You might also like
- Scared SickDocument320 pagesScared SickChapali100% (5)
- Physiology of PainDocument30 pagesPhysiology of PainVaibhavJain100% (1)
- Drugs in Neurology - OXFORD 2017Document677 pagesDrugs in Neurology - OXFORD 2017athenea89100% (1)
- Cerebral Palsy PDFDocument6 pagesCerebral Palsy PDFprasadNo ratings yet
- Dry Needling TrapezitisDocument52 pagesDry Needling Trapezitismita.faalNo ratings yet
- FIDNDocument21 pagesFIDNBeta WattimenaNo ratings yet
- Back Pain PathophysiologyDocument33 pagesBack Pain PathophysiologyDaryo Soemitro94% (18)
- 1.pfizer Documents Reveal at Least 800 People Never Finished The COVID Vaccine Trial Due To Death, Injury or Withdrawn Consent - The ExposeDocument15 pages1.pfizer Documents Reveal at Least 800 People Never Finished The COVID Vaccine Trial Due To Death, Injury or Withdrawn Consent - The ExposeElvaNo ratings yet
- A Simple Guide to Neuralgia and Related Nerve DisordersFrom EverandA Simple Guide to Neuralgia and Related Nerve DisordersRating: 5 out of 5 stars5/5 (5)
- An Introduction To Regenerative Injection Therapy RIT in Interventional Regenerative Orthopedic Medicine IROMDocument71 pagesAn Introduction To Regenerative Injection Therapy RIT in Interventional Regenerative Orthopedic Medicine IROMEnzo100% (2)
- Nerve InjuriesDocument20 pagesNerve InjuriesAnupama NagrajNo ratings yet
- Caries Activity TestDocument8 pagesCaries Activity TestSaransh MalotNo ratings yet
- Basic Principles of Peripheral Nerve DisordersDocument288 pagesBasic Principles of Peripheral Nerve DisordersJosé Ramírez100% (1)
- Step 2 CK (CCSSA) Form 6Document51 pagesStep 2 CK (CCSSA) Form 6Appu ayyalaNo ratings yet
- Peripheral Nerve Entrapment Hydrodissection and Neural Regenerative Strategies Andrea Trescot 2015 PDFDocument9 pagesPeripheral Nerve Entrapment Hydrodissection and Neural Regenerative Strategies Andrea Trescot 2015 PDFAngela PagliusoNo ratings yet
- Herbal Cancer Treatment - Sabah Snake GrassDocument6 pagesHerbal Cancer Treatment - Sabah Snake GrassGelo Joson100% (2)
- Case Analysis Bronchial AsthmaDocument21 pagesCase Analysis Bronchial AsthmaKim LladaNo ratings yet
- Intralipid infusion for Myelin Sheath Repair in Multiple Sclerosis and Trigeminal Neuralgia?From EverandIntralipid infusion for Myelin Sheath Repair in Multiple Sclerosis and Trigeminal Neuralgia?No ratings yet
- Técnicas Neuroquirúrgicas IDocument6 pagesTécnicas Neuroquirúrgicas ISociedad de Gerontología y Geriatría del PerúNo ratings yet
- Interventional Pain ManagementDocument2 pagesInterventional Pain ManagementjosephNo ratings yet
- DRG in Chronic PainDocument10 pagesDRG in Chronic PainDido KamelNo ratings yet
- Pain in Trigeminal Neuralgia: Neurophysiology and Measurement: A Comprehensive ReviewDocument6 pagesPain in Trigeminal Neuralgia: Neurophysiology and Measurement: A Comprehensive ReviewTejo PramonoNo ratings yet
- Fneur 14 1104817Document6 pagesFneur 14 1104817geowalker7092No ratings yet
- Carbamazepine Relieves Trigeminal Neuralgia PainDocument6 pagesCarbamazepine Relieves Trigeminal Neuralgia PainlarasatiNo ratings yet
- PCT 2Document20 pagesPCT 2Wialda Dwi rodyahNo ratings yet
