You might also like
- Probation Period ReportDocument17 pagesProbation Period ReportMiranti Puspitasari0% (1)
- Basic Terms/Concepts IN Analytical ChemistryDocument53 pagesBasic Terms/Concepts IN Analytical ChemistrySheralyn PelayoNo ratings yet
- Reliability of Digital Orthodontic Setups: Monica S. Barreto Jorge Faber Carlos J. Vogel Telma M. AraujoDocument5 pagesReliability of Digital Orthodontic Setups: Monica S. Barreto Jorge Faber Carlos J. Vogel Telma M. AraujoMarlon Cespedes AlccaNo ratings yet
- da Silva 等 - 2023 - Comparison between clear aligners and 2 × 4 mechanDocument8 pagesda Silva 等 - 2023 - Comparison between clear aligners and 2 × 4 mechanDr.QiuNo ratings yet
- S - 2019 - Influence of Surgical Guide Support and Implant Site Location On Accuracy of Static Computer-Assisted Implant SurgeryDocument9 pagesS - 2019 - Influence of Surgical Guide Support and Implant Site Location On Accuracy of Static Computer-Assisted Implant SurgeryVõHoàngThủyTiênNo ratings yet
- Implant Positioning Errors in Freehand and Computeraided Placement Methods A Singleblind Clinical Comparative StudyDocument15 pagesImplant Positioning Errors in Freehand and Computeraided Placement Methods A Singleblind Clinical Comparative StudyDenisa CorneaNo ratings yet
- Marlière Et Al. 2018 ProsthodonticsDocument8 pagesMarlière Et Al. 2018 ProsthodonticsApril FloresNo ratings yet
- How Accurate Is Invisalign in Nonextraction Cases? Are Predicted Tooth Positions Achieved?Document7 pagesHow Accurate Is Invisalign in Nonextraction Cases? Are Predicted Tooth Positions Achieved?Mirza GlusacNo ratings yet
- Indirect Orthodontic Bonding - A Modified Technique For Improved Efficiency and PrecisionDocument10 pagesIndirect Orthodontic Bonding - A Modified Technique For Improved Efficiency and PrecisionSimon SitumorangNo ratings yet
- How Accurate Is Invisalign in Nonextraction Cases? Are Predicted Tooth Positions Achieved?Document7 pagesHow Accurate Is Invisalign in Nonextraction Cases? Are Predicted Tooth Positions Achieved?CLAUDIA PATRICIA ROSALES BASANTENo ratings yet
- Lingual Bracket Transfer Accuracy of Double VacuumDocument9 pagesLingual Bracket Transfer Accuracy of Double VacuumLipopapadaculiacan Marco OsunaNo ratings yet
- Accuracy of Bracket Placement by Orthodontists andDocument8 pagesAccuracy of Bracket Placement by Orthodontists andBethiza CamposNo ratings yet
- ARTICULO 1 Occlusal Contacts and Treatment With The Invisalign ApplianceDocument7 pagesARTICULO 1 Occlusal Contacts and Treatment With The Invisalign ApplianceJohanna TorresNo ratings yet
- Sarkis-Onofre2015 (Poste Fibra)Document6 pagesSarkis-Onofre2015 (Poste Fibra)Carmen AdamesNo ratings yet
- Evaluation of The Vertical Accuracy of Bracket Placement With The Boone GaugeDocument6 pagesEvaluation of The Vertical Accuracy of Bracket Placement With The Boone GaugeSoe San KyawNo ratings yet
- Clinical Oral Implants Res - 2018 - Tahmaseb - The Accuracy of Static Computer Aided Implant Surgery A Systematic ReviewDocument20 pagesClinical Oral Implants Res - 2018 - Tahmaseb - The Accuracy of Static Computer Aided Implant Surgery A Systematic ReviewOctavioJose DuarteFrenkyNo ratings yet
- Orthodontic Bonding A Direct ApproachDocument9 pagesOrthodontic Bonding A Direct ApproachAniket PotnisNo ratings yet
- Kjod 48 236Document9 pagesKjod 48 236Zaid DewachiNo ratings yet
- Zhou 2017Document13 pagesZhou 2017OctavioJose DuarteFrenkyNo ratings yet
- Transfer Accuracy of Vinyl Polysiloxane Trays For Indirect BondingDocument7 pagesTransfer Accuracy of Vinyl Polysiloxane Trays For Indirect BondingGABRIELA NIETO GONZALEZNo ratings yet
- Accuracy Comparison of Guided SurgeryDocument11 pagesAccuracy Comparison of Guided Surgerypolianass1109No ratings yet
