You might also like
- MGH Whitebook 2021-2022Document258 pagesMGH Whitebook 2021-2022Gabriel Braga Villa100% (1)
- Test Bank For Discovering Behavioral Neuroscience An Introduction To Biological Psychology 3rd EditionDocument44 pagesTest Bank For Discovering Behavioral Neuroscience An Introduction To Biological Psychology 3rd EditionKevin Brown100% (43)
- Cardiology Case 1Document2 pagesCardiology Case 1vil62650% (2)
- PRS Ear Instillation - GlovaDocument3 pagesPRS Ear Instillation - GlovaAndrea Colleen GlovaNo ratings yet
- Examinarea Clinică in Afecţiuni Ale Aparatului CardiovascularDocument49 pagesExaminarea Clinică in Afecţiuni Ale Aparatului CardiovascularFranceska LtkNo ratings yet
- Congestive Heart FailureDocument8 pagesCongestive Heart Failureiancel_038893% (27)
- NCM 109 Lecture: Nursing Care of A Child With Hematologic DisorderDocument95 pagesNCM 109 Lecture: Nursing Care of A Child With Hematologic DisorderAmiscua Pauline AnneNo ratings yet
- Cardiovascular System Anatomy and PhysiologyDocument14 pagesCardiovascular System Anatomy and PhysiologyKIRSTEN CHAVEZ100% (1)
- (MIDTERM) NCM-206 (Pharmacology) ReviewerDocument26 pages(MIDTERM) NCM-206 (Pharmacology) ReviewerASTR4 BABY100% (1)
- Cardiovascular Disorders & PregnancyDocument6 pagesCardiovascular Disorders & PregnancyChelcee MagsinoNo ratings yet
- Ncp-Risk ForDocument2 pagesNcp-Risk ForValledor Ian MosesNo ratings yet
- Lecture NCM 109Document11 pagesLecture NCM 109Evangeline Anne MacanasNo ratings yet
- TOF (Pathophysiology)Document4 pagesTOF (Pathophysiology)Doreen Claire M. WallangNo ratings yet
- Spontaneous AbortionDocument8 pagesSpontaneous Abortionsaber_fate_11No ratings yet
- Coxa Plana PathophysiologyDocument1 pageCoxa Plana Pathophysiologymiss RN100% (4)
- Abdominal AssessmentDocument2 pagesAbdominal AssessmentMuhammad Fahrin AzhariNo ratings yet
- NCM 104 Case Study NCP FinalDocument40 pagesNCM 104 Case Study NCP FinalKyle JingcoNo ratings yet
- Activity 3 Case Scenario GcsDocument3 pagesActivity 3 Case Scenario GcsDfatsbsNo ratings yet
- P1 P2 Mastery Examination Reviewer in FNP LECTUREDocument34 pagesP1 P2 Mastery Examination Reviewer in FNP LECTUREMary Ann G. CorsanesNo ratings yet
- Chapter 40. Nursing Care of A Child With Respiratory Disorder TermsDocument3 pagesChapter 40. Nursing Care of A Child With Respiratory Disorder TermsJœnríčk AzueloNo ratings yet
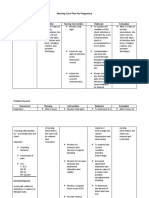
- Nursing Care Plan For Pregnancy: Risk Diagnosis Nursing Diagnosis Objective Nursing Intervention Rationale EvaluationDocument2 pagesNursing Care Plan For Pregnancy: Risk Diagnosis Nursing Diagnosis Objective Nursing Intervention Rationale EvaluationCheska PalomaNo ratings yet
- Concept Map of DMDocument1 pageConcept Map of DMRobert Timothy YapNo ratings yet
- Quiz 3 Fetal CirculationDocument1 pageQuiz 3 Fetal CirculationDENNIS N. MUÑOZNo ratings yet
- Nursing Care of The Family Experiencing A Sudden Pregnancy ComplicationDocument7 pagesNursing Care of The Family Experiencing A Sudden Pregnancy ComplicationDacillo GailleNo ratings yet
- Ncma219 Ob Lec: BSN 2Nd Year 2Nd Semester Prelim 2022: Bachelor of Science in Nursing 2YBDocument59 pagesNcma219 Ob Lec: BSN 2Nd Year 2Nd Semester Prelim 2022: Bachelor of Science in Nursing 2YBEARL GERALD RICAFRANCANo ratings yet
- PartographDocument3 pagesPartographAlliana O. BalansayNo ratings yet
- Mark Fredderick R. Abejo RN, MAN: Maternal and Child Nursing BulletsDocument9 pagesMark Fredderick R. Abejo RN, MAN: Maternal and Child Nursing BulletsCrystal Ann Monsale TadiamonNo ratings yet
- DDSTDocument61 pagesDDSTji payNo ratings yet