- Cagnie2013 Physiological Effects of Dry NeedlingDocument8 pagesCagnie2013 Physiological Effects of Dry NeedlingWahyu FathurrachmanNo ratings yet
- Oclusion y Desordenes TemporomandibularesDocument8 pagesOclusion y Desordenes TemporomandibularesEsteban AlvaradoNo ratings yet
- Inflammation and Nerve FiberDocument10 pagesInflammation and Nerve FiberAnnisaastikaNo ratings yet
- Anesthetics and AnesthesiologyDocument4 pagesAnesthetics and AnesthesiologyPrisiliaNo ratings yet
- Surgery in The DREZ For Refractory Neuropathic Pain After Spinal Cord/Cauda Equina InjuryDocument2 pagesSurgery in The DREZ For Refractory Neuropathic Pain After Spinal Cord/Cauda Equina InjurystancaNo ratings yet
- Chapter 8. Pain Pathways and Mechanisms of The Pulpodentin Complex - CompressedDocument26 pagesChapter 8. Pain Pathways and Mechanisms of The Pulpodentin Complex - CompressedPaola cruzNo ratings yet
- TL 1Document4 pagesTL 1ĐôngNo ratings yet
- Shock 2Document6 pagesShock 2diretoriacmbaNo ratings yet
- Ef Ficacy of Transcutaneous Electrical Nerve Stimulation in People With Pain After Spinal Cord Injury: A Meta-AnalysisDocument7 pagesEf Ficacy of Transcutaneous Electrical Nerve Stimulation in People With Pain After Spinal Cord Injury: A Meta-Analysisxian karachiNo ratings yet
- A Review On Oral and Dental PainDocument5 pagesA Review On Oral and Dental PainzainaNo ratings yet
- Anestesi Text Book ReadingDocument5 pagesAnestesi Text Book Readingli2delNo ratings yet
- Ultrasound-Guided Nerve Blocks in The Head and Neck For Chronic Pain Management - The Anatomy, Sonoanatomy, and ProcedureDocument16 pagesUltrasound-Guided Nerve Blocks in The Head and Neck For Chronic Pain Management - The Anatomy, Sonoanatomy, and Proceduremarcus moraisNo ratings yet
- Peripheral Nerve Injuries and TreatmentDocument24 pagesPeripheral Nerve Injuries and TreatmentSakanadeNo ratings yet
- Jurding NeuroDocument6 pagesJurding NeuroAulia sabrina ramadhantyNo ratings yet
- Pain Pathways and Mechanisms of the Pulpodentin ComplexDocument9 pagesPain Pathways and Mechanisms of the Pulpodentin ComplexKyucha ChanNo ratings yet
- WEISSPNEDocument4 pagesWEISSPNELauraNo ratings yet
- Low Back Related Leg Pain Is The Nerve Guilty How To Differentiate The Underlying Pain MechanismDocument8 pagesLow Back Related Leg Pain Is The Nerve Guilty How To Differentiate The Underlying Pain Mechanism杨钦杰No ratings yet
- AnesthesiaDocument2 pagesAnesthesiakitten14No ratings yet
- The Neurobiology of Acute PainDocument8 pagesThe Neurobiology of Acute PainEduardoSilveiraNo ratings yet
- Alivio AmputadosDocument12 pagesAlivio AmputadosJAVIER ANDRÉS ROMEO OSESNo ratings yet
- Mechanisms of PainDocument3 pagesMechanisms of PainPembaca sejatiNo ratings yet
- Dentistry: Orofacial Pain: A ReviewDocument6 pagesDentistry: Orofacial Pain: A ReviewAstriAl-hutamiNo ratings yet
- TENS Mechanisms and Applications in Neuropathic PainDocument14 pagesTENS Mechanisms and Applications in Neuropathic PainAfnes AstrianiNo ratings yet
- (2015) Functional Neuroanatomy of Nociception and Pain-DikonversiDocument20 pages(2015) Functional Neuroanatomy of Nociception and Pain-DikonversiAnes ThesiaNo ratings yet
- Fact Sheet Painful Peripheral NeuropathyDocument6 pagesFact Sheet Painful Peripheral Neuropathyasdar fajrinNo ratings yet
