You might also like
- Antecedentes INFECTOLOGYDocument40 pagesAntecedentes INFECTOLOGYDr. Claro RichardNo ratings yet
- Hvi 9 322Document3 pagesHvi 9 322Christina DavisNo ratings yet
- Lakew 2013Document4 pagesLakew 2013Ali AbidNo ratings yet
- CE (Ra1) F (SL) PF1 (AG SHU) PN (SL)Document2 pagesCE (Ra1) F (SL) PF1 (AG SHU) PN (SL)Asti NuriatiNo ratings yet
- 3 Meses VaricelaDocument4 pages3 Meses VaricelaNatalia CruzNo ratings yet
- Cong GengueDocument4 pagesCong GengueSiti Hidayatul FitriNo ratings yet
- Neonatal Bacterial InfectionDocument8 pagesNeonatal Bacterial InfectionNuurNo ratings yet
- Pediatrics IIDocument22 pagesPediatrics IICertificate SurrenderNo ratings yet
- Case Report An Infant With Congenital Rubella Syndrome in IndiaDocument2 pagesCase Report An Infant With Congenital Rubella Syndrome in IndiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Final Case Study SLDocument17 pagesFinal Case Study SLCharmie Mei Paredes-RoqueNo ratings yet
- Dengue Shock Syndrome in An Infant: Linda Aurpibul, Punyawee Khumlue, Satja Issaranggoon Na Ayuthaya, Peninnah OberdorferDocument4 pagesDengue Shock Syndrome in An Infant: Linda Aurpibul, Punyawee Khumlue, Satja Issaranggoon Na Ayuthaya, Peninnah OberdorferLIdya Goprani UmarNo ratings yet
- Neonatal Tetanus After Home Delivery 2019Document4 pagesNeonatal Tetanus After Home Delivery 2019astutikNo ratings yet
- 2002 23 132 Benjamin Gaston: Pediatr. RevDocument11 pages2002 23 132 Benjamin Gaston: Pediatr. RevDiego DíazNo ratings yet
- Enterovirus and Parechovirus Meningitis in InfantsDocument6 pagesEnterovirus and Parechovirus Meningitis in InfantsCarlos Peña PaterninaNo ratings yet
- Two Cases and A Review of Streptococcus Pyogenes Endocarditis in ChildrenDocument6 pagesTwo Cases and A Review of Streptococcus Pyogenes Endocarditis in ChildrenShigellaKimNo ratings yet
- Acute Pancreatitis in Children and Multisystemic Inflammatory Syndrome Post Covid Infection 19Document6 pagesAcute Pancreatitis in Children and Multisystemic Inflammatory Syndrome Post Covid Infection 19IJAR JOURNALNo ratings yet
- Proteus Mirabilis Case ReportDocument3 pagesProteus Mirabilis Case ReportMaria Chacón CarbajalNo ratings yet
- TI Croup Review Bjornson2005Document11 pagesTI Croup Review Bjornson2005mutimutimutiNo ratings yet
- Medicine Lec.8 - Viral InfectionDocument67 pagesMedicine Lec.8 - Viral Infection7fefdfbea1No ratings yet
- Varicella ZosterDocument10 pagesVaricella ZosterVu Nhat KhangNo ratings yet
- ARTICULO Estudio de CasoDocument14 pagesARTICULO Estudio de Casowhmticona2002No ratings yet
- SOGC Interim Guidance On Monkeypox Exposure For Pregnant PeopleDocument6 pagesSOGC Interim Guidance On Monkeypox Exposure For Pregnant PeopleariniNo ratings yet
- Neonatal Sepsis 2019.Document6 pagesNeonatal Sepsis 2019.Jean Paúl LópezNo ratings yet
- Peds InfectiousDocument8 pagesPeds InfectiousMohammad RammalNo ratings yet
- Gi QodDocument67 pagesGi QodAmmar AlnajjarNo ratings yet
- Crup Revision PDFDocument9 pagesCrup Revision PDFEmily Gabriela Caicedo RuedaNo ratings yet
- Basnyat 2021Document7 pagesBasnyat 2021nathanaellee92No ratings yet
- Respiratory Failure in Pregnant Women Infected by Swine-Origin Influenza A (H1N1)Document3 pagesRespiratory Failure in Pregnant Women Infected by Swine-Origin Influenza A (H1N1)meliabudiNo ratings yet
- 2002 23 132 Benjamin Gaston: Pediatrics in ReviewDocument11 pages2002 23 132 Benjamin Gaston: Pediatrics in ReviewLuis Fernando Rojas ArroyoNo ratings yet
- Paediatric Empyema: A Case Report and Literature ReviewDocument5 pagesPaediatric Empyema: A Case Report and Literature ReviewphobicmdNo ratings yet
- Fatal Pulmonary Infection With Respiratory SyncytiDocument5 pagesFatal Pulmonary Infection With Respiratory Syncyti21701101046 Devi NavilaNo ratings yet