- Spina Bifida, Meningocele MyelomeningoceleDocument1 pageSpina Bifida, Meningocele MyelomeningocelesmilingstarsNo ratings yet
- Laguna, Alleja Rose M March 30,2021 BSN 2E DR Rotation (Prof. Oton)Document2 pagesLaguna, Alleja Rose M March 30,2021 BSN 2E DR Rotation (Prof. Oton)Alleja Rose M. LAGUNANo ratings yet
- Abortion and Ectopic PregnancyDocument3 pagesAbortion and Ectopic PregnancyJefelson Eu Palaña NahidNo ratings yet
- Guided Answers For NCM 109 Oral RevalidaDocument6 pagesGuided Answers For NCM 109 Oral RevalidaBenedict Reyes, Jr.No ratings yet
- Pa Tho PhysiologyDocument1 pagePa Tho PhysiologyEiztirfNo ratings yet
- Hereditary SpherocytosisDocument39 pagesHereditary SpherocytosisjoannaNo ratings yet
- NCLXDocument5 pagesNCLXkhadeejakhurshidNo ratings yet
- n213 Unit 2 BDocument390 pagesn213 Unit 2 BJeonghwa Park100% (1)
- Case Study HydrocephalusDocument19 pagesCase Study HydrocephalusJane Mae JesoroNo ratings yet
- Pre EclampsiaDocument13 pagesPre EclampsiaEniamrahs DnalonNo ratings yet
- Pathophysiology of ThrombophlebitisDocument3 pagesPathophysiology of ThrombophlebitisJennifer ArdeNo ratings yet
- Birth Asphyxia: by Anne E. Odaro MCM/2017/69852Document26 pagesBirth Asphyxia: by Anne E. Odaro MCM/2017/69852ElvisNo ratings yet
- Chapter 9: Nursing Care During Normal Pregnancy and Care of The Developing FetusDocument8 pagesChapter 9: Nursing Care During Normal Pregnancy and Care of The Developing FetusAlyssaGrandeMontimor100% (1)
- Pathophysiology of Cerebral PalsyDocument5 pagesPathophysiology of Cerebral PalsydaisibanNo ratings yet
- PATHOPHYSIO (Megaloblastic Anemia)Document3 pagesPATHOPHYSIO (Megaloblastic Anemia)Giselle EstoquiaNo ratings yet
- Sterloie Inn MCN AssignmentDocument15 pagesSterloie Inn MCN AssignmentIan Mizzel A. DulfinaNo ratings yet
- Oral Revalida - H-MoleDocument1 pageOral Revalida - H-MoleMary Loise Villegas0% (1)
- NSDDocument44 pagesNSDabyssodeep100% (1)
- Quiz 7. NCM 116 For StudentsDocument4 pagesQuiz 7. NCM 116 For StudentsZayne Lucas Gabrielle TadiamonNo ratings yet
- The Lived Experiences of Thriving Family Caregivers of Persons With Autism Spectrum DisorderDocument11 pagesThe Lived Experiences of Thriving Family Caregivers of Persons With Autism Spectrum DisorderPsychology and Education: A Multidisciplinary JournalNo ratings yet
- NCM 109 Prelims ReviewerDocument2 pagesNCM 109 Prelims ReviewerReyna Chame GarcinezNo ratings yet
- Apgar Scoring ActivityDocument3 pagesApgar Scoring ActivityAshley SorgenNo ratings yet
- Care of Clients With Problems in Oxygenation (Part 2)Document88 pagesCare of Clients With Problems in Oxygenation (Part 2)mikErlhNo ratings yet
- Pregnancy Induced HypertensionDocument3 pagesPregnancy Induced HypertensionunagraciaNo ratings yet
- Case PresentationDocument10 pagesCase PresentationWina Hanriyani0% (1)
- Health Education - Reviewer (Prelims)Document9 pagesHealth Education - Reviewer (Prelims)Frances Nicole FloresNo ratings yet
- NCM 112 Periop QuizletDocument13 pagesNCM 112 Periop QuizletZhoey ReyesNo ratings yet
- Oral RevalidaDocument14 pagesOral RevalidaAyaBasilioNo ratings yet
- Iv. Review of Anatomy and Physiology Figure 1. The Immune SystemDocument7 pagesIv. Review of Anatomy and Physiology Figure 1. The Immune SystemNejie Zarrah Diaz100% (1)
- Hemolytic AnemiaDocument46 pagesHemolytic AnemiaSjerwin Anthony Gianan100% (1)
- Grand Case (Sigmoid Adenocarcinoma)Document24 pagesGrand Case (Sigmoid Adenocarcinoma)Leslee Amor EspirituNo ratings yet
- Origin and Development of Organ Systems NotesDocument4 pagesOrigin and Development of Organ Systems NotesimnasNo ratings yet