- Phatofisiology of Pain PDFDocument8 pagesPhatofisiology of Pain PDFmohd nor muhammadNo ratings yet
- Sci Managing Pain PDFDocument16 pagesSci Managing Pain PDFPharmacist Ehab HammadNo ratings yet
- 2010 Acute Pain - MurphyDocument10 pages2010 Acute Pain - MurphypNo ratings yet
- MPDS-Multifactorial Etiology and Varied Pathophysiology: A ReviewDocument7 pagesMPDS-Multifactorial Etiology and Varied Pathophysiology: A Reviewsnehal jaiswalNo ratings yet
- Mechanisms and Manifestations in Musculoskeletal.4 PDFDocument17 pagesMechanisms and Manifestations in Musculoskeletal.4 PDFRodrigo Yarzábal RodríguezNo ratings yet
- Manual Therapy: Jo Nijs, Enrique Lluch Girb Es, Mari Lundberg, Anneleen Mal Iet, Michele SterlingDocument5 pagesManual Therapy: Jo Nijs, Enrique Lluch Girb Es, Mari Lundberg, Anneleen Mal Iet, Michele SterlingCentro Integral KndNo ratings yet
- IVDP & Spinal SurgeriesDocument7 pagesIVDP & Spinal Surgeriesbbpanicker67% (3)
- Neuropathic Orofacial PainDocument10 pagesNeuropathic Orofacial PainDeema FlembanNo ratings yet
- Epidural NeuroplastyDocument13 pagesEpidural NeuroplastyadityakurniantoNo ratings yet
- Pain ProcessingDocument12 pagesPain ProcessingKunal KatyayanNo ratings yet
- Nihms 396443Document12 pagesNihms 396443kickinghorse892No ratings yet
- Brachial Plexus InjuryDocument11 pagesBrachial Plexus InjuryNabil AhmedNo ratings yet
- Pathophysiology Back Pain: Daryo SoemitroDocument33 pagesPathophysiology Back Pain: Daryo SoemitroJohannah DaroNo ratings yet
- Update in Pain ManagementDocument51 pagesUpdate in Pain Managementeriep_keatnNo ratings yet
- % Dextrose Water As The Primary: Stanley K. H. Lam, Kenneth Dean Reeves, and An-Lin ChengDocument18 pages% Dextrose Water As The Primary: Stanley K. H. Lam, Kenneth Dean Reeves, and An-Lin ChengFloyd. BNo ratings yet
- or (See Spelling Differences From Greek ĮȞDocument4 pagesor (See Spelling Differences From Greek ĮȞOrene OnaicilefNo ratings yet
- Neuromodulation in Headache and Facial Pain Management: Principles, Rationale and Clinical DataFrom EverandNeuromodulation in Headache and Facial Pain Management: Principles, Rationale and Clinical DataGiorgio LambruNo ratings yet
- Peripheral Nerve Lesions: Nerve Surgery and Secondary Reconstructive RepairFrom EverandPeripheral Nerve Lesions: Nerve Surgery and Secondary Reconstructive RepairNo ratings yet
- Treatment of Cluster Headache: Acute and Preventive OptionsDocument3 pagesTreatment of Cluster Headache: Acute and Preventive OptionsharunNo ratings yet
- Pre-Employment Screening Form: Personal DetailsDocument7 pagesPre-Employment Screening Form: Personal DetailsLudmila PirtacNo ratings yet
- Managing Increased Intracranial PressureDocument13 pagesManaging Increased Intracranial PressureLudmila PirtacNo ratings yet
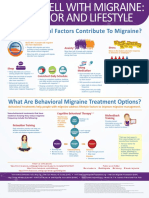
- Behavioral Infographic - V3 11x14Document1 pageBehavioral Infographic - V3 11x14Ludmila PirtacNo ratings yet
- Todd J. Albert and Alexander R. Vaccaro: Physical Examination of The SpineDocument1 pageTodd J. Albert and Alexander R. Vaccaro: Physical Examination of The SpineLudmila PirtacNo ratings yet
- Neuroexamportfolio 090413121923 Phpapp01Document154 pagesNeuroexamportfolio 090413121923 Phpapp01Ludmila PirtacNo ratings yet
