You might also like
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtFrom EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtRating: 5 out of 5 stars5/5 (1)
- 14 Test Bank Cardiovascular Physiology MCQ Test Bank With AnswersDocument45 pages14 Test Bank Cardiovascular Physiology MCQ Test Bank With Answersmugtaba100% (4)
- MTY 1211 Chapter 1 Overview Clinical Lab HematologyDocument68 pagesMTY 1211 Chapter 1 Overview Clinical Lab Hematologychris andrieNo ratings yet
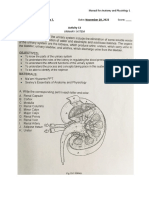
- Urinary SystemDocument5 pagesUrinary SystemJushelle Anne Tigoy Pilare100% (1)
- ATLS Practice Test 2 Answers & ExplanationsDocument8 pagesATLS Practice Test 2 Answers & ExplanationsCarl Sars50% (2)
- Robbins - 12 The HeartDocument5 pagesRobbins - 12 The HeartCM NajitoNo ratings yet
- Science Quest 8 AC 3E c04 PDFDocument94 pagesScience Quest 8 AC 3E c04 PDFmaxx100% (1)
- Cardiac TamponadeDocument18 pagesCardiac Tamponadeyelsinosmin romeroalvaradoNo ratings yet
- Recovery in TrainingDocument7 pagesRecovery in TrainingAnonymous 92hWDcNo ratings yet
- Newborn Resuscitation (Newborn CPR) BSN 12C: Madeline N. Gerzon, RN, MM Clinical Instructor Davao Doctors CollegeDocument59 pagesNewborn Resuscitation (Newborn CPR) BSN 12C: Madeline N. Gerzon, RN, MM Clinical Instructor Davao Doctors CollegemgerzonNo ratings yet
- NCM 112 Midterm ExamDocument16 pagesNCM 112 Midterm ExamYman Gio BumanglagNo ratings yet
- Mechanical VentilationDocument16 pagesMechanical VentilationBhawna JoshiNo ratings yet
- NCP CopdDocument6 pagesNCP Copdjoelette100% (1)
- Persistent Pulmonary Hypertension of The NewbornDocument4 pagesPersistent Pulmonary Hypertension of The NewbornMarwa Adly100% (1)
- BLS CPR GuideDocument27 pagesBLS CPR GuideMoh PurnomoNo ratings yet
- Acute Respiratory Distress Syndrome - Background, Pathophysiology, EtiologyDocument5 pagesAcute Respiratory Distress Syndrome - Background, Pathophysiology, EtiologyARHNo ratings yet
- 2013 CLSIFDA Table UpdateDocument5 pages2013 CLSIFDA Table UpdateGerald SweinslionNo ratings yet
- Paediatric Respiratory Reviews: F. Healy, B.D. Hanna, R. ZinmanDocument6 pagesPaediatric Respiratory Reviews: F. Healy, B.D. Hanna, R. ZinmanfadmayulianiNo ratings yet
- Tension Pneumothorax - StatPearls - NCBI BookshelfDocument9 pagesTension Pneumothorax - StatPearls - NCBI Bookshelfshinta damayantiNo ratings yet
- Go To:: Respiratory ImpairmentDocument18 pagesGo To:: Respiratory ImpairmentNanik LestariNo ratings yet
- TBL Enfermedades de La Pleura - Lectura 2Document13 pagesTBL Enfermedades de La Pleura - Lectura 2Jose LunaNo ratings yet
- handa2018Document18 pageshanda2018rocio enriquezNo ratings yet
- 28 Infective EndocarditisDocument10 pages28 Infective EndocarditisVictor PazNo ratings yet
- Stenosis Pulmonal.Document21 pagesStenosis Pulmonal.syelNo ratings yet
- Obstructive Shock, From Diagnosis To TreatmentDocument10 pagesObstructive Shock, From Diagnosis To TreatmentJonathan PuenteNo ratings yet
- Acute Pulmonary Edema - NEJMDocument4 pagesAcute Pulmonary Edema - NEJMSuzika Dewi0% (1)
- Neurogenic Pulmonary Edema - StatPearls - NCBI BookshelfDocument1 pageNeurogenic Pulmonary Edema - StatPearls - NCBI Bookshelfkud4l14rNo ratings yet
- Pulmonary Edema - StatPearls - NCBI BookshelfDocument7 pagesPulmonary Edema - StatPearls - NCBI BookshelfriyanasirNo ratings yet
