You might also like
- Pulpectomy ProceduresDocument3 pagesPulpectomy ProceduresITS DENTAL COLLEGE Greater NoidaNo ratings yet
- Bonded Lingual Retainer Fit for 17yo Male with Clear Medical HistoryDocument3 pagesBonded Lingual Retainer Fit for 17yo Male with Clear Medical Historymaddie g.No ratings yet
- RCT FinalDocument13 pagesRCT FinalDaniela NoreñaNo ratings yet
- Oral Health Instructions - During Treatment 1Document3 pagesOral Health Instructions - During Treatment 1maddie g.No ratings yet
- UNIT4 Endodontics - Best PPDocument37 pagesUNIT4 Endodontics - Best PPAnna PruteanuNo ratings yet
- City & Guilds Level 3 Extended Diploma Indental Nursing (4238-12)Document112 pagesCity & Guilds Level 3 Extended Diploma Indental Nursing (4238-12)yesja1No ratings yet
- S3 Funct App Bite Reg2Document3 pagesS3 Funct App Bite Reg2maddie g.No ratings yet
- S1 Fixed App DEBONDING 2Document3 pagesS1 Fixed App DEBONDING 2maddie g.No ratings yet
- S2 Remov Apps Adjustment 1Document3 pagesS2 Remov Apps Adjustment 1maddie g.0% (1)
- S1 Fixed App BANDING 3Document3 pagesS1 Fixed App BANDING 3maddie g.No ratings yet
- Fitting of upper removable appliance with bilateral expansion screwsDocument3 pagesFitting of upper removable appliance with bilateral expansion screwsmaddie g.No ratings yet
- Adjustment of Frankel regulator in 10y male patientDocument3 pagesAdjustment of Frankel regulator in 10y male patientmaddie g.No ratings yet
- Bleeding After Tooth ExtractionDocument3 pagesBleeding After Tooth ExtractionwahyurianjaniNo ratings yet
- Dental Pain Control MethodsDocument32 pagesDental Pain Control MethodsAnna PruteanuNo ratings yet
- Functional App Fit3Document3 pagesFunctional App Fit3maddie g.No ratings yet
- DiplomaCourseHandbook 000Document86 pagesDiplomaCourseHandbook 000Mostafa FayadNo ratings yet
- Endodontic Clinic Manual-1Document32 pagesEndodontic Clinic Manual-1marko makramNo ratings yet
- The Bite Stage. The Try-In Stage. The Fitting StageDocument4 pagesThe Bite Stage. The Try-In Stage. The Fitting StageStanislavNemtanuNo ratings yet
- Questions and Answers for Diploma in Dental Nursing, Level 3From EverandQuestions and Answers for Diploma in Dental Nursing, Level 3No ratings yet
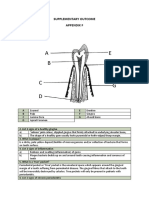
- Supplementary Outcome Appendix RDocument2 pagesSupplementary Outcome Appendix Rburcu ersahinNo ratings yet
- Infection Control in Dentistry FinalDocument12 pagesInfection Control in Dentistry FinalDevAshish BNo ratings yet
- Try-in Procedure GuideDocument8 pagesTry-in Procedure GuideVikas AggarwalNo ratings yet
- Dental Risk AssessmentDocument13 pagesDental Risk AssessmentCamila Walton100% (1)
- Patient CareDocument3 pagesPatient CareAistė AgapovaitėNo ratings yet
- Infectious Control Measures (Dental Clinic)Document7 pagesInfectious Control Measures (Dental Clinic)Susan JilhanoNo ratings yet
- Tooth preparation technique for studentsDocument6 pagesTooth preparation technique for studentsadindayokopNo ratings yet
- Myanmar Dental Journal - Vol. 22, No. 1, January 2015Document60 pagesMyanmar Dental Journal - Vol. 22, No. 1, January 2015Nugraha AnggaNo ratings yet
- Extra Oral RadiographyDocument17 pagesExtra Oral RadiographyAl RawdhaNo ratings yet
- Endo & RestorativeDocument59 pagesEndo & RestorativeLoredana RaduNo ratings yet
- Photograph Protocol: A Guide For Clinical StaffDocument22 pagesPhotograph Protocol: A Guide For Clinical Staffmaddie g.No ratings yet
- Full Crown Module 2786Document16 pagesFull Crown Module 2786Mustafa S. KoperlyNo ratings yet
- Essential Examination Aid For Dental NursesFrom EverandEssential Examination Aid For Dental NursesRating: 3.5 out of 5 stars3.5/5 (3)
- RadiographsDocument28 pagesRadiographs10atmNo ratings yet