- Retrobulbar NeuritisDocument5 pagesRetrobulbar NeuritisLudmila PirtacNo ratings yet
- Toxicological and Pharmacokinetic Properties of Sucralose 6 Acetate and Its Parent Sucralose in Vitro Screening AssaysDocument36 pagesToxicological and Pharmacokinetic Properties of Sucralose 6 Acetate and Its Parent Sucralose in Vitro Screening AssayswipiriNo ratings yet
- STDs-Sexually Transmitted Diseases & Infections GuideDocument11 pagesSTDs-Sexually Transmitted Diseases & Infections GuideYoon Pwint PhyuNo ratings yet
- 2008Document46 pages2008jimmyNo ratings yet
- Understanding The Carbon Dioxide Gaps: ReviewDocument9 pagesUnderstanding The Carbon Dioxide Gaps: ReviewLaura A M MNo ratings yet
- Chairside Diagnostic Kit - Dr. PriyaDocument25 pagesChairside Diagnostic Kit - Dr. PriyaDr. Priya PatelNo ratings yet
- Yukgehnaish Etal PhageLeadsDocument16 pagesYukgehnaish Etal PhageLeadsAugust ThomasenNo ratings yet
- A Modified Acid-Fast Staining Method For Rapid Detection ofDocument5 pagesA Modified Acid-Fast Staining Method For Rapid Detection ofWan HafizNo ratings yet
- Clinical Case NobelReplace Conical Connection Alessandro PozziDocument8 pagesClinical Case NobelReplace Conical Connection Alessandro PozziShyam BhatNo ratings yet
- D20rha25 2013-1Document2 pagesD20rha25 2013-1Icmi KadarsihNo ratings yet
- Placenta Previa GuideDocument7 pagesPlacenta Previa GuideMargaret AssilasNo ratings yet
- MICROPARA LEC Chapter 14 ReviewerDocument11 pagesMICROPARA LEC Chapter 14 ReviewerRen “Shel” ManaloNo ratings yet
- Implant ProstheticsDocument8 pagesImplant Prostheticssaggar65No ratings yet
- Indications For Nutritional Assessment in Childhood - UpToDateDocument28 pagesIndications For Nutritional Assessment in Childhood - UpToDatevaideeswari kumarNo ratings yet
- D.S.S. Aiims Prepration Test Series - 10 DR - SANJAY 7014964651 All Subject MCQDocument24 pagesD.S.S. Aiims Prepration Test Series - 10 DR - SANJAY 7014964651 All Subject MCQDr-Sanjay SinghaniaNo ratings yet
- Mifepristone & MisoprostolDocument6 pagesMifepristone & MisoprostolnanimadallaNo ratings yet
- STEAM INHALATION and NEBULIZATIONDocument4 pagesSTEAM INHALATION and NEBULIZATIONRenzo GabrielNo ratings yet
- Classic Laryngeal Mask Airway Insertion With Laryngoscope Mcgrath and Macintosh: A Case SeriesDocument3 pagesClassic Laryngeal Mask Airway Insertion With Laryngoscope Mcgrath and Macintosh: A Case SeriesYeyen AgustinNo ratings yet
- PG List 2016 17Document4 pagesPG List 2016 17Sundeep ArcheliesNo ratings yet
- 600 First أسئلة القصيمDocument165 pages600 First أسئلة القصيمFatema AlaaliNo ratings yet
- AMEBIASISDocument19 pagesAMEBIASISDika Herza Pratama100% (1)
- Angioedema 4Document18 pagesAngioedema 4Venosha GunasekaranNo ratings yet
- Bril (2002) - Validation of The Toronto Clinical Scoring System For Diabetic PolyneuropathyDocument5 pagesBril (2002) - Validation of The Toronto Clinical Scoring System For Diabetic PolyneuropathyRicky WatariNo ratings yet
- Ultrasound Supraclavicular Plexus Block Enhances Arteriovenous Fistula Blood Flow in ESRDDocument14 pagesUltrasound Supraclavicular Plexus Block Enhances Arteriovenous Fistula Blood Flow in ESRDaymankahlaNo ratings yet