- Lip Support 3Document7 pagesLip Support 3Pradusha RevuruNo ratings yet
- Assessment of Malalignment Factors Related To Invisalign Treatment Time Aided by Automated Imaging ProcessesDocument7 pagesAssessment of Malalignment Factors Related To Invisalign Treatment Time Aided by Automated Imaging ProcessesEzra ZuñigaNo ratings yet
- 65 - JPR - D - 20 - 00169 - 1Document7 pages65 - JPR - D - 20 - 00169 - 1Gt SolarcNo ratings yet
- Accuracy of Implant Placement With Computer-Guided SurgeryDocument15 pagesAccuracy of Implant Placement With Computer-Guided SurgerydentureNo ratings yet
- MARPE Guide A Case ReportDocument7 pagesMARPE Guide A Case ReportMarcelo ChinizacaNo ratings yet
- 1 s2.0 S1013905218301214 MainDocument7 pages1 s2.0 S1013905218301214 MainMostafa MedhatNo ratings yet
- Evaluación de Impresiones Dentales Por Métodos Convencionales y DigitalesDocument8 pagesEvaluación de Impresiones Dentales Por Métodos Convencionales y Digitalesdr. efrain camacho landerosNo ratings yet
- Ari 15Document6 pagesAri 15mariaNo ratings yet
- Complete Denture Rapid PrototypingDocument7 pagesComplete Denture Rapid Prototypingpopat78No ratings yet
- At-Home Vs In-Office Bleaching: A Systematic Review and Meta-AnalysisDocument16 pagesAt-Home Vs In-Office Bleaching: A Systematic Review and Meta-Analysisgerson fabian arangoNo ratings yet
- At Home Vs in Office Bleaching A Systematic Review and Meta AnalysisDocument16 pagesAt Home Vs in Office Bleaching A Systematic Review and Meta Analysismariandreina rodriguezNo ratings yet
- AutotransplanteDocument7 pagesAutotransplanteAlexandre PenaNo ratings yet
- Litreture Review 5Document6 pagesLitreture Review 5Daniel AtiehNo ratings yet
- Novellino 2013Document6 pagesNovellino 2013Glais FerrariNo ratings yet
- Ijbm 12 (3) Oa16Document5 pagesIjbm 12 (3) Oa16Juve EduardoNo ratings yet
- Diagnosis and Treatment Planning With 3-Dimensional Dentofacial RecordsDocument9 pagesDiagnosis and Treatment Planning With 3-Dimensional Dentofacial RecordsThibaut BossuytNo ratings yet
- Preparation and Evaluation of Orthodontic Setup PDFDocument20 pagesPreparation and Evaluation of Orthodontic Setup PDFLiezty VioLen'sNo ratings yet
- 1 s2.0 S1991790222000307 MainDocument2 pages1 s2.0 S1991790222000307 Maingfdsa jklNo ratings yet
- Art 1Document38 pagesArt 1Juan José Chacón BalderramaNo ratings yet
- Microperforacion Con Autoligado y ConvencionalDocument6 pagesMicroperforacion Con Autoligado y ConvencionalDiana ElíasNo ratings yet
- Indirect Orthodontic Bonding - A Modified Technique For Improved Efficiency and Precision PDFDocument10 pagesIndirect Orthodontic Bonding - A Modified Technique For Improved Efficiency and Precision PDFLuis Paipay SantosNo ratings yet
- Am J Orthod Dentofacial Orthop. 2016 150 3 425-35Document11 pagesAm J Orthod Dentofacial Orthop. 2016 150 3 425-35jonvargasNo ratings yet
- A Comparison of Two-Dimensional Prediction Tracing and A Virtual Reality Pa... - Discovery Service For Jordan Univ of Science & TechnologyDocument8 pagesA Comparison of Two-Dimensional Prediction Tracing and A Virtual Reality Pa... - Discovery Service For Jordan Univ of Science & TechnologyYazan AhedNo ratings yet
- EBD Nature Journal-Clinical Outcomes of Implant Supported-2023Document8 pagesEBD Nature Journal-Clinical Outcomes of Implant Supported-2023NARESHNo ratings yet
- Validity of A Manual Soft Tissue Profile Prediction Method Following Mandibular Setback OsteotomyDocument10 pagesValidity of A Manual Soft Tissue Profile Prediction Method Following Mandibular Setback OsteotomyMuhammad AleemNo ratings yet
