monday Tuesday Wednesday Thursday FridayJessie Atillo TindoyNo ratings yet
- SACS Back To School 2020Document37 pagesSACS Back To School 2020Saige DriverNo ratings yet
- Medico-Legal Aspect of DeathDocument29 pagesMedico-Legal Aspect of DeathDm Cinco100% (1)
- Stages of LaborDocument3 pagesStages of Laborkatzuhmee leeNo ratings yet