You might also like
- 17.IFU G11 Var ReagentsDocument68 pages17.IFU G11 Var ReagentsAufar SyahrulianNo ratings yet
- ADAMS - HA 8180V - Operation and Maintenance (2020 - 08 - 20 02 - 50 - 44 UTC)Document51 pagesADAMS - HA 8180V - Operation and Maintenance (2020 - 08 - 20 02 - 50 - 44 UTC)Arnoldo Felix0% (1)
- HbA1c Reageant KitsDocument4 pagesHbA1c Reageant KitsMichael TanglaoNo ratings yet
- Orac MethodDocument5 pagesOrac MethodPriscillaL.SilvaNo ratings yet
- Practice Quiz M1 (Ungraded) - MergedDocument22 pagesPractice Quiz M1 (Ungraded) - MergedAbdullah Abdullah100% (1)
- Mañanita Songs Mañanita SongsDocument2 pagesMañanita Songs Mañanita SongsSanchez Bayan100% (1)
- Confined Space Entry: OSHA Standard 1910.146Document38 pagesConfined Space Entry: OSHA Standard 1910.146SKH CultureNo ratings yet
- Preformed Expansion Joint Filler For Concrete (Bituminous Type)Document2 pagesPreformed Expansion Joint Filler For Concrete (Bituminous Type)Katerin HernandezNo ratings yet
- 1 Sebia - Presentation 1 HbA1c Next Generation Separation Method (Aug 2017) - EnglishDocument54 pages1 Sebia - Presentation 1 HbA1c Next Generation Separation Method (Aug 2017) - EnglishVương KiênNo ratings yet
- Glycated Hemoglobin (Hba1C) : Prepared By: Basalingappa.B.G. 2 M.Sc. Medical Biochemistry JSS Medical College MysoreDocument46 pagesGlycated Hemoglobin (Hba1C) : Prepared By: Basalingappa.B.G. 2 M.Sc. Medical Biochemistry JSS Medical College MysoreYuniati ValentinaNo ratings yet
- HPLC Tech 2021 WebDocument6 pagesHPLC Tech 2021 WebRajat VarmiNo ratings yet
- GX Variant EN Rev 07112013 01 PDFDocument8 pagesGX Variant EN Rev 07112013 01 PDFQuang Pham NhatNo ratings yet
- Roche Tina Quant Hba1C: Setting A New Precedent in Hba1C Lab EfficiencyDocument23 pagesRoche Tina Quant Hba1C: Setting A New Precedent in Hba1C Lab EfficiencyrezqiNo ratings yet
- HB A1c Meta-Analysis - Second Edition - Final 20182304Document50 pagesHB A1c Meta-Analysis - Second Edition - Final 20182304Kader SmailiNo ratings yet
- Mini CLSI guide for Staph, Strep and CoryneDocument19 pagesMini CLSI guide for Staph, Strep and CoryneMuhammad Yssir100% (1)
- Guidelines Microbiology Lab ProceduresDocument61 pagesGuidelines Microbiology Lab ProceduresSadao MatsumotoNo ratings yet
- Brosur HbA1c DxGEN PDFDocument4 pagesBrosur HbA1c DxGEN PDFAnonymous AFEzu0No ratings yet
- MANUAL ElectrophoresisDocument24 pagesMANUAL ElectrophoresisMohamed Ali50% (2)
- Serum Protein Electrophoresis: Interpreting ResultsDocument23 pagesSerum Protein Electrophoresis: Interpreting ResultsRajesh_AnanthuNo ratings yet
- Pato 2Document25 pagesPato 2api-3713854No ratings yet
- Semen Analysis WHO StandardDocument286 pagesSemen Analysis WHO StandardSam Lai100% (1)
- Stago BrochureDocument44 pagesStago BrochureagbnetNo ratings yet
- Sysmex SEED 4 2013 Automated Haematology Sample Interferences Flagging and Results Interpretation - Part 1 enDocument8 pagesSysmex SEED 4 2013 Automated Haematology Sample Interferences Flagging and Results Interpretation - Part 1 enPieter Du Toit-Enslin50% (2)
- Lipemia: Causes, Interference Mechanisms, Detection and ManagementDocument16 pagesLipemia: Causes, Interference Mechanisms, Detection and ManagementkartikaparamitaNo ratings yet
- 5.5 Serum Protein ElectrophoresisDocument2 pages5.5 Serum Protein ElectrophoresisMai MostafaNo ratings yet
- 1111 Chemical Composition of Berry Essential Oils From Juniperus Communis L. From MACEDONIA PDFDocument10 pages1111 Chemical Composition of Berry Essential Oils From Juniperus Communis L. From MACEDONIA PDFGaston CassaroNo ratings yet
- Platlets DisorderDocument177 pagesPlatlets DisorderFatimah A Al-dawoodNo ratings yet
