You might also like
- EKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookFrom EverandEKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookNo ratings yet
- Module7b Reading12lead EcgDocument43 pagesModule7b Reading12lead EcgTakpire DrMadhukarNo ratings yet
- The 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsFrom EverandThe 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsNo ratings yet
- Module 7bDocument43 pagesModule 7bapi-3738700100% (1)
- ECG Rhythm Interpretation: Reading 12-Lead ECG'sDocument45 pagesECG Rhythm Interpretation: Reading 12-Lead ECG'svanstar7No ratings yet
- 12 - Lead ECG-A Web Brain For Easy InterpretationDocument54 pages12 - Lead ECG-A Web Brain For Easy Interpretatione-kino3692100% (1)
- ECG InterpretationDocument83 pagesECG InterpretationJuana Maria Garcia Espinoza100% (2)
- Normal Impulse Conduction: Sinoatrial Node AV Node Bundle of His Bundle Branches Purkinje FibersDocument73 pagesNormal Impulse Conduction: Sinoatrial Node AV Node Bundle of His Bundle Branches Purkinje FibersIndra ToshiwayNo ratings yet
- Normal Impulse Conduction and ECG InterpretationDocument73 pagesNormal Impulse Conduction and ECG InterpretationIndra ToshiwayNo ratings yet
- 5 ECG Interpretation With AnswersDocument48 pages5 ECG Interpretation With AnswersQusai Ibraheem100% (1)
- ECGDocument115 pagesECGBhakti WashilkarNo ratings yet
- 16-Handout - ECG Interpretation (Study This)Document38 pages16-Handout - ECG Interpretation (Study This)Sa GhNo ratings yet
- Basics of EKG InterpretationDocument132 pagesBasics of EKG InterpretationArif Imam HidayatNo ratings yet
- Basics of EKG InterpretationDocument132 pagesBasics of EKG InterpretationSiddhant GautamNo ratings yet
- Introduction To ECG RhythmsDocument59 pagesIntroduction To ECG RhythmsIvona RagužNo ratings yet
- ECG Interpretation UnismaDocument178 pagesECG Interpretation UnismadefinaNo ratings yet
- QTc Interval - The Corrected QT IntervalDocument4 pagesQTc Interval - The Corrected QT IntervalkaelenNo ratings yet
- A Simplified ECG GuideDocument4 pagesA Simplified ECG Guidejalan_z96% (26)
- Intepretasi EKG (DR Eka)Document93 pagesIntepretasi EKG (DR Eka)Danil Anugrah JayaNo ratings yet
- ECG ECHO12007 NotesDocument133 pagesECG ECHO12007 NotescassandramacphersonNo ratings yet
- ElectrocardiogramDocument11 pagesElectrocardiogramAbby BhevNo ratings yet
- Cme Ecg InterpretationDocument60 pagesCme Ecg InterpretationAtirah AaNo ratings yet
- Basics of ECG Pre-Workshop: Dr. Nancy Selfridge Chair, Department of Clinical Medicine Semester 4 2019Document43 pagesBasics of ECG Pre-Workshop: Dr. Nancy Selfridge Chair, Department of Clinical Medicine Semester 4 2019Tom TsouNo ratings yet
- ECG Basics Lecture 1Document116 pagesECG Basics Lecture 1AreebaNo ratings yet
- EKG Interpretasi Dan Lethal Aritmia: Aan NuraeniDocument34 pagesEKG Interpretasi Dan Lethal Aritmia: Aan NuraeniCitra Marchelina Novilini100% (1)
- How To Read An ECGDocument15 pagesHow To Read An ECGSarah RonquilloNo ratings yet
- ECG tutorial covers basics, axis, waves, intervals, hypertrophy and moreDocument56 pagesECG tutorial covers basics, axis, waves, intervals, hypertrophy and morefeby_valNo ratings yet
- Management of Perioperative ArrhythmiasDocument51 pagesManagement of Perioperative ArrhythmiasAbhishek LonikarNo ratings yet
- ECG FinalDocument128 pagesECG FinalErikaNo ratings yet
- Dr. Anas Yasin - MDDocument58 pagesDr. Anas Yasin - MDMahfouzNo ratings yet
- ELECTROCARDIOGRAPHYDocument75 pagesELECTROCARDIOGRAPHYMeliaNo ratings yet
- Pediatrics ECG by DR Ali Bel KheirDocument9 pagesPediatrics ECG by DR Ali Bel KheirFerasNo ratings yet
- The 12-Lead EKG: A Step-by-Step GuideDocument31 pagesThe 12-Lead EKG: A Step-by-Step GuideJay JiangNo ratings yet
- ECG LectureDocument214 pagesECG Lecturensyuzon100% (1)
- Atria Arrythmia TestDocument8 pagesAtria Arrythmia TestAnnette SandovalNo ratings yet
- ECG Interpretation Guide: Learn How to Read and Analyze an ElectrocardiogramDocument40 pagesECG Interpretation Guide: Learn How to Read and Analyze an ElectrocardiogramAnonymous HAbhRTs2TfNo ratings yet
- Ecg Basics - NAVEENDocument65 pagesEcg Basics - NAVEENNaveen MathieuNo ratings yet
- Systematic Approach To ECGDocument12 pagesSystematic Approach To ECGAmr El TaherNo ratings yet
- ECG - Systematic-ApproachDocument12 pagesECG - Systematic-ApproachMicael MendesNo ratings yet
- Basics of EKG InterpretationDocument53 pagesBasics of EKG InterpretationHala BahaaNo ratings yet
- EcgDocument6 pagesEcgMohamed IbrahimNo ratings yet
- Mikosis Endemik-WPS OfficeDocument75 pagesMikosis Endemik-WPS OfficeKurniatiKhasanahQhafisaQurratul'ainNo ratings yet
- Ecg Interpretation New TemplateDocument88 pagesEcg Interpretation New TemplateJonathan NgNo ratings yet
- BASIC ECG GUIDE FOR NURSESDocument112 pagesBASIC ECG GUIDE FOR NURSESSam jr TababaNo ratings yet
- Kuliah EKG Blok Kegawatdaruratan September 2018Document122 pagesKuliah EKG Blok Kegawatdaruratan September 2018khanzaisdiharanaNo ratings yet
- Dasar Ekg Iwe - RSPP Seminar RSPPDocument89 pagesDasar Ekg Iwe - RSPP Seminar RSPPMabro CahyoNo ratings yet
- How To Read An ECGDocument24 pagesHow To Read An ECGredroseeeeeeNo ratings yet
- EKG DasarDocument54 pagesEKG Dasarseptiyana indahpraptiwiNo ratings yet
- Gamal Abd EL Nasser Mahmoud: Prepared ByDocument64 pagesGamal Abd EL Nasser Mahmoud: Prepared ByMohamed ElkadyNo ratings yet
- How To Read An ECGDocument21 pagesHow To Read An ECGSlychenkoNo ratings yet
- 11 Steps of ECG - Ali Alnahari PDFDocument16 pages11 Steps of ECG - Ali Alnahari PDFBìnhNo ratings yet
- Principles of ECGDocument11 pagesPrinciples of ECGDeinielle Magdangal RomeroNo ratings yet
- Ecg Crit - CareDocument55 pagesEcg Crit - CarekrismatactayNo ratings yet
- Elektro Kardio Grafi - Dasar - : DR Eka Ginanjar, SPPDDocument105 pagesElektro Kardio Grafi - Dasar - : DR Eka Ginanjar, SPPDalmiraerickaiNo ratings yet
- ECG Interpretation & Dysrhythmia Identification: by Naaim AliDocument47 pagesECG Interpretation & Dysrhythmia Identification: by Naaim AliMohamed ElkadyNo ratings yet
- Ecg Guidelines: Donna J. Castillo, MDDocument76 pagesEcg Guidelines: Donna J. Castillo, MDBheck Magat100% (1)
- ECG InterpretationDocument1 pageECG InterpretationCecil-An DalanonNo ratings yet
- Kamis 10 September 2015 - IPD 2 - Kuliah-Ekg-Blok-KegawatdaruratanDocument118 pagesKamis 10 September 2015 - IPD 2 - Kuliah-Ekg-Blok-KegawatdaruratanIrfanArifZulfikarNo ratings yet
- How To Read An ECGDocument15 pagesHow To Read An ECGcharlyn206No ratings yet
- Biosynthesis PDFDocument43 pagesBiosynthesis PDFtrinitysugumarNo ratings yet
- Stock market books beginners tamilDocument2 pagesStock market books beginners tamiltrinitysugumarNo ratings yet
- All the Good Stuff Book ReviewDocument3 pagesAll the Good Stuff Book Reviewtrinitysugumar0% (1)
- Analytical Standardization of Brahmi Nei and Effect of Siddha Methodologies On Spasticity in Cerebral PalsyDocument8 pagesAnalytical Standardization of Brahmi Nei and Effect of Siddha Methodologies On Spasticity in Cerebral PalsytrinitysugumarNo ratings yet
- Purine Metabolism PathwaysDocument29 pagesPurine Metabolism Pathwaystrinitysugumar0% (1)
- Tamil Comedy MoviesDocument4 pagesTamil Comedy Moviesnts1020No ratings yet
- Inosinic AcidDocument19 pagesInosinic AcidtrinitysugumarNo ratings yet
- Nucleic Acid Metabolism PDFDocument29 pagesNucleic Acid Metabolism PDFtrinitysugumar100% (1)
- HH Blood Group: This Article Needs Additional Citations For VerificationDocument22 pagesHH Blood Group: This Article Needs Additional Citations For VerificationtrinitysugumarNo ratings yet
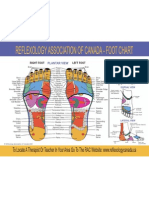
- Foot Chart - English清楚Document1 pageFoot Chart - English清楚junkuiwangNo ratings yet
- COVID-19 Hotspots in India List - Version 2 - 270420 PDFDocument40 pagesCOVID-19 Hotspots in India List - Version 2 - 270420 PDFDeepali Garg50% (4)
- LUNGS FunctionsDocument4 pagesLUNGS FunctionstrinitysugumarNo ratings yet
- Kapa Suram - Kaviya Ssura NoolDocument5 pagesKapa Suram - Kaviya Ssura NooltrinitysugumarNo ratings yet
- Corona VirusDocument10 pagesCorona VirustrinitysugumarNo ratings yet
- Acupuncture Is Fake?Document6 pagesAcupuncture Is Fake?rswongym449No ratings yet
- Asthma MimcsDocument7 pagesAsthma MimcstrinitysugumarNo ratings yet
- S PDFDocument6 pagesS PDFtrinitysugumarNo ratings yet
- Meanings of FL Ower Therapy For Anxiety in People With Overweight or ObesityDocument6 pagesMeanings of FL Ower Therapy For Anxiety in People With Overweight or ObesitytrinitysugumarNo ratings yet
- To Do Activity ProgressDocument2 pagesTo Do Activity ProgresstrinitysugumarNo ratings yet
- Foot Chart - English清楚Document1 pageFoot Chart - English清楚junkuiwangNo ratings yet
- Printable Hand Reflexology ChartDocument3 pagesPrintable Hand Reflexology Charthertz27100% (1)
- Learn Acupressure Point Names and Locations For Self-Treatment - HerbalShopDocument23 pagesLearn Acupressure Point Names and Locations For Self-Treatment - HerbalShoptrinitysugumarNo ratings yet
- Guitar Chord Encyclopedia 36 Chords in Each Key Ultimate Guitarists Reference by Steve HallDocument47 pagesGuitar Chord Encyclopedia 36 Chords in Each Key Ultimate Guitarists Reference by Steve Halltrinitysugumar0% (3)
- Learn Acupressure Point Names and Locations For Self-Treatment - HerbalShopDocument23 pagesLearn Acupressure Point Names and Locations For Self-Treatment - HerbalShoptrinitysugumarNo ratings yet
- Swot BagusDocument2 pagesSwot BagusdianNo ratings yet
- OsteopathyDocument64 pagesOsteopathytrinitysugumarNo ratings yet
- Dorn Method Advanced Training Course OutlineDocument1 pageDorn Method Advanced Training Course OutlinetrinitysugumarNo ratings yet
- Fretboard Diagrams Scales and Modes Arpeggios and Chord ChartsDocument26 pagesFretboard Diagrams Scales and Modes Arpeggios and Chord ChartstrinitysugumarNo ratings yet
- Cuba (Nocturne) by Isaac AlbenizDocument8 pagesCuba (Nocturne) by Isaac Albenizmleoto7332No ratings yet
- Management If Intra-Arterial Injection, ATOTW 2023Document6 pagesManagement If Intra-Arterial Injection, ATOTW 2023Ali AftabNo ratings yet
- LEAN Weekly Guide - August 24 - 7 Day Best of The Best AbsDocument1 pageLEAN Weekly Guide - August 24 - 7 Day Best of The Best AbsNisita_dyahNo ratings yet
- Zoology II Year EM FinalDocument106 pagesZoology II Year EM FinalAlina KuwaitNo ratings yet
- Excellup Class TenDocument3 pagesExcellup Class TenHemant KumarNo ratings yet
- Kami Export - Hamad Alsayer - Gizmo Circulatory System PDFDocument4 pagesKami Export - Hamad Alsayer - Gizmo Circulatory System PDFbratlyNo ratings yet
- Duration of Dual Antiplatelet Therapy: Current ControversiesDocument8 pagesDuration of Dual Antiplatelet Therapy: Current ControversiesRajendra ChavanNo ratings yet
- B22123 POCUS Workbook LinkedDocument39 pagesB22123 POCUS Workbook LinkedDrMarcus KeyboardNo ratings yet
- IV Calcium Gluconate IV Labetalol IV Methyldopa IV LorazepamDocument22 pagesIV Calcium Gluconate IV Labetalol IV Methyldopa IV Lorazepamabod alaniNo ratings yet
- CABG x4Document2 pagesCABG x4Indranil SinhaNo ratings yet
- AAP Common Cardiac Issues in Pediatrics 2018 PDFDocument786 pagesAAP Common Cardiac Issues in Pediatrics 2018 PDFiahmad9No ratings yet
- Tony Cross CDU Low Risk ACS Proforma - V3.212 Review Due June 2014Document4 pagesTony Cross CDU Low Risk ACS Proforma - V3.212 Review Due June 2014ED@HEFTNo ratings yet
- Daftar PustakaDocument4 pagesDaftar PustakaWe HereNo ratings yet
- BTEC Sport Level 3 Revision Guide Cardiovascular SystemDocument19 pagesBTEC Sport Level 3 Revision Guide Cardiovascular SystemMPNo ratings yet
- Management of Cardiogenic Shock After Acute - 2023Document10 pagesManagement of Cardiogenic Shock After Acute - 2023Angy KarakostaNo ratings yet
- Department of Education Division of Leyte Taberna National High SchoolDocument3 pagesDepartment of Education Division of Leyte Taberna National High SchoolSheila May Tapales TabonNo ratings yet
- 10 1016@j Amjcard 2018 03 369Document21 pages10 1016@j Amjcard 2018 03 369Martin De Santiago ValenzuelaNo ratings yet
- PathophysiologyDocument3 pagesPathophysiologyali sarjunipadangNo ratings yet
- DR Hasanah - Update Manajemen Terapi Gagal JantungDocument43 pagesDR Hasanah - Update Manajemen Terapi Gagal JantungnadiaNo ratings yet
- Heart Failure Pelatihan Dokter KeluargaDocument55 pagesHeart Failure Pelatihan Dokter KeluargaDelia NingrumNo ratings yet
- Date/ Time Cues Need Nursing Diagnosis Patient Outcome Planning of Intervention Implementation Evaluation Objective: - R: HypotensionDocument5 pagesDate/ Time Cues Need Nursing Diagnosis Patient Outcome Planning of Intervention Implementation Evaluation Objective: - R: HypotensionGregg AndoyNo ratings yet
- Electrophysiological Maneuvers For Arrhythmia Analysis-Cardiotext Publishing (2014)Document211 pagesElectrophysiological Maneuvers For Arrhythmia Analysis-Cardiotext Publishing (2014)Ali Uğur Soysal100% (1)
- Of Our Mission: at The HeartDocument6 pagesOf Our Mission: at The Heartkhairul ihsanNo ratings yet
- Long-Term Mortality After The Blood Pressure and Lipid-Lowering Treatment in Hypertensive Patients: 16-Year Follow-Up of The ASCOT Legacy StudyDocument22 pagesLong-Term Mortality After The Blood Pressure and Lipid-Lowering Treatment in Hypertensive Patients: 16-Year Follow-Up of The ASCOT Legacy StudyFlore HountondjiNo ratings yet
- Sila Gy 1994Document5 pagesSila Gy 1994Arbey Aponte PuertoNo ratings yet
- Case Điện tâm đồDocument287 pagesCase Điện tâm đồSelina BerniceNo ratings yet
- Pamj 36 187Document14 pagesPamj 36 187Lisa SariNo ratings yet
- BME - 314 Biomedical Equipments Course OverviewDocument1 pageBME - 314 Biomedical Equipments Course Overviewrohit860No ratings yet
- TỔNG HỢP CÁC DẠNG CÂU HỎI MÔN TOÁN XUẤT HIỆN TRONG ĐỀ THI TĐNDocument10 pagesTỔNG HỢP CÁC DẠNG CÂU HỎI MÔN TOÁN XUẤT HIỆN TRONG ĐỀ THI TĐNVan NguyenNo ratings yet
- Obstetrics AclsDocument6 pagesObstetrics AclsPedro BurgosNo ratings yet
- Drug StudyDocument6 pagesDrug StudySoleil MaxwellNo ratings yet