You might also like
- Galactic Handbook and Synchronized MeditationsDocument91 pagesGalactic Handbook and Synchronized Meditationslapiton100% (10)
- Load-Out and Sea-Fastening ProcedureDocument17 pagesLoad-Out and Sea-Fastening ProcedureAdaghara100% (2)
- Ceph Reference ArchitectureDocument12 pagesCeph Reference ArchitectureGermgmaan100% (1)
- Sugar Sweetened Beverages: Factors Affecting Consumption and Level of Awareness On Its Effects To Health Among Nursing Students of Mindanao State University-SuluDocument8 pagesSugar Sweetened Beverages: Factors Affecting Consumption and Level of Awareness On Its Effects To Health Among Nursing Students of Mindanao State University-SuluPsychology and Education: A Multidisciplinary JournalNo ratings yet
- Engineering StudiesDocument4 pagesEngineering StudiesSamuel PhegelloNo ratings yet
- HydrotherapyDocument7 pagesHydrotherapyGialys MoretaNo ratings yet
- Useful Medications For Oral Conditions: AnalgesicsDocument7 pagesUseful Medications For Oral Conditions: AnalgesicsAswathyNo ratings yet
- Amco Veba Marine - Brochure - LRDocument24 pagesAmco Veba Marine - Brochure - LRHươngTpuNo ratings yet
- OrlDocument186 pagesOrlMuli MaroshiNo ratings yet
- Policy On Snacks and Sugar-Sweetened BeveragesDocument2 pagesPolicy On Snacks and Sugar-Sweetened BeveragesمعتزباللهNo ratings yet
- Recomendaciones de DietaDocument3 pagesRecomendaciones de DietaAna CristernaNo ratings yet
- Free Sugar Intake From Snacks and Beverages in Canadian Preschool-And Toddler-Aged Children: A Cross-Sectional StudyDocument9 pagesFree Sugar Intake From Snacks and Beverages in Canadian Preschool-And Toddler-Aged Children: A Cross-Sectional StudySYERLI PERMATA HENITA SARINo ratings yet
- Grupo 3Document9 pagesGrupo 3Michel Vilarinho CarvalhoNo ratings yet
- Soft Drinks and School-Age ChildrenDocument6 pagesSoft Drinks and School-Age ChildrenkalikNo ratings yet
- Factors Associated With Water Consumption Among Children: A Systematic ReviewDocument14 pagesFactors Associated With Water Consumption Among Children: A Systematic ReviewMohammed OmarNo ratings yet
- Practical ResearchDocument8 pagesPractical ResearchRomar CambaNo ratings yet
- Group 3 StsDocument14 pagesGroup 3 Stskyrelle atentarNo ratings yet
- Edited Sugary Drinks and Child ObesityDocument4 pagesEdited Sugary Drinks and Child ObesityChristopher Rodriguez PerezNo ratings yet
- Where Are We With Smoothies A Review of The Latest Guidelines Nutritionalgaps and Evidence 2155 9600 1000632Document5 pagesWhere Are We With Smoothies A Review of The Latest Guidelines Nutritionalgaps and Evidence 2155 9600 1000632pololeoextremoeyyNo ratings yet
- Australian Dental Journal: Sugary Drink Consumption and Dental Caries in New South Wales TeenagersDocument7 pagesAustralian Dental Journal: Sugary Drink Consumption and Dental Caries in New South Wales TeenagersRega RegiawanNo ratings yet
- EditedDocument8 pagesEditedjosephmainam9No ratings yet
- Nihms 1503143 Niños y CariesDocument20 pagesNihms 1503143 Niños y CariesLuis franNo ratings yet
- Nihms-1503143-Niños y CariesDocument20 pagesNihms-1503143-Niños y CariesLuis franNo ratings yet
- 1 s2.0 S1499404621006886 MainDocument9 pages1 s2.0 S1499404621006886 MainTarannum TrishaNo ratings yet
- Evaluating The Effects of Sugary Beverage Consumption On Child Health in Ghana-JosephineDocument21 pagesEvaluating The Effects of Sugary Beverage Consumption On Child Health in Ghana-JosephineJosephine NarteyNo ratings yet
- VanEpps Roberto Beverage Warnings-1Document9 pagesVanEpps Roberto Beverage Warnings-1Jenika ShahNo ratings yet
