You might also like
- DM74LS47 BCD To 7-Segment Decoder/Driver With Open-Collector OutputsDocument7 pagesDM74LS47 BCD To 7-Segment Decoder/Driver With Open-Collector OutputsMarlon Henry Arosemena ZúñigaNo ratings yet
- MG Casting PDFDocument12 pagesMG Casting PDFLokesh RameshNo ratings yet
- Microchip 18F877 DatasheetDocument218 pagesMicrochip 18F877 DatasheetberetyNo ratings yet
- ACTIVIDAD 3 Del Sena PLCDocument2 pagesACTIVIDAD 3 Del Sena PLCcarolina duque suarezNo ratings yet
- Number in EnglishDocument1 pageNumber in Englishcarolina duque suarezNo ratings yet
- Activity: Etiquette and Business Protocol 1Document2 pagesActivity: Etiquette and Business Protocol 1carolina duque suarezNo ratings yet
- Foro Semana 01Document1 pageForo Semana 01carolina duque suarezNo ratings yet
- Nuevo Documento de TextoDocument1 pageNuevo Documento de Textocarolina duque suarezNo ratings yet
- My Life ProjectDocument1 pageMy Life Projectcarolina duque suarezNo ratings yet
- International System of Units, SI SummaryDocument4 pagesInternational System of Units, SI SummaryGerman ZeceñaNo ratings yet
- OIML R 16-2: Nternational EcommendationDocument42 pagesOIML R 16-2: Nternational Ecommendationcarolina duque suarezNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Method of Statement For GroutingDocument7 pagesMethod of Statement For GroutingCezar DasiNo ratings yet
- The Impact of Computer Based Test On Senior Secondary School StudentsDocument46 pagesThe Impact of Computer Based Test On Senior Secondary School StudentsOrlanshilay100% (18)
- Module 3 Lesson 1Document4 pagesModule 3 Lesson 1Rickie Marx RonamoNo ratings yet
- Chinese Contractor Wins Kuwait Remediation WorkDocument4 pagesChinese Contractor Wins Kuwait Remediation WorkSanabel EliasNo ratings yet
- Skil Lab EBMDocument6 pagesSkil Lab EBMYahya Darmais FaridNo ratings yet
- Occupational Therapy Practice FrameworkDocument31 pagesOccupational Therapy Practice FrameworkDReKA2010100% (4)
- Staff Nurses, Lab-Technicians& Pharmacists: WWW - Vizianagaram.nic - inDocument6 pagesStaff Nurses, Lab-Technicians& Pharmacists: WWW - Vizianagaram.nic - inSATYAM NAIDUNo ratings yet
- Healing Clay - Healing Earth2Document27 pagesHealing Clay - Healing Earth2Tiger Dimension-ElNo ratings yet
- Definition of Terms: Service RadiusDocument11 pagesDefinition of Terms: Service RadiusSamuel ValentineNo ratings yet
- Improve Your Medication Management Processes: Advisory ServicesDocument2 pagesImprove Your Medication Management Processes: Advisory ServicesSimarpreet KaurNo ratings yet
- NHS Dental Statistics For England 2018-19, Annual Report (PAS) - NHS DigitalDocument3 pagesNHS Dental Statistics For England 2018-19, Annual Report (PAS) - NHS DigitalRowayda NourNo ratings yet
- Assignment - 4: The Saying Goes 'He/ She Who Knows Occlusion Knows Dentistry 'Document19 pagesAssignment - 4: The Saying Goes 'He/ She Who Knows Occlusion Knows Dentistry 'nivitha naidu100% (1)
- Ew MeritDocument120 pagesEw MeritShlok RathodNo ratings yet
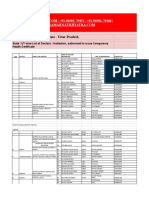
- Uttar PradeshDocument7 pagesUttar PradeshPawani Gupta100% (1)
- Tenants Pathology-Update Uploads 329 SEBASTIAN Roche ePoster+FINALDocument1 pageTenants Pathology-Update Uploads 329 SEBASTIAN Roche ePoster+FINALsanderssebastianNo ratings yet
- VTM 1sted 1-Page Caitiff InteractiveDocument1 pageVTM 1sted 1-Page Caitiff InteractivePanaSikuNo ratings yet
- Youth Camp Registration Form-2022Document1 pageYouth Camp Registration Form-2022FlerkNo ratings yet
- Portfolio in Gender and Society: Jennifer D. RoseteDocument7 pagesPortfolio in Gender and Society: Jennifer D. RoseteDmzjmb SaadNo ratings yet
- Kepelbagaian Budaya (Individual Assignment)Document6 pagesKepelbagaian Budaya (Individual Assignment)Yusran RosdiNo ratings yet
- Mhcet Mock Test-2Document29 pagesMhcet Mock Test-2Poonam UpadhyayNo ratings yet
- Histology: Diagnosis and Treatment of Acute Apical AbscessDocument4 pagesHistology: Diagnosis and Treatment of Acute Apical AbscessPrince AmiryNo ratings yet
- Managing School OperationsDocument15 pagesManaging School OperationsAmberShanty TalerNo ratings yet
- Health - WikipediaDocument16 pagesHealth - WikipediakddorNo ratings yet
- Housekeeping ProjectDocument22 pagesHousekeeping Projectpoorohit33% (3)
- Survey Method Statement For Construction Under PASSDocument28 pagesSurvey Method Statement For Construction Under PASSMustakim AnsaryNo ratings yet
- Changes of Vitamin D Levels in Parkinson's Disease in LibyaDocument1 pageChanges of Vitamin D Levels in Parkinson's Disease in LibyaJagannadh peelaNo ratings yet
- Ulkus DiabetikumDocument8 pagesUlkus DiabetikumDwi Feri HariyantoNo ratings yet
- PareidoliaDocument7 pagesPareidoliamariaNo ratings yet
- Strauman BLX Product Catalog - 450.012-A-En - LowDocument22 pagesStrauman BLX Product Catalog - 450.012-A-En - LowDiyaa SakrNo ratings yet
- Lilac Illustrated Social Psychology PresentationDocument35 pagesLilac Illustrated Social Psychology PresentationGia GajasNo ratings yet