- Platelet Aggregometry - NotesDocument2 pagesPlatelet Aggregometry - NotesNilginCombatirPonceNo ratings yet
- Casts in The Urine SedimentDocument3 pagesCasts in The Urine SedimentSyazmin KhairuddinNo ratings yet
- Techtalk August2010Document2 pagesTechtalk August2010Abu KhalidNo ratings yet
- ABL5 Blood Gas Analyser & AnalysisDocument46 pagesABL5 Blood Gas Analyser & AnalysisSurbhi MittalNo ratings yet
- Fluorescence-Activated Cell SortingDocument10 pagesFluorescence-Activated Cell SortingShaher Bano MirzaNo ratings yet
- ADVIA-2120i Hematology TrainingDocument73 pagesADVIA-2120i Hematology TrainingLoay TibiNo ratings yet
- Clsi-Catalog Web Links042414Document64 pagesClsi-Catalog Web Links042414PerezGut100% (1)
- Hemophilia and Factor Assay PDFDocument17 pagesHemophilia and Factor Assay PDFSumaira JunaidNo ratings yet
- Sysmex ScattergramsDocument7 pagesSysmex ScattergramsRuxandra Mesaros100% (1)
- Laboratory Hematology CriteriaDocument7 pagesLaboratory Hematology CriteriaRosNo ratings yet
- Bayer A1CNow HCP Product InsertDocument11 pagesBayer A1CNow HCP Product InsertLindsay YooNo ratings yet
- Lod-Loq-Signal To Noise Ratio Etc. Important ArticleDocument5 pagesLod-Loq-Signal To Noise Ratio Etc. Important Articleanon_687115068No ratings yet
- Guide to Diagnostic Tests for Paroxysmal Nocturnal HemoglobinuriaDocument3 pagesGuide to Diagnostic Tests for Paroxysmal Nocturnal HemoglobinuriaOrxan HumbetovNo ratings yet
- WHO Use of Anticoagulants and Stability of Samples PDFDocument64 pagesWHO Use of Anticoagulants and Stability of Samples PDFImre DinnyesNo ratings yet
- Laboratory Turnaround TimeDocument17 pagesLaboratory Turnaround TimeNicole HoNo ratings yet
- One Step Hepatitis B Virus Test KitDocument34 pagesOne Step Hepatitis B Virus Test KitGail IbanezNo ratings yet
- CC1 - Topic 1Document11 pagesCC1 - Topic 1Marie MontemarNo ratings yet
- RBCDocument66 pagesRBCFarah mansourNo ratings yet
- Evaluation of New LAB MethodsDocument100 pagesEvaluation of New LAB MethodsSTARK DIAGNOSTICSNo ratings yet
- Radial ImmunoDocument8 pagesRadial Immunograce meunierNo ratings yet
- Preanalytical ErrorsDocument99 pagesPreanalytical ErrorsSulakshmi KurlekarNo ratings yet
- AnaemiaDocument27 pagesAnaemiaSamahir F HusseinNo ratings yet
- CC Lecture Reviewer - ppt3 (QC Part2)Document10 pagesCC Lecture Reviewer - ppt3 (QC Part2)Johanna Rose Cobacha SalvediaNo ratings yet
- Statistical Approach in HematologyDocument33 pagesStatistical Approach in HematologycandiddreamsNo ratings yet
- XN Series: Case InterpretationDocument41 pagesXN Series: Case InterpretationTanveerNo ratings yet
- CorrelationDocument17 pagesCorrelationisabel bautistaNo ratings yet
- Automated Versus Manual Platelet Count in Aden 2161 0681-3-149Document4 pagesAutomated Versus Manual Platelet Count in Aden 2161 0681-3-149Jeffry MaglalangNo ratings yet
- Slide Preparation of Cerebrospinal Fluid For Cytological ExaminationDocument3 pagesSlide Preparation of Cerebrospinal Fluid For Cytological ExaminationMurshed HaidarNo ratings yet
- The Diagnostic Use of ADVIA 2120i Siemens and An "APL Criteria" CanDocument9 pagesThe Diagnostic Use of ADVIA 2120i Siemens and An "APL Criteria" CananggaririnNo ratings yet
- Plasma Protein BindingDocument2 pagesPlasma Protein BindingKavish ChhajedNo ratings yet
- Validation Cell AnalyzersDocument45 pagesValidation Cell AnalyzerscandiddreamsNo ratings yet
- Uric Acid Mono SL: Clinical SignificanceDocument2 pagesUric Acid Mono SL: Clinical SignificancexlkoNo ratings yet
- 68th AACC Annual Scientific Meeting Abstract eBookFrom Everand68th AACC Annual Scientific Meeting Abstract eBookNo ratings yet