- Action On Salt ResponseDocument2 pagesAction On Salt Responsetijak88617No ratings yet
- EqweDocument6 pagesEqweKaren ArganosaNo ratings yet
- Drinking Water Linked To Fewer Sugary Drinks. ExerciseDocument3 pagesDrinking Water Linked To Fewer Sugary Drinks. ExerciseRafael FreitasNo ratings yet
- Making The Healthy Choice The Easy Choice in SchoolsDocument36 pagesMaking The Healthy Choice The Easy Choice in SchoolsProject PANo ratings yet
- Water Fluoridation Reduces Impact of SSB Consumption on Tooth DecayDocument7 pagesWater Fluoridation Reduces Impact of SSB Consumption on Tooth DecaygdpratiwiNo ratings yet
- Ni Hms 538419Document20 pagesNi Hms 538419Luis franNo ratings yet
- Parents' Preferences and Perceptions of Their Children's Consumption of Sugar and Non-Nutritive Sugar SubstitutesDocument8 pagesParents' Preferences and Perceptions of Their Children's Consumption of Sugar and Non-Nutritive Sugar SubstitutesCardenas JuanNo ratings yet
- Simple Interventions To Improve Healthy Eating Behaviors in The School CafeteriaDocument12 pagesSimple Interventions To Improve Healthy Eating Behaviors in The School CafeteriaHusni maiyantiNo ratings yet
- Research PaperDocument15 pagesResearch PaperKeithryn Lee OrtizNo ratings yet
- Morgan 2013Document6 pagesMorgan 2013Lucia HerediaNo ratings yet
- The Role of Schools in Preventing Childhood ObesityDocument4 pagesThe Role of Schools in Preventing Childhood ObesityEMMANUELNo ratings yet
- Association between early childhood caries and intake of 100% fruit juice among US preschoolersDocument8 pagesAssociation between early childhood caries and intake of 100% fruit juice among US preschoolersJavier Farias VeraNo ratings yet
- My Research ProposalDocument6 pagesMy Research ProposalJoseph AddoNo ratings yet
- The Importance and Challenges of School Feeding: Literature ReviewDocument13 pagesThe Importance and Challenges of School Feeding: Literature ReviewIJAERS JOURNALNo ratings yet
- Shagun Paper 3Document9 pagesShagun Paper 3shagun khandelwalNo ratings yet
- Sugar Drink Consumption Fact SheetDocument3 pagesSugar Drink Consumption Fact SheetMarcosNo ratings yet
- 3 Popular Foods in Your Fridge That Could Damage Your HealthDocument15 pages3 Popular Foods in Your Fridge That Could Damage Your Healthtopcat7No ratings yet
- Energy and Sports Drinks in Children and Adolescents: Position StatementDocument5 pagesEnergy and Sports Drinks in Children and Adolescents: Position StatementDIPIN PNo ratings yet
- 262 FullDocument6 pages262 FullSenyum SehatNo ratings yet
- Are School Meals A Viable and Sustainable Tool To Improve The Healthiness and Sustainability of Children S Diet and Food Consumption A Cross NationalDocument18 pagesAre School Meals A Viable and Sustainable Tool To Improve The Healthiness and Sustainability of Children S Diet and Food Consumption A Cross NationalAndreia BorgesNo ratings yet
- Related Literature-StudiesDocument3 pagesRelated Literature-StudiesClarissa MorteNo ratings yet
- Awareness of Health Consequences of Junk Foods Among Medical StudentsDocument5 pagesAwareness of Health Consequences of Junk Foods Among Medical Studentsprincesspaypa21No ratings yet
- P EccclassificationsDocument3 pagesP EccclassificationsS AhliyaNo ratings yet
- Association of Key Foods and Beverages With Obesity in Australian SchoolchildrenDocument6 pagesAssociation of Key Foods and Beverages With Obesity in Australian SchoolchildrenLSPRO LAMPUNGNo ratings yet
- Acidic Beverages and Foods Associated With Dental ErosionDocument8 pagesAcidic Beverages and Foods Associated With Dental ErosionMariel Orozco TrellesNo ratings yet
