You might also like
- Relationships Mark MansonDocument31 pagesRelationships Mark MansonBao NgocNo ratings yet
- Candle MagicDocument38 pagesCandle MagicKathy Brannon Green75% (4)
- SketchyMicro ChartDocument14 pagesSketchyMicro ChartSonia100% (8)
- Archer III Pilots Training Handbook AV8Document344 pagesArcher III Pilots Training Handbook AV8James D ShankNo ratings yet
- Flash Notes SyndromesDocument8 pagesFlash Notes SyndromesschxzerrydawnNo ratings yet
- Activity 6 - Drug StudyDocument14 pagesActivity 6 - Drug StudyAl-Mujib TanogNo ratings yet
- Backup of ANTIMICROBIALS PRINTABLEDocument4 pagesBackup of ANTIMICROBIALS PRINTABLEinvading_jam7582100% (1)
- Sizing A Generator For Electric Motor LoadsDocument2 pagesSizing A Generator For Electric Motor LoadsMind of BeautyNo ratings yet
- AMC MCQ Dermatology NotesDocument25 pagesAMC MCQ Dermatology NotesJenny FuNo ratings yet
- Drug StudyDocument30 pagesDrug StudyClaire MachicaNo ratings yet
- Serpent 1Document19 pagesSerpent 1BurdetOnitaNo ratings yet
- Captains Posts With Attachments 1 PDFDocument211 pagesCaptains Posts With Attachments 1 PDFMushfiq FaysalNo ratings yet
- Part1 WHOStandardAccupuncturePointLocationsDocument39 pagesPart1 WHOStandardAccupuncturePointLocationsJiman Ryu100% (1)
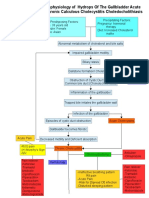
- Pathophysiology of CholecystitisDocument2 pagesPathophysiology of CholecystitisAnonymous gDp7y3Cl82% (22)
- Hematology Oncology - LymphomaDocument1 pageHematology Oncology - LymphomaEugen MNo ratings yet
- Republic of The Philippines Puerto Princesa City: Palawan State UniversityDocument2 pagesRepublic of The Philippines Puerto Princesa City: Palawan State UniversityRosemarie EustaquioNo ratings yet
- HeparinDocument2 pagesHeparinMagdayao Romamea100% (1)
- Pediatrics DR Anand BhatiaDocument54 pagesPediatrics DR Anand BhatianadeemhumdardNo ratings yet
- CeftriaxoneDocument3 pagesCeftriaxonejiloNo ratings yet
- Top Ten Family Practice DiagosesDocument6 pagesTop Ten Family Practice DiagosesKatrina HumphreyNo ratings yet
- Brand Name Generic Name Dosage Action Indication Contra-Indication Precautions Nursing ConsiderationDocument6 pagesBrand Name Generic Name Dosage Action Indication Contra-Indication Precautions Nursing ConsiderationDrexcy Jhoy San AntonioNo ratings yet
- Final Exam-1st Trial (2020-2021) : Choose The Most Appropriate Single AswerDocument2 pagesFinal Exam-1st Trial (2020-2021) : Choose The Most Appropriate Single Aswerhayfaa AhmedNo ratings yet
- Approach To Neonatal JaundiceDocument5 pagesApproach To Neonatal JaundiceMaryam BajNo ratings yet
- Day2 Communicable Disease ReviewerDocument19 pagesDay2 Communicable Disease ReviewerLrac KangNo ratings yet
- URO 3 - Neoplasm in The Genitourinary TractDocument8 pagesURO 3 - Neoplasm in The Genitourinary TractHa Jae kyeongNo ratings yet
- Disease Symptoms/Signs Labs/ Workup Treatment NotesDocument4 pagesDisease Symptoms/Signs Labs/ Workup Treatment NotesYingying RezmovitsNo ratings yet
- Molluscum Contagiosum by P.jagadeeshDocument2 pagesMolluscum Contagiosum by P.jagadeeshJagadeesh YadavNo ratings yet
- Drugs For Coagulation Disorders: Coagulant DrugDocument6 pagesDrugs For Coagulation Disorders: Coagulant DrugApple MaeNo ratings yet
- CD B Fluids and Sputum Dr. Buenverida Kate FaustoDocument6 pagesCD B Fluids and Sputum Dr. Buenverida Kate FaustoKaren GumabonNo ratings yet
- Drug Study BevacizumabDocument1 pageDrug Study BevacizumabBARRISTERFLOWERSEAURCHIN6No ratings yet
- Drug Gordons PeDocument6