- Pertusis 2Document21 pagesPertusis 2AbhishekNo ratings yet
- VZIG Recommendations High-Risk Varicella ExposureDocument19 pagesVZIG Recommendations High-Risk Varicella ExposureRajiv Kabad100% (1)
- Neonatal Varicella Case ReportDocument15 pagesNeonatal Varicella Case ReportArum Ardisa RiniNo ratings yet
- Late Presentation of Post Diphtheritic Myocarditis in A 15-Year MaleDocument3 pagesLate Presentation of Post Diphtheritic Myocarditis in A 15-Year MaleFaqih Alam RuqmanaNo ratings yet
- Coxsackievirus: Shandong University School of MedicineDocument26 pagesCoxsackievirus: Shandong University School of MedicineMonRedNo ratings yet
- Candidiasis NeonatalDocument9 pagesCandidiasis Neonatalgeorgi15685No ratings yet
- Neonatal Sepsis: Haematological PerspectivesDocument6 pagesNeonatal Sepsis: Haematological PerspectivesPUBLISHER JOURNALNo ratings yet
- Neonatal Sepsis 1219225703095484 9Document50 pagesNeonatal Sepsis 1219225703095484 9Ali FalihNo ratings yet
- Rare Case of Bronchiolitis Obliterans in a 21-Month-OldDocument3 pagesRare Case of Bronchiolitis Obliterans in a 21-Month-OldWelly ElvandariNo ratings yet
- Practice EssentialsDocument6 pagesPractice EssentialsdessydaswarNo ratings yet
- Respiratory Syncytial Virus Infection and Bronchiolitis: Practice GapsDocument14 pagesRespiratory Syncytial Virus Infection and Bronchiolitis: Practice GapsAnge CerónNo ratings yet
- Case ReportDocument3 pagesCase Reportchiquilon749No ratings yet
- 1) - Oral Exam Revealed A White Strawberry Tongue: Ecker, Habashy, SkopitDocument5 pages1) - Oral Exam Revealed A White Strawberry Tongue: Ecker, Habashy, SkopitAngela DuangchitNo ratings yet
- Opth 7 2249Document4 pagesOpth 7 2249amilyapraditaNo ratings yet
- Tetanus Neonatorum A Review of ManagementDocument5 pagesTetanus Neonatorum A Review of ManagementFrisiliakombaitan BaubauNo ratings yet
- Managing Tetanus Neonatorum: A Review of TreatmentDocument5 pagesManaging Tetanus Neonatorum: A Review of TreatmentFrisiliakombaitan BaubauNo ratings yet
- Management of Varicella in Neonates and Infants: (Penatalaksanaan Varisella Pada Neonatus Dan Bayi)Document35 pagesManagement of Varicella in Neonates and Infants: (Penatalaksanaan Varisella Pada Neonatus Dan Bayi)Farra PattipawaeNo ratings yet
- Kırşehir Ahi Evran Üniversitesi Sağlık Bilimleri Enstitüsü: Neonatal Sepsis & MeningitisDocument40 pagesKırşehir Ahi Evran Üniversitesi Sağlık Bilimleri Enstitüsü: Neonatal Sepsis & MeningitisAli FalihNo ratings yet
- Extremely Low Birth Weight (ELBW) InfantDocument48 pagesExtremely Low Birth Weight (ELBW) InfanthannanyusofNo ratings yet
- 0506hoENTEROVIRAL INFECTIONSDocument57 pages0506hoENTEROVIRAL INFECTIONSAmandeep SinghNo ratings yet
- Clinical Features and Outcomes of Children Admitted To The PICU Due To Rotavirus Infection GUNDocument5 pagesClinical Features and Outcomes of Children Admitted To The PICU Due To Rotavirus Infection GUNRoxana Ștefania DrăganNo ratings yet
- Jurnal NewDocument6 pagesJurnal NewTatik HandayaniNo ratings yet
- Chicken PoxDocument15 pagesChicken PoxQareeb KhanNo ratings yet
- Pediatrics: Pertussis, Varicella, and ZosterDocument14 pagesPediatrics: Pertussis, Varicella, and ZosterMy StoryNo ratings yet
- Dr. Vona 12Document5 pagesDr. Vona 12Agustiawan ImronNo ratings yet
- Rubella - Pediatrics - MSD Manual Professional EditionDocument4 pagesRubella - Pediatrics - MSD Manual Professional EditionSadia Shafique100% (1)
- Hyper-inflammatory Syndrome in a Child With COVID-19Document3 pagesHyper-inflammatory Syndrome in a Child With COVID-19Bala RamachandranNo ratings yet
- Bronchiolitis PDFDocument5 pagesBronchiolitis PDFjuniorebindaNo ratings yet