- Automated Glycohemoglobin Analyzer Handles Increasing HbA1c Testing WorkloadDocument8 pagesAutomated Glycohemoglobin Analyzer Handles Increasing HbA1c Testing WorkloadNia AmbarwatiNo ratings yet
- G8 Variant EN Rev 09072013 01Document9 pagesG8 Variant EN Rev 09072013 01Nia AmbarwatiNo ratings yet
- Ajcpath138 0448Document9 pagesAjcpath138 0448Bihlul AbiNo ratings yet
- Taylors 10 Minute Diagnosis Manual Symptoms and Signs in The Time Limited Encounter PDFDocument656 pagesTaylors 10 Minute Diagnosis Manual Symptoms and Signs in The Time Limited Encounter PDF19marvoloNo ratings yet
- A Review: HPLC Method Development and Validation: November 2015Document7 pagesA Review: HPLC Method Development and Validation: November 2015R Abdillah AkbarNo ratings yet
- Thermal Performance of Air-Cooled Condensing Units by CFD SimulationDocument2 pagesThermal Performance of Air-Cooled Condensing Units by CFD SimulationFauziah JeraiNo ratings yet
- Model Question Paper and Solution 2022Document14 pagesModel Question Paper and Solution 2022R Y AnushNo ratings yet
- Common Mistakes in Dimensional Calibration MethodsDocument16 pagesCommon Mistakes in Dimensional Calibration MethodssujudNo ratings yet
- API 510 BasicsDocument40 pagesAPI 510 BasicsBalakumarNo ratings yet
- BrosurDocument68 pagesBrosurKiki Xhui7No ratings yet
- Hero LetterDocument3 pagesHero LetterArunachalam Muthiah0% (1)
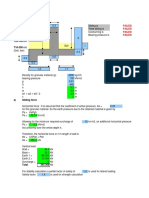
- Sliding, Overturning, Bearing Pressure and Bending Reinforcement Calculations for Retaining WallDocument4 pagesSliding, Overturning, Bearing Pressure and Bending Reinforcement Calculations for Retaining WallAbdul Aziz Julkarnain ZulkifliNo ratings yet
- Introduction To The Philosophy of The Human PersonDocument14 pagesIntroduction To The Philosophy of The Human PersonDan Niel50% (2)
- Deks Olje ArticleDocument5 pagesDeks Olje ArticleTomMacNaughtonNo ratings yet
- Bio-Sil ULTRA 1050: Medically Pure Platinum-Cured Silicone Tubing With An Ultra-Smooth Inner SurfaceDocument2 pagesBio-Sil ULTRA 1050: Medically Pure Platinum-Cured Silicone Tubing With An Ultra-Smooth Inner SurfaceLari GrossiNo ratings yet
- Memorial Garden Policies and Guidelines St. Mark's Episcopal Church, Raleigh, North CarolinaDocument7 pagesMemorial Garden Policies and Guidelines St. Mark's Episcopal Church, Raleigh, North Carolinaestela maria dulaganNo ratings yet
- Generador APD550PEDocument4 pagesGenerador APD550PEFTL1990No ratings yet
- Fair Directory 02-2016Document44 pagesFair Directory 02-2016Ravichandran SNo ratings yet
- Beyond Schein DentalDocument9 pagesBeyond Schein DentaltomdietzlerNo ratings yet
- General Biology 1: Go Fast, or Slow Down?Document23 pagesGeneral Biology 1: Go Fast, or Slow Down?Mikhael OiraNo ratings yet
- G5 C11 TestDocument6 pagesG5 C11 TestvictoriaNo ratings yet
- Pasture FatteningDocument15 pagesPasture FatteningKartika PurnamasariNo ratings yet
- SteelsDocument72 pagesSteelsLLNo ratings yet
- Memories of HomeDocument14 pagesMemories of HomeMary Francis Edmer SayconNo ratings yet
- Popular CultureDocument25 pagesPopular CultureVibhuti KachhapNo ratings yet
- EU Food Label GuidanceDocument99 pagesEU Food Label GuidanceMunteanu CristianNo ratings yet
- Hearing Aid InformationDocument22 pagesHearing Aid InformationDeepakRodeyNo ratings yet
- Fit For WashingDocument85 pagesFit For WashingIyaka YoeNo ratings yet
- Computational Models For Trunk Trajectory Planning and Load Distribution: A Test-Bed For Studying Various Clinical Adaptation and Motor Control Strategies of Low Back Pain PatientsDocument13 pagesComputational Models For Trunk Trajectory Planning and Load Distribution: A Test-Bed For Studying Various Clinical Adaptation and Motor Control Strategies of Low Back Pain PatientsOTorresGonzalezNo ratings yet