- Chairside Diet Assessment of Caries RiskDocument6 pagesChairside Diet Assessment of Caries RiskCindyJessicaNo ratings yet
- Beverage Consumption of Filipino Childrend and Adolescents PDFDocument11 pagesBeverage Consumption of Filipino Childrend and Adolescents PDFHanor Ssecnirp NozitNo ratings yet
- Added Sugar Intake and Tooth Decay in ChildrenDocument17 pagesAdded Sugar Intake and Tooth Decay in ChildrenNicole StoicaNo ratings yet
- JINAN BANNA - Calcium Intake Among Early AdolescentsDocument13 pagesJINAN BANNA - Calcium Intake Among Early AdolescentsAzizah Sabrina 19 057No ratings yet
- Literature Review On Nutrition EducationDocument5 pagesLiterature Review On Nutrition Educationea8dfysf100% (1)
- Answer - 1 (1) (1) .EditedDocument6 pagesAnswer - 1 (1) (1) .Editedrabinelvis2030No ratings yet
- fsn310 - Research PaperDocument8 pagesfsn310 - Research Paperapi-300301211No ratings yet
- Hardy Et Al-2018-Australian and New Zealand Journal of Public HealthDocument5 pagesHardy Et Al-2018-Australian and New Zealand Journal of Public HealthAnggita RifkyNo ratings yet
- Impact of Dietary Habits Upon Nutrition-Related Factors of Secondary Schools Female Students at AL-Rusafa District in Baghdad CityDocument8 pagesImpact of Dietary Habits Upon Nutrition-Related Factors of Secondary Schools Female Students at AL-Rusafa District in Baghdad CityDoneva Lyn MedinaNo ratings yet
- Future Chefs' Beliefs On The Role of Nutrition, Diet, and Healthy Cooking Techniques in Culinary Arts Training For Foodservice A Cross-Cultural and Gender Perspective PDFDocument16 pagesFuture Chefs' Beliefs On The Role of Nutrition, Diet, and Healthy Cooking Techniques in Culinary Arts Training For Foodservice A Cross-Cultural and Gender Perspective PDFMohannad Al-OudatNo ratings yet
- The Impact of Food Branding On Children's Eating Behaviour and ObesityDocument8 pagesThe Impact of Food Branding On Children's Eating Behaviour and ObesityAlessandraBattagliaNo ratings yet
- AderemiAV FoodAdditiveDocument13 pagesAderemiAV FoodAdditivePamela Alexandra MañayNo ratings yet
- Jurnal Karies 2Document5 pagesJurnal Karies 2Suci RahmawatiNo ratings yet
- Sistema de Información Científica: Red de Revistas Científicas de América Latina, El Caribe, España y PortugalDocument7 pagesSistema de Información Científica: Red de Revistas Científicas de América Latina, El Caribe, España y PortugalSugita PattahNo ratings yet
- Competitive Food Sales in Schools and Childhood Obesity: A Longitudinal StudyDocument17 pagesCompetitive Food Sales in Schools and Childhood Obesity: A Longitudinal StudyGianpiero VincenzoNo ratings yet
- Kista Erupsi Jurnal 2Document10 pagesKista Erupsi Jurnal 2Purnama SyahbaniNo ratings yet
- Guideline On Use of Local Anesthesia For Pediatric Dental PatientsDocument7 pagesGuideline On Use of Local Anesthesia For Pediatric Dental PatientsyoelianibudisidhartaNo ratings yet
- G - BehavGuide Pedo PDFDocument13 pagesG - BehavGuide Pedo PDFcare17_08No ratings yet
- G SealantsDocument17 pagesG SealantsAngie Peterson VillamizarNo ratings yet
- Riesgo de Caries OdontopediatriaDocument8 pagesRiesgo de Caries OdontopediatriaAlexandraPortugalInfantasNo ratings yet
- Terapia Pulpar OdontopediatríaDocument9 pagesTerapia Pulpar OdontopediatríaAlexandraPortugalInfantasNo ratings yet
- Fopj 2011 - 2 PDFDocument39 pagesFopj 2011 - 2 PDFAlexandraPortugalInfantasNo ratings yet
- Magnificacion en EndodonciaDocument5 pagesMagnificacion en EndodonciaAlexandraPortugalInfantasNo ratings yet