- Topic # 2 PartographDocument42 pagesTopic # 2 PartographJayrelle D. Safran100% (1)
- Cardio and Hema - DR PueyoDocument161 pagesCardio and Hema - DR Pueyoapi-3735995100% (2)
- Disorders: By: Nur Hanisah Binti ZainorenDocument53 pagesDisorders: By: Nur Hanisah Binti ZainorenJœnríčk AzueloNo ratings yet
- Acute Care and Emergency General Surgery in Patients With Chronic Liver Disease: How Can We Optimize Perioperative Care? A Review of The LiteratureDocument9 pagesAcute Care and Emergency General Surgery in Patients With Chronic Liver Disease: How Can We Optimize Perioperative Care? A Review of The LiteratureJœnríčk AzueloNo ratings yet
- Chapter 52. Nursing Care of The Child With A Traumatic Injury TermsDocument8 pagesChapter 52. Nursing Care of The Child With A Traumatic Injury TermsJœnríčk AzueloNo ratings yet
- Chapter 51. Nursing Care of The Child With A Musculoskeletal Disorder TermsDocument3 pagesChapter 51. Nursing Care of The Child With A Musculoskeletal Disorder TermsJœnríčk AzueloNo ratings yet
- 31 Rathnayaky Originial 9 3Document13 pages31 Rathnayaky Originial 9 3Jœnríčk AzueloNo ratings yet
- MCN CompiledDocument71 pagesMCN CompiledJœnríčk AzueloNo ratings yet
- Chapter 43. Nursing Care of The Child With An Infectious Disorder TermsDocument1 pageChapter 43. Nursing Care of The Child With An Infectious Disorder TermsJœnríčk AzueloNo ratings yet
- Chapter 25Document63 pagesChapter 25Jœnríčk AzueloNo ratings yet
- Nursing Care of The Child With A Hematologic Disorder TermsDocument8 pagesNursing Care of The Child With A Hematologic Disorder TermsJœnríčk AzueloNo ratings yet
- Chapter 43. Nursing Care of The Child With An Infectious Disorder TermsDocument1 pageChapter 43. Nursing Care of The Child With An Infectious Disorder TermsJœnríčk AzueloNo ratings yet
- Chapter 40. Nursing Care of A Child With Respiratory Disorder TermsDocument3 pagesChapter 40. Nursing Care of A Child With Respiratory Disorder TermsJœnríčk AzueloNo ratings yet
- Keep Safe Everyone. God Bless 2C.: 3. Deadline For This Activity Will Be On Sunday March 29, 2020 11:59PMDocument10 pagesKeep Safe Everyone. God Bless 2C.: 3. Deadline For This Activity Will Be On Sunday March 29, 2020 11:59PMJœnríčk AzueloNo ratings yet
- C. The Disengagement Theory D. The Personal Meaning TheoryDocument2 pagesC. The Disengagement Theory D. The Personal Meaning TheoryJœnríčk AzueloNo ratings yet
- Chapter 43. Nursing Care of The Child With An Infectious Disorder TermsDocument1 pageChapter 43. Nursing Care of The Child With An Infectious Disorder TermsJœnríčk AzueloNo ratings yet
- Situation 15. The Community Health Nurse Prepares/participate in The Preparation of TheDocument3 pagesSituation 15. The Community Health Nurse Prepares/participate in The Preparation of TheJœnríčk AzueloNo ratings yet
- Situation 14. The Department of Health Implements Various Health Programs and ProjectsDocument2 pagesSituation 14. The Department of Health Implements Various Health Programs and ProjectsJœnríčk AzueloNo ratings yet
- Chapter 42. Nursing Care of The Child With An Immune Disorder TermsDocument2 pagesChapter 42. Nursing Care of The Child With An Immune Disorder TermsJœnríčk AzueloNo ratings yet
- Part I. Awareness and Knowledge On HIV/AIDS and PLHIV General KnowledgeDocument2 pagesPart I. Awareness and Knowledge On HIV/AIDS and PLHIV General KnowledgeJœnríčk AzueloNo ratings yet
- MCN ReportDocument21 pagesMCN ReportJœnríčk AzueloNo ratings yet
- Cover PageDocument1 pageCover PageJœnríčk AzueloNo ratings yet
- CaseDocument4 pagesCaseJœnríčk AzueloNo ratings yet