- Metabolic Factor - QuizDocument8 pagesMetabolic Factor - Quizsalva13100% (3)
- A Century of Biological-Weapons Programs (1915-2015) : Reviewing The EvidenceDocument26 pagesA Century of Biological-Weapons Programs (1915-2015) : Reviewing The EvidenceCaio CesarNo ratings yet
- Michigan State and Local Public Health COVID-19 Standard Operating ProceduresDocument19 pagesMichigan State and Local Public Health COVID-19 Standard Operating Proceduresfebri rizaldyNo ratings yet
- Week1 - NAILCARE (Sek)Document2 pagesWeek1 - NAILCARE (Sek)rhyzeneNo ratings yet
- Hsslive-Xi-Zoology-Rev-Test-4-Qn-By-Zta-Malappuram (1) - 230212 - 105754Document5 pagesHsslive-Xi-Zoology-Rev-Test-4-Qn-By-Zta-Malappuram (1) - 230212 - 105754എസ്സാർപി ഊരുചുറ്റൽ തുടരുന്നുNo ratings yet
- Cardiovascular SystemDocument26 pagesCardiovascular SystemRismawatiNo ratings yet
- IUM-First Aid, Safety Concept (1594)Document7 pagesIUM-First Aid, Safety Concept (1594)Risad ChoudhuryNo ratings yet
- PA y Depresión en Nepal 2017Document8 pagesPA y Depresión en Nepal 2017Alfredo PérezNo ratings yet
- Cardiopulmonary Resuscitation Update: Continuing Education ColumnDocument9 pagesCardiopulmonary Resuscitation Update: Continuing Education Columnkang soon cheolNo ratings yet
- Pain: Current Understanding of Assessment, Management, and Treatments (An Overview of Two Monographs)Document4 pagesPain: Current Understanding of Assessment, Management, and Treatments (An Overview of Two Monographs)National Pharmaceutical Council100% (1)
- Pentasa Tablets and Sachets PIDocument14 pagesPentasa Tablets and Sachets PIGeo GeoNo ratings yet
- Surgical SeiveDocument28 pagesSurgical SeiveSumeet PratapNo ratings yet
- Achigan-DakoTchokponhoueNDanikouetal 2015Document13 pagesAchigan-DakoTchokponhoueNDanikouetal 2015Juan Pablo Hernandez PaezNo ratings yet
- Physical Rehabilitation Assessment and TreatmentDocument1 pagePhysical Rehabilitation Assessment and Treatmentananya mishraNo ratings yet
- OVPR FY20Q1 Proposal List PDFDocument45 pagesOVPR FY20Q1 Proposal List PDFtsuregiNo ratings yet
- Ward DrugsDocument5 pagesWard DrugsMary Grace AgataNo ratings yet
- NP1 - ToprankDocument16 pagesNP1 - ToprankAllaiza Cristille100% (1)
- NefrologiDocument25 pagesNefrologifitriNo ratings yet
- The Ultimate Guide To Breathwork 2024Document8 pagesThe Ultimate Guide To Breathwork 2024lucicdNo ratings yet
- Specialized Group Homes For Persons With Severe or Profound Mental Retardation and Serious Problem Behaviour in EnglandDocument18 pagesSpecialized Group Homes For Persons With Severe or Profound Mental Retardation and Serious Problem Behaviour in EnglandDeborah RiskinNo ratings yet
- DVLA Null NewDocument1 pageDVLA Null NewTaniaNo ratings yet
- Medical History TemplateDocument4 pagesMedical History TemplateBrijesh KukretiNo ratings yet
- Arthritis OsteoarthritisDocument43 pagesArthritis OsteoarthritisMYMANo ratings yet
- Pharma Laboratory ExperimentsDocument34 pagesPharma Laboratory Experimentsapi-3748748100% (4)
- Fast Weight Loss TipsDocument2 pagesFast Weight Loss TipsLenny AnsirNo ratings yet
- Neet Ug Absolute Biology Vol 2Document22 pagesNeet Ug Absolute Biology Vol 2Rakesh Agarwal0% (1)
- b306cb470bc979ce717e6505073701baDocument78 pagesb306cb470bc979ce717e6505073701baHAIDAR RACHMANNo ratings yet
- Nuclear Medicine Therapy: Side Effects and Complications Luca GiovanellaDocument124 pagesNuclear Medicine Therapy: Side Effects and Complications Luca GiovanellaWhite HeartNo ratings yet
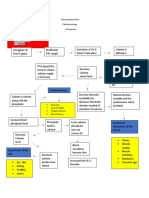
- Hypoparathyroidism PathophysiologyDocument1 pageHypoparathyroidism PathophysiologymaricarNo ratings yet
- Session 10. Review of Centric Records RECORDSDocument25 pagesSession 10. Review of Centric Records RECORDSbaraa.abdulrahman.23No ratings yet