- Comparison of Orthodontic Space Closure Using Micro-Osteoperforation and Passive Self-Ligating Appliances or Conventional Fixed Appliances: A Randomized Controlled TrialDocument6 pagesComparison of Orthodontic Space Closure Using Micro-Osteoperforation and Passive Self-Ligating Appliances or Conventional Fixed Appliances: A Randomized Controlled TrialakNo ratings yet
- Navi y GuiadaDocument14 pagesNavi y GuiadaDr.CdiazNo ratings yet
- Pi Is 0889540623004225Document10 pagesPi Is 0889540623004225Aaditya MallikNo ratings yet
- Eview Rticle: Journal of Advanced Medical and Dental Sciences ResearchDocument3 pagesEview Rticle: Journal of Advanced Medical and Dental Sciences ResearchSwathiLingannagariNo ratings yet
- BBRC 188Document6 pagesBBRC 188Egga AndiniNo ratings yet
- Kjod 52 6 420Document12 pagesKjod 52 6 420강북다인치과No ratings yet
- Comparison of Two Impression TechniqueDocument6 pagesComparison of Two Impression TechniqueAmar BhochhibhoyaNo ratings yet
- Dental Implant Navigation System Guide The Surgery Future: SciencedirectDocument9 pagesDental Implant Navigation System Guide The Surgery Future: SciencedirectrachmadyNo ratings yet
- Video Cephalometric Diagnosis (VCD) : A New Concept in Treatment Planning?Document17 pagesVideo Cephalometric Diagnosis (VCD) : A New Concept in Treatment Planning?Ismail BenameurNo ratings yet
- The Effect of Digital Diagnostic Setups On Orthodontic Treatment PlanningDocument8 pagesThe Effect of Digital Diagnostic Setups On Orthodontic Treatment PlanningAlejandro Aranzábal NavarreteNo ratings yet
- Biomechanics in Lingual Orthodontics What The Fut - 2018 - Seminars in Orthodon PDFDocument9 pagesBiomechanics in Lingual Orthodontics What The Fut - 2018 - Seminars in Orthodon PDFOmy J. CruzNo ratings yet
- Effectiveness and Efficacy of Thermoformed and 3D Printed PDFDocument7 pagesEffectiveness and Efficacy of Thermoformed and 3D Printed PDFGhimpu DanielaNo ratings yet
- S - 2019 - Influence of Implant Macrodesign and Insertion Connection Technology On The Accuracy of Static Computer-Assisted Implant SurgeryDocument7 pagesS - 2019 - Influence of Implant Macrodesign and Insertion Connection Technology On The Accuracy of Static Computer-Assisted Implant SurgeryVõHoàngThủyTiênNo ratings yet
- The Accuracy of Different Dental Impression Techniques For Implant-Supported Dental Prostheses: A Systematic Review and Meta - AnalysisDocument19 pagesThe Accuracy of Different Dental Impression Techniques For Implant-Supported Dental Prostheses: A Systematic Review and Meta - AnalysisAnonymous AyxIccS4aXNo ratings yet
- 2020 - Stereolithographic Surgical Guide With A Combination of Tooth and Bone SupportDocument13 pages2020 - Stereolithographic Surgical Guide With A Combination of Tooth and Bone SupportVõHoàngThủyTiênNo ratings yet
- Machine Learning in DentistryFrom EverandMachine Learning in DentistryChing-Chang KoNo ratings yet
- 2.1 SamplingDocument44 pages2.1 SamplingVishal SharmaNo ratings yet
- Theories of GrowthDocument157 pagesTheories of GrowthVishal SharmaNo ratings yet
- Safe Sites For Orthodontic Miniscrew InsertionDocument9 pagesSafe Sites For Orthodontic Miniscrew InsertionDa Hae SungNo ratings yet
- Ocr 12193 PDFDocument7 pagesOcr 12193 PDFVishal SharmaNo ratings yet
- Angle Orthod. 2018 88 4 435-41Document7 pagesAngle Orthod. 2018 88 4 435-41brookortontiaNo ratings yet
- Effects of Rapid Maxillary Expansion On Upper Airway Volume: A Three-Dimensional Cone-Beam Computed Tomography StudyDocument7 pagesEffects of Rapid Maxillary Expansion On Upper Airway Volume: A Three-Dimensional Cone-Beam Computed Tomography StudyVishal SharmaNo ratings yet
- Flexible and Biocompatible High-Performance Solid-State Micro-Battery For Implantable Orthodontic SystemDocument8 pagesFlexible and Biocompatible High-Performance Solid-State Micro-Battery For Implantable Orthodontic SystemVishal SharmaNo ratings yet
- Seminar: Treatment Planning in Orthodontic PatientsDocument105 pagesSeminar: Treatment Planning in Orthodontic PatientsVishal SharmaNo ratings yet
- Crowding 180601115625 PDFDocument109 pagesCrowding 180601115625 PDFVishal SharmaNo ratings yet
- CD Class 270117Document233 pagesCD Class 270117Vishal SharmaNo ratings yet
- SSC Gr8 Biotech Q4 Module 1 WK 1 - v.01-CC-released-09May2021Document22 pagesSSC Gr8 Biotech Q4 Module 1 WK 1 - v.01-CC-released-09May2021Ivy JeanneNo ratings yet
- Plan Lectie Clasa 5 D HaineDocument5 pagesPlan Lectie Clasa 5 D HaineCristina GrapinoiuNo ratings yet
- Construction Project - Life Cycle PhasesDocument4 pagesConstruction Project - Life Cycle Phasesaymanmomani2111No ratings yet
- Pearson R CorrelationDocument2 pagesPearson R CorrelationAira VillarinNo ratings yet
- PDS DeltaV SimulateDocument9 pagesPDS DeltaV SimulateJesus JuarezNo ratings yet
- Nominal GroupDocument3 pagesNominal GroupSrourNo ratings yet
- Strategic Management SlidesDocument150 pagesStrategic Management SlidesIqra BilalNo ratings yet
- DTR Testastretta Valve Adjustment ProcedureDocument10 pagesDTR Testastretta Valve Adjustment ProcedureTony LamprechtNo ratings yet
- Amity School of Business:, Semester IV Research Methodology and Report Preparation Dr. Deepa KapoorDocument23 pagesAmity School of Business:, Semester IV Research Methodology and Report Preparation Dr. Deepa KapoorMayank TayalNo ratings yet
- Exploring-Engineering-And-Technology-Grade-6 1Document5 pagesExploring-Engineering-And-Technology-Grade-6 1api-349870595No ratings yet
- Sheet-Metal Forming Processes: Group 9 PresentationDocument90 pagesSheet-Metal Forming Processes: Group 9 PresentationjssrikantamurthyNo ratings yet
- OTP User Manual For English) v1,0Document15 pagesOTP User Manual For English) v1,0auyinNo ratings yet
- FIR FliterDocument10 pagesFIR FliterasfsfsafsafasNo ratings yet
- RSW - F - 01 " ": Building UtilitiesDocument4 pagesRSW - F - 01 " ": Building Utilities62296bucoNo ratings yet
- 11-Rubber & PlasticsDocument48 pages11-Rubber & PlasticsJack NgNo ratings yet
- Statistical Process Control and Process Capability PPT EXPLANATIONDocument2 pagesStatistical Process Control and Process Capability PPT EXPLANATIONJohn Carlo SantiagoNo ratings yet
- VOTOL EMController Manual V2.0Document18 pagesVOTOL EMController Manual V2.0Nandi F. ReyhanNo ratings yet
- The University of The West Indies: Application For First Degree, Associate Degree, Diploma and Certificate ProgrammesDocument5 pagesThe University of The West Indies: Application For First Degree, Associate Degree, Diploma and Certificate ProgrammesDavid Adeyinka RamgobinNo ratings yet
- AP8 Q4 Ip9 V.02Document7 pagesAP8 Q4 Ip9 V.02nikka suitadoNo ratings yet
- Arudha PDFDocument17 pagesArudha PDFRakesh Singh100% (1)
- Does Adding Salt To Water Makes It Boil FasterDocument1 pageDoes Adding Salt To Water Makes It Boil Fasterfelixcouture2007No ratings yet
- Code of Ethics For Civil Engineers PiceDocument3 pagesCode of Ethics For Civil Engineers PiceEdwin Ramos Policarpio100% (3)
- Kübler 5800-5820 - enDocument5 pagesKübler 5800-5820 - enpomsarexnbNo ratings yet
- Philo Q2 Lesson 5Document4 pagesPhilo Q2 Lesson 5Julliana Patrice Angeles STEM 11 RUBYNo ratings yet
- FS-1040 FS-1060DN: Parts ListDocument23 pagesFS-1040 FS-1060DN: Parts List1980cvvrNo ratings yet
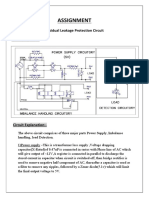
- Assignment: Residual Leakage Protection Circuit Circuit DiagramDocument2 pagesAssignment: Residual Leakage Protection Circuit Circuit DiagramShivam ShrivastavaNo ratings yet
- Pyramid Type Plate Bending MachineDocument10 pagesPyramid Type Plate Bending MachineAswin JosephNo ratings yet
- Designed For Severe ServiceDocument28 pagesDesigned For Severe ServiceAnthonyNo ratings yet