- Try in Step in Complete DentureDocument8 pagesTry in Step in Complete DentureMuhammad SdiqNo ratings yet
- Supplementary Outcome Appendix GDocument3 pagesSupplementary Outcome Appendix Gburcu ersahinNo ratings yet
- Elastomeric Impression MaterialsDocument89 pagesElastomeric Impression MaterialsDr Anand RajapurNo ratings yet
- G 110 Complaints, Problems and Events Overview Ver 12Document12 pagesG 110 Complaints, Problems and Events Overview Ver 12Qurat-Ul-Ain tariqNo ratings yet
- Pulpotomy and Pulpectomy in Children: Pulpotomy For Primary TeethDocument10 pagesPulpotomy and Pulpectomy in Children: Pulpotomy For Primary TeethVinayak SinghNo ratings yet
- Finishing Lines:: Requirements of Finishing LineDocument13 pagesFinishing Lines:: Requirements of Finishing LineVikas BhattNo ratings yet
- PulpectomyDocument3 pagesPulpectomyWafa Nabilah Kamal100% (1)
- Supplementary Outcome Appendix LDocument2 pagesSupplementary Outcome Appendix Lburcu ersahinNo ratings yet
- Dental Impression Materials GuideDocument25 pagesDental Impression Materials Guidescort cherNo ratings yet
- Dental Infection Control PrecautionsDocument5 pagesDental Infection Control PrecautionsdrdarshakNo ratings yet
- Mock Exam 11Document11 pagesMock Exam 11Abhay Khanna100% (2)
- HND Dental Nurse AssignmentDocument18 pagesHND Dental Nurse Assignmentandreeal8950% (8)
- Dental Nursing Health and SafetyDocument7 pagesDental Nursing Health and SafetyPierina Lucia Mushka Cirigliano-Able100% (2)
- S5 Assist With Imps and Bite FUNCTIONAL APP IMPS 1Document3 pagesS5 Assist With Imps and Bite FUNCTIONAL APP IMPS 1maddie g.No ratings yet
- Supplementary Outcome Appendix JDocument2 pagesSupplementary Outcome Appendix Jburcu ersahinNo ratings yet
- Supplementary Outcome Appendix FDocument2 pagesSupplementary Outcome Appendix Fburcu ersahinNo ratings yet
- Supplementary Outcome Appendix TDocument2 pagesSupplementary Outcome Appendix Tburcu ersahinNo ratings yet
- Elastomeric Impression MaterialsDocument121 pagesElastomeric Impression Materialskashyap sawantNo ratings yet
- ROE Session UNIT 4Document22 pagesROE Session UNIT 4Amina Abdullahi0% (1)
- Bite Registration Methods for Dental Cast ArticulationDocument5 pagesBite Registration Methods for Dental Cast ArticulationDr-Mohamed TharwatNo ratings yet
- Roe All 5 Units PDFDocument60 pagesRoe All 5 Units PDFVaibhav Singh100% (1)
- Color Atlas of EndoDocument203 pagesColor Atlas of Endooana_en100% (23)
- Fixed Prosthetics WorkbookDocument23 pagesFixed Prosthetics WorkbookEliza EllieNo ratings yet
- Inaly and Onlay: For Single Tooth Restoration Onlay: All Cusp Inlay: All CuspDocument20 pagesInaly and Onlay: For Single Tooth Restoration Onlay: All Cusp Inlay: All CuspLesta Yang100% (7)
- Oral Anatomy & Physiology TestDocument34 pagesOral Anatomy & Physiology TestEliza EllieNo ratings yet
- Infection Control in Dental PracticeDocument28 pagesInfection Control in Dental PracticeAntony Sebastian75% (4)
- Interpretation of OpgDocument6 pagesInterpretation of Opgjawaad29375% (8)
- Eur JEsthet Dent 2013 MeyenbergDocument97 pagesEur JEsthet Dent 2013 Meyenbergsoma kiranNo ratings yet
- Rehabilitation of Maxillary Anterior Teeth with Richmond CrownDocument4 pagesRehabilitation of Maxillary Anterior Teeth with Richmond CrownRaghav PratapNo ratings yet
- UConn Dental: Prosthodontics Clinic Manual 11-12Document67 pagesUConn Dental: Prosthodontics Clinic Manual 11-12lippincott2011No ratings yet
- 6.clinical Case ReportMultidisciplinary Approach For Rehabilitation of Debilitated Anterior ToothDocument6 pages6.clinical Case ReportMultidisciplinary Approach For Rehabilitation of Debilitated Anterior ToothSahana RangarajanNo ratings yet
- Rosen 1961Document14 pagesRosen 1961Fer TorresNo ratings yet
- Endo SCHC EaxamDocument30 pagesEndo SCHC EaxamKiran Gowda80% (10)
- Conventional Tic Failure and Re TreatmentDocument25 pagesConventional Tic Failure and Re TreatmentBruno Miguel Teixeira QueridinhaNo ratings yet
- Restoration of The Endodontically Treated Tooth: J. William Robbins, DDS, MADocument18 pagesRestoration of The Endodontically Treated Tooth: J. William Robbins, DDS, MAboskiguptaNo ratings yet
- Gutmann 1992Document10 pagesGutmann 1992Asik AliNo ratings yet
- Direct Fiber-reinforced Composite Reconstruction of a Severely Damaged ToothDocument7 pagesDirect Fiber-reinforced Composite Reconstruction of a Severely Damaged ToothAngga RanggaNo ratings yet
- Restoration of Endodontically Treated Teeth: Answers To Important QuestionsDocument57 pagesRestoration of Endodontically Treated Teeth: Answers To Important QuestionsGermanLoopezzNo ratings yet
- Richmondcrown PDFDocument7 pagesRichmondcrown PDFAthulya PallipurathNo ratings yet
- Maciej Zarow Metal Post and Core How To Improve Aesthetics Via WWW Styleitaliano OrgDocument27 pagesMaciej Zarow Metal Post and Core How To Improve Aesthetics Via WWW Styleitaliano OrgghfhfdghNo ratings yet
- MCQ Review For Saudi Licensing Exam (SLE)Document0 pagesMCQ Review For Saudi Licensing Exam (SLE)Rakesh Kumar83% (6)
- Indication To The Type of RestorationDocument61 pagesIndication To The Type of RestorationDr.O.R.GANESAMURTHINo ratings yet
- LibmanDocument8 pagesLibmanManjeev GuragainNo ratings yet
- Maryland Bridge: An Interim Prosthesis For Tooth Replacement in AdolescentsDocument4 pagesMaryland Bridge: An Interim Prosthesis For Tooth Replacement in AdolescentsHien TruongNo ratings yet
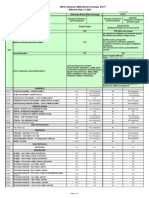
- MCS Classicare (MA) Dental Coverage SummaryDocument4 pagesMCS Classicare (MA) Dental Coverage SummaryJessicaNo ratings yet
- Multi-Piece Post-Crown For Multi-Rooted Teeth With Non-Parallel CanalsDocument4 pagesMulti-Piece Post-Crown For Multi-Rooted Teeth With Non-Parallel CanalsGiannis DimitriouNo ratings yet
- Modern Endodontic Principles Part 7 The Restorative InterfaceDocument12 pagesModern Endodontic Principles Part 7 The Restorative InterfacedoctorlupuNo ratings yet
- NY Medicaid Dental CodesDocument32 pagesNY Medicaid Dental CodesWil HectorNo ratings yet
- Load Fatigue of Teeth Restored With Cast Posts and Crowns Affected by Ferrule LengthDocument8 pagesLoad Fatigue of Teeth Restored With Cast Posts and Crowns Affected by Ferrule LengthEddy Mazariegos100% (1)
- POST-CORE HISTORY AND TECHNIQUESDocument8 pagesPOST-CORE HISTORY AND TECHNIQUESGolda MardikaNo ratings yet
- Prefabricated Logam Antara Bahan Core Build Up Modifikasi Logam Glass Ionomer Dan Core Build Up ResinDocument12 pagesPrefabricated Logam Antara Bahan Core Build Up Modifikasi Logam Glass Ionomer Dan Core Build Up ResinghinaNo ratings yet
- 023 Morgano Clasico PDFDocument15 pages023 Morgano Clasico PDFLaura Sandoval AcevedoNo ratings yet
- Restorative Dentistry Logbook RequirementsDocument21 pagesRestorative Dentistry Logbook RequirementsIrfan AhmedNo ratings yet
- Fracture Strength of Endodontically Treated Maxillary Premolars Supported by A Horizontal Glass Fiber Post: An in Vitro StudyDocument6 pagesFracture Strength of Endodontically Treated Maxillary Premolars Supported by A Horizontal Glass Fiber Post: An in Vitro StudyPaulo CastroNo ratings yet
- HAAD EXAM 24/01/2018 KEY POINTSDocument21 pagesHAAD EXAM 24/01/2018 KEY POINTSmuneer024No ratings yet
- 05 Goodacre 1994 Review Part 1Document8 pages05 Goodacre 1994 Review Part 1Ana Massiel NarváezNo ratings yet
- Removable Partial Denture ComponentsDocument128 pagesRemovable Partial Denture ComponentsVikas Aggarwal50% (2)