You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- TTAV Coronavirus - Field - Guide Ty and Charlene BollingerDocument78 pagesTTAV Coronavirus - Field - Guide Ty and Charlene BollingerSakamoto ShintaroNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- 01-Reading Comprehension-Short and Long TextsDocument15 pages01-Reading Comprehension-Short and Long Textsapi-238910137No ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Spanish Flu HistoryDocument3 pagesSpanish Flu Historyrichlion50% (6)
- 1 Social Administrative and Management Sciences Q&A Content Ver1Document34 pages1 Social Administrative and Management Sciences Q&A Content Ver1bhaveshnidhi64100% (1)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Abc Book of Human DiseaseDocument27 pagesAbc Book of Human Diseaseapi-463761938No ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Ism Product Proposal EssayDocument2 pagesIsm Product Proposal Essayapi-668969983No ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Various Face Mask Studies Prove Their Ineffectiveness PDFDocument9 pagesVarious Face Mask Studies Prove Their Ineffectiveness PDFdazzo0007No ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
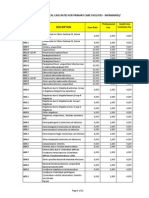
- PhilHealth Circular No. 0035, s.2013 Annex 5 List of Medical Case Rates For Primary Care FacilitiesDocument22 pagesPhilHealth Circular No. 0035, s.2013 Annex 5 List of Medical Case Rates For Primary Care FacilitiesChrysanthus HerreraNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Iceberg DiseasesDocument18 pagesIceberg Diseasesachuth29No ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Biology MCQs SSBCrack PDFDocument39 pagesBiology MCQs SSBCrack PDFPRASHANT MARKANNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Plainte Déposée Par L'avocat Grec Nikos Antoniadis (Version Anglaise)Document38 pagesPlainte Déposée Par L'avocat Grec Nikos Antoniadis (Version Anglaise)Éditions Dédicaces100% (1)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- NSABB Final Report Recommendations Evaluation Oversight Proposed Gain of Function Research May 2016Document109 pagesNSABB Final Report Recommendations Evaluation Oversight Proposed Gain of Function Research May 2016Jim Hoft100% (1)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- 05 Lecture Presentation-1Document76 pages05 Lecture Presentation-1Shahida BukhariNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- 4 Modern Science B2Document3 pages4 Modern Science B2Марія ТернавськаNo ratings yet
- The Morning Calm Korea Weekly - Nov. 25, 2005Document25 pagesThe Morning Calm Korea Weekly - Nov. 25, 2005Morning Calm Weekly NewspaperNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Animalhealth Flyer Vetmax Aiv CO125306Document2 pagesAnimalhealth Flyer Vetmax Aiv CO125306Yoana GulenovaNo ratings yet
- English Language Form 5 Part 3Document16 pagesEnglish Language Form 5 Part 3HALIL BIN SIRI MoeNo ratings yet
- JPS-The Eleventh Meeting of The Pan Arab Gastroenterology Logy and Nutrition Society - Medics Index MembersDocument20 pagesJPS-The Eleventh Meeting of The Pan Arab Gastroenterology Logy and Nutrition Society - Medics Index MembersMedicsindex Telepin Slidecase100% (4)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Clinical Applications and Pharmacological Resea - 2021 - Journal of TraditionalDocument9 pagesClinical Applications and Pharmacological Resea - 2021 - Journal of Traditionalayarin heNo ratings yet
- Actividad #1 Lectura, Comprensión y Crítica.Document9 pagesActividad #1 Lectura, Comprensión y Crítica.Nicolás RamirezNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- FSC Extra ENT and Tuning Fork January 11-Th 2018 Internet ConferenceDocument21 pagesFSC Extra ENT and Tuning Fork January 11-Th 2018 Internet Conferencemarc800No ratings yet
- Disease and First AidDocument4 pagesDisease and First AidPriyadharsini BalasubramanianNo ratings yet
- Pandemics - What Everyone Needs To Know® (PDFDrive)Document268 pagesPandemics - What Everyone Needs To Know® (PDFDrive)arquivoslivros100% (1)
- Bird Flu Exposure HandoutDocument2 pagesBird Flu Exposure HandoutJose PeñarrietaNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Viral Infection and Obesity: Current Status and Future ProspectiveDocument24 pagesViral Infection and Obesity: Current Status and Future ProspectiveBasobi MukherjeeNo ratings yet
- Influenza Vaccination and Mortality Differentiating Vaccine Effects From BiasDocument8 pagesInfluenza Vaccination and Mortality Differentiating Vaccine Effects From BiasadrianaNo ratings yet
- January 9, 2015Document12 pagesJanuary 9, 2015The Delphos HeraldNo ratings yet
- Part Two ResourcesDocument4 pagesPart Two Resourcesapi-158169273No ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Bounty Fresh Food Inc. - Bio Security ManualDocument4 pagesBounty Fresh Food Inc. - Bio Security Manualjeffrey danicoNo ratings yet
- Viện Đào Tạo Ngoại Ngữ Uel Học kỳ 1 Năm học 2023 - 2024 (Không được sử dụng tài liệu)Document6 pagesViện Đào Tạo Ngoại Ngữ Uel Học kỳ 1 Năm học 2023 - 2024 (Không được sử dụng tài liệu)ngo593465No ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)