- NANDA Nursing Diagnosis Nanda Definition Cues/Defining Characteristics Nursing Outcomes Classification (NOC) Nursing Interventions Classification (NIC) EvaluationDocument3 pagesNANDA Nursing Diagnosis Nanda Definition Cues/Defining Characteristics Nursing Outcomes Classification (NOC) Nursing Interventions Classification (NIC) EvaluationJœnríčk AzueloNo ratings yet
- NANDA Nursing Diagnosis Nanda Definition Cues/Defining Characteristics Nursing Outcomes Classification (NOC) Nursing Interventions Classification (NIC) EvaluationDocument3 pagesNANDA Nursing Diagnosis Nanda Definition Cues/Defining Characteristics Nursing Outcomes Classification (NOC) Nursing Interventions Classification (NIC) EvaluationJœnríčk AzueloNo ratings yet
- Suprarenal GlandDocument13 pagesSuprarenal GlandAaa JjjjNo ratings yet
- Case Study 3 - HCVDDocument12 pagesCase Study 3 - HCVDJilkiah Mae Alfoja CampomanesNo ratings yet
- Fetal CirculationDocument16 pagesFetal CirculationArunashree ajayNo ratings yet
- Persistent Left Superior Vena Cava PLSVCDocument2 pagesPersistent Left Superior Vena Cava PLSVCEdit KirályNo ratings yet
- Basic Ecg Interpretation Powerpoint For The OsceDocument20 pagesBasic Ecg Interpretation Powerpoint For The OsceCHARLOTTE DU PREEZNo ratings yet
- Nursing Care Plan Evaluation FormDocument7 pagesNursing Care Plan Evaluation FormSusmita BeheraNo ratings yet
- ECG BasicsDocument15 pagesECG Basicsrohitmeena2889No ratings yet
- Dog Dissection ProcedureDocument20 pagesDog Dissection ProcedureChristine Joyce NavarroNo ratings yet
- Celecoxib, Etoricoxib, DiclofenacDocument13 pagesCelecoxib, Etoricoxib, Diclofenacbaitur rohmahNo ratings yet
- Hodis 2016Document11 pagesHodis 2016Ibrahim Al ShantiNo ratings yet
- POCUSDocument10 pagesPOCUSSMIBA MedicinaNo ratings yet
- Orthopaedic MCQDocument11 pagesOrthopaedic MCQShiKid COMIX-GAMENo ratings yet
- Etihad Airlines Medical FormDocument9 pagesEtihad Airlines Medical FormVidu ChaNo ratings yet
- Tutorial 4 Jan 2016 QPDocument2 pagesTutorial 4 Jan 2016 QPchinNo ratings yet
- PDF Atlas of Endovascular Venous Surgery Almeida Ebook Full ChapterDocument53 pagesPDF Atlas of Endovascular Venous Surgery Almeida Ebook Full Chaptercynthia.brazill243100% (4)
- PRADAXA: Dosing Guide: Starting Patients On PRADAXADocument2 pagesPRADAXA: Dosing Guide: Starting Patients On PRADAXAPapp Szodorai BeátaNo ratings yet
- Anti-Anginal and Antiischemic Drugs: Dr. Pradeepa H D Clinical PharmacologistDocument25 pagesAnti-Anginal and Antiischemic Drugs: Dr. Pradeepa H D Clinical PharmacologistpradeephdNo ratings yet
- NON CARDIAC SURGERY. ESC POCKET GLS.2022. Larger FontDocument63 pagesNON CARDIAC SURGERY. ESC POCKET GLS.2022. Larger FontGeoNo ratings yet
- PacemakerDocument5 pagesPacemakerMuhammad Umer SaeedNo ratings yet
- Choledochal CystDocument16 pagesCholedochal CystNico HernándezNo ratings yet
- 250 SCFHS-USMLE QuestionsDocument39 pages250 SCFHS-USMLE QuestionsAhmedNo ratings yet
- Pulmonary HypertensionDocument36 pagesPulmonary HypertensionDiana_anca6100% (2)
- Etiology Predisposing Factors Actual Findings Implication FactorsDocument3 pagesEtiology Predisposing Factors Actual Findings Implication FactorsJIMENEZ, TRISHA MARIE D.No ratings yet
- Biochemistry LRR InicetDocument290 pagesBiochemistry LRR InicetSendhilNo ratings yet
- Presentation 1Document15 pagesPresentation 1Sanjeevini KNo ratings yet
- Acute Exacerbation of COPDDocument21 pagesAcute Exacerbation of COPDArmaanjeet SinghNo ratings yet
- DRUG STUDY AdenosineDocument1 pageDRUG STUDY Adenosinejulesubayubay5428100% (1)
- Primary Sclerosing Cholangitis-JR KrisnaDocument16 pagesPrimary Sclerosing Cholangitis-JR Krisnamerlyn angelinaNo ratings yet