- AAPD Policy on Use of FluorideDocument2 pagesAAPD Policy on Use of FluorideAlexandraPortugalInfantasNo ratings yet
- Alfonsina TodoDocument11 pagesAlfonsina TodoAlexandraPortugalInfantasNo ratings yet
- EE 102 Cabric Final Spring08 o Id15Document10 pagesEE 102 Cabric Final Spring08 o Id15Anonymous TbHpFLKNo ratings yet
- Giddings & Lewis Sect08 HydDocument24 pagesGiddings & Lewis Sect08 HydAngel AdautaNo ratings yet
- Design Calculations of Thrust Blocks at Lower Indira: L&T Construction Water & Effluent Treatment ICDocument3 pagesDesign Calculations of Thrust Blocks at Lower Indira: L&T Construction Water & Effluent Treatment IClagnajit dasNo ratings yet
- Pneumatic Pruning Equipment American Arborist Supplies, Tree Care, Climbing EquipmentDocument1 pagePneumatic Pruning Equipment American Arborist Supplies, Tree Care, Climbing EquipmentSalman JoNo ratings yet
- A Grammar of Anong Language Death Under Intense ContactDocument409 pagesA Grammar of Anong Language Death Under Intense ContacthaoyichuanNo ratings yet
- A Robust Firearm Identification Algorithm ProposalDocument7 pagesA Robust Firearm Identification Algorithm ProposalEuneel EscalaNo ratings yet
- Time Rates ExplainedDocument6 pagesTime Rates ExplainedAljohn Escalona100% (1)
- Comparative Study of Organic Solvents For Extraction of Copper From Ammoniacal Carbonate Solution Hu2010Document6 pagesComparative Study of Organic Solvents For Extraction of Copper From Ammoniacal Carbonate Solution Hu2010mtanaydinNo ratings yet
- 09 Exp 11 Buffer SolutionsDocument8 pages09 Exp 11 Buffer SolutionsShainmaugne AdvientoNo ratings yet
- SR. NO. Capacity/Descirption of Machine Client: A.C. Generator StatorsDocument5 pagesSR. NO. Capacity/Descirption of Machine Client: A.C. Generator Statorsmtj4uNo ratings yet
- Errata Introduction To Quantum Mechanics, David Griffiths, 2nd Ed.Document3 pagesErrata Introduction To Quantum Mechanics, David Griffiths, 2nd Ed.Marcel BezerraNo ratings yet
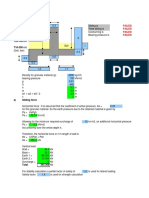
- Sliding, Overturning, Bearing Pressure and Bending Reinforcement Calculations for Retaining WallDocument4 pagesSliding, Overturning, Bearing Pressure and Bending Reinforcement Calculations for Retaining WallAbdul Aziz Julkarnain ZulkifliNo ratings yet
- Manufacturing Airbrushes Since 1904Document20 pagesManufacturing Airbrushes Since 1904Sa MiNo ratings yet
- Manual Hoist ProductsDocument40 pagesManual Hoist Productskavin bhagavathyNo ratings yet
- Textile Internship Report AlokDocument39 pagesTextile Internship Report AlokRahul TelangNo ratings yet
- Beyond Schein DentalDocument9 pagesBeyond Schein DentaltomdietzlerNo ratings yet
- XR5 9 Element 5 Band Yagi 20-17-15-12-10MDocument16 pagesXR5 9 Element 5 Band Yagi 20-17-15-12-10Msboonuy331No ratings yet
- Course Progression Map For 2021 Commencing Students: E3001 Bachelor of Engineering (Honours) Common First YearDocument21 pagesCourse Progression Map For 2021 Commencing Students: E3001 Bachelor of Engineering (Honours) Common First YearNguyễn An KhoaNo ratings yet
- Cs Project Book ManagementDocument22 pagesCs Project Book ManagementabNo ratings yet
- GLOBAL GAME AFK IN THE ZOMBIE APOCALYPSE GAME Chapter 201-250Document201 pagesGLOBAL GAME AFK IN THE ZOMBIE APOCALYPSE GAME Chapter 201-250ganesh sarikondaNo ratings yet
- Communications in Algebra: On The U-Invariant of P-Adic Function FieldsDocument9 pagesCommunications in Algebra: On The U-Invariant of P-Adic Function FieldsKarim ZahidiNo ratings yet
- S2 Papers FinalizedDocument149 pagesS2 Papers FinalizedRaffles HolmesNo ratings yet