- Pneumothorax, Tension and TraumaticDocument29 pagesPneumothorax, Tension and TraumaticicaNo ratings yet
- Neonatal Pericardial Effusion: Case Report and Review of The LiteratureDocument9 pagesNeonatal Pericardial Effusion: Case Report and Review of The LiteratureMarsya Yulinesia LoppiesNo ratings yet
- Emergency Department Guide to Diagnosing and Treating Pleural DiseaseDocument25 pagesEmergency Department Guide to Diagnosing and Treating Pleural DiseaseEdgardo Vargas AlvarezNo ratings yet
- Pleural Effusion in Adults—Etiology, Diagnosis, and Treatment (24.05.2019)Document10 pagesPleural Effusion in Adults—Etiology, Diagnosis, and Treatment (24.05.2019)lordiroh1No ratings yet
- PneumothotaxDocument32 pagesPneumothotaxAvishay ZoarNo ratings yet
- Cor Pulmonale An Overview 2003Document12 pagesCor Pulmonale An Overview 2003Ade Cahyo IslamiNo ratings yet
- Diagnosis and Management of Traumatic PneumothoraxDocument8 pagesDiagnosis and Management of Traumatic PneumothoraxsimcassNo ratings yet
- Acute Pulmonary EmbolismDocument13 pagesAcute Pulmonary EmbolismIrina SumeicoNo ratings yet
- (Cardiology Clinics) Ori Ben-Yehuda, Michael H. Crawford - Pulmonary Vascular Disease-Saunders (2004)Document145 pages(Cardiology Clinics) Ori Ben-Yehuda, Michael H. Crawford - Pulmonary Vascular Disease-Saunders (2004)LucasPeresBetNo ratings yet
- Pulmonary Embolism (PE) - Pulmonary Disorders - MSD Manual Professional EditionDocument25 pagesPulmonary Embolism (PE) - Pulmonary Disorders - MSD Manual Professional Editionpeterpavel112No ratings yet
- Neurogenic Pulmonary EdemaDocument7 pagesNeurogenic Pulmonary EdemajuanNo ratings yet
- Young Man With Cardiac Arrest Secondary To Undiagnosed Mediastinal MassDocument4 pagesYoung Man With Cardiac Arrest Secondary To Undiagnosed Mediastinal MassPxPPxH ChanNo ratings yet
- Dyspnoea: Pathophysiology and A Clinical Approach: ArticleDocument5 pagesDyspnoea: Pathophysiology and A Clinical Approach: ArticleadninhanafiNo ratings yet
- Chest 2002 TEP Excelente PDFDocument31 pagesChest 2002 TEP Excelente PDFEdwin AlvarezNo ratings yet
- Tetzlaff 2003Document9 pagesTetzlaff 2003Lên DươngNo ratings yet
- IJMR - Volume 3 - Issue 1 - Pages 365-370Document6 pagesIJMR - Volume 3 - Issue 1 - Pages 365-370AzaliRiccoNo ratings yet
- Management of Primary Spontaneous PneumothoraxDocument6 pagesManagement of Primary Spontaneous PneumothoraxPendragon ArthurNo ratings yet
- Congestive Heart Failure: Diagnosis, Pathophysiology, Therapy, and Implications For Respiratory CareDocument10 pagesCongestive Heart Failure: Diagnosis, Pathophysiology, Therapy, and Implications For Respiratory CareMirachel AugustNo ratings yet
- Non-Cardiogenic Pulmonary EdemaDocument7 pagesNon-Cardiogenic Pulmonary EdemadarmariantoNo ratings yet
- ABIGAIL 2010_Diffuse Alveolar HemorrhageDocument10 pagesABIGAIL 2010_Diffuse Alveolar HemorrhageRafael JustinoNo ratings yet
- CASE REPORT ON LANDAU KLEFFNER SYNDROMEDocument49 pagesCASE REPORT ON LANDAU KLEFFNER SYNDROMEMageswari SelvarajooNo ratings yet
- Sclerodactyly, and Telangiectasis) Syndrome Accompany-: Cor PulmonaleDocument2 pagesSclerodactyly, and Telangiectasis) Syndrome Accompany-: Cor PulmonaledivinaNo ratings yet
- PericarditisDocument11 pagesPericarditisrbarcellonaNo ratings yet
- Hall 2013Document6 pagesHall 2013Julio Orallo MartínezNo ratings yet
- Clinical Presentation and Diagnosis of PneumothoraxDocument49 pagesClinical Presentation and Diagnosis of PneumothoraxisahNo ratings yet
- HemodinmiaDocument8 pagesHemodinmiaPepin SalasNo ratings yet
- SaludDocument16 pagesSaluddianamera84No ratings yet
- Iadt 11 I 1 P 10Document2 pagesIadt 11 I 1 P 10anmolmani20003190No ratings yet
- 31990-PB3-7415-R3Document7 pages31990-PB3-7415-R3Rolando Miranda PeñaNo ratings yet
- PericarditisDocument11 pagesPericarditisjosefamdNo ratings yet
- Saddle Embolism in The Pulmonary Artery BifurcationDocument3 pagesSaddle Embolism in The Pulmonary Artery BifurcationAtiquzzaman RinkuNo ratings yet
- Bronchiolitis Obliterans PDFDocument7 pagesBronchiolitis Obliterans PDFSatnam KaurNo ratings yet
- Vascular Air Embolism: Symposium: Embolism in The Intensive Care UnitDocument5 pagesVascular Air Embolism: Symposium: Embolism in The Intensive Care UnitAdsoni IndoNo ratings yet
- Pulmonary Edema II: Noncardiogenic Pulmonary EdemaDocument31 pagesPulmonary Edema II: Noncardiogenic Pulmonary EdemaGita Helvia SariNo ratings yet
- Bullae, PneumothraxDocument20 pagesBullae, PneumothraxJim Albert PerlasNo ratings yet
- Pneumothorax Review: Causes, Diagnosis and ManagementDocument5 pagesPneumothorax Review: Causes, Diagnosis and ManagementAby SuryaNo ratings yet
- Modern Management of Cardiogenic Pulmonary Edema: Amal Mattu, MD, Joseph P. Martinez, MD, Brian S. Kelly, MDDocument21 pagesModern Management of Cardiogenic Pulmonary Edema: Amal Mattu, MD, Joseph P. Martinez, MD, Brian S. Kelly, MDJoni MokodoNo ratings yet
- Overview of Acute Pulmonary Embolism in AdultsDocument33 pagesOverview of Acute Pulmonary Embolism in AdultsEyla Breceda Garc�aNo ratings yet
- Pi Is 0140673696980010Document4 pagesPi Is 0140673696980010JoeNo ratings yet
- 403 Full PDFDocument10 pages403 Full PDFKuroto YoshikiNo ratings yet
- Principles of Diagnosis and Management of Traumatic PneumothoraxDocument14 pagesPrinciples of Diagnosis and Management of Traumatic PneumothoraxEkaNo ratings yet
- Causes, Effects and Treatment of Submersion InjuriesDocument9 pagesCauses, Effects and Treatment of Submersion InjuriesJ-two PallayaNo ratings yet
- Edema Pulmonar AgudaDocument4 pagesEdema Pulmonar AgudaAna Belén Artero CastañoNo ratings yet
- Superior Mediastinal Syndrome: Emergency Management: Symposium On Pgimer Management Protocols On Oncological EmergenciesDocument5 pagesSuperior Mediastinal Syndrome: Emergency Management: Symposium On Pgimer Management Protocols On Oncological EmergenciesakshayajainaNo ratings yet
- Pathophysiology: Pulmonary Embolus Hypoalbuminemia CirrhosisDocument42 pagesPathophysiology: Pulmonary Embolus Hypoalbuminemia CirrhosisLala Aya-ayNo ratings yet
- Management of Medical Records: Facts and Figures For SurgeonsDocument4 pagesManagement of Medical Records: Facts and Figures For SurgeonsGerald SweinslionNo ratings yet
- ptj4004277 PDFDocument7 pagesptj4004277 PDFChristian AriNo ratings yet
- Mayoclinproc 86 2 013 PDFDocument12 pagesMayoclinproc 86 2 013 PDFMagdy Ali ELsherbenyNo ratings yet
- Pediatric ShockDocument19 pagesPediatric ShockdarlingcarvajalduqueNo ratings yet
- Shock Pediatric in Review Yager Noviski - JournalDocument11 pagesShock Pediatric in Review Yager Noviski - JournalGerald SweinslionNo ratings yet
- Early Recognition and Management of Septic Shock in Children - JournalDocument4 pagesEarly Recognition and Management of Septic Shock in Children - JournalGerald SweinslionNo ratings yet
- Shock Pediatric in Review Yager Noviski - JournalDocument11 pagesShock Pediatric in Review Yager Noviski - JournalGerald SweinslionNo ratings yet
- Pediatric ShockDocument19 pagesPediatric ShockdarlingcarvajalduqueNo ratings yet
- The Hazard of Sharp Force Injuries Factors Influencing OutcomeDocument7 pagesThe Hazard of Sharp Force Injuries Factors Influencing OutcomeGerald SweinslionNo ratings yet
- Sepsis en PediatriaDocument8 pagesSepsis en PediatriaJorge Eduardo Espinoza RiosNo ratings yet
- Early Recognition and Management of Septic Shock in Children - JournalDocument4 pagesEarly Recognition and Management of Septic Shock in Children - JournalGerald SweinslionNo ratings yet
- Septic ShockDocument26 pagesSeptic ShockIma SoniaNo ratings yet
- Alma Saudi 2016Document28 pagesAlma Saudi 2016Gerald SweinslionNo ratings yet
- IgG IgM Pengertian Dari NigeriaDocument9 pagesIgG IgM Pengertian Dari NigeriaGerald SweinslionNo ratings yet
- Quiz #3 - ELS Human Body SystemsDocument3 pagesQuiz #3 - ELS Human Body SystemsVannie MonderoNo ratings yet
- Pharm NotesDocument113 pagesPharm NotesBibek SutradharNo ratings yet
- 2 CTN MSDocument7 pages2 CTN MSAngelie PantajoNo ratings yet
- Oral Surgery Oral Medicine Oral PathologyDocument7 pagesOral Surgery Oral Medicine Oral PathologyDiego LemurNo ratings yet
- Fernalia, Devi Listiana, Harti Monica STIKES Tri Mandiri Sakti, BengkuluDocument10 pagesFernalia, Devi Listiana, Harti Monica STIKES Tri Mandiri Sakti, BengkuluSyafi udinNo ratings yet
- Arianna Mabunga Bsn-3BDocument7 pagesArianna Mabunga Bsn-3BArianna Jasmine MabungaNo ratings yet
- ManitolDocument20 pagesManitolkr PadmanabhanNo ratings yet
- n512 Care Plan 1 3 2Document13 pagesn512 Care Plan 1 3 2api-316574434No ratings yet
- Anaerobic RespirationDocument4 pagesAnaerobic RespirationJackDaviesNo ratings yet
- Nursing Care of ThoracentesisDocument15 pagesNursing Care of ThoracentesisNora AlnaimNo ratings yet
- 2016 - Submaximal Exercise Intensity Modulates Acute Post-Exercise Heart Rate VariabilityDocument10 pages2016 - Submaximal Exercise Intensity Modulates Acute Post-Exercise Heart Rate VariabilityVeronica JanethNo ratings yet
- Cardiac DefibrillatorsDocument8 pagesCardiac Defibrillatorsصفا طلال نايفNo ratings yet
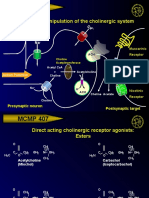
- MCMP 407: Pharmacologic Manipulation of The Cholinergic SystemDocument13 pagesMCMP 407: Pharmacologic Manipulation of The Cholinergic System16_dev5038No ratings yet
- Pathophysiology of Atrial Septal DefectDocument2 pagesPathophysiology of Atrial Septal Defectbobtaguba50% (2)
- Overview - HUMAN BLOOD CIRCULATION AND PATHWAYSDocument2 pagesOverview - HUMAN BLOOD CIRCULATION AND PATHWAYSDj22 JakeNo ratings yet
- Journal Bedah Thorax 2Document15 pagesJournal Bedah Thorax 2Novia LarasatiNo ratings yet
- Hematology: Mohamad H Qari, MD, FRCPADocument49 pagesHematology: Mohamad H Qari, MD, FRCPASantoz ArieNo ratings yet
- Animaltissues 180604115637Document40 pagesAnimaltissues 180604115637proud.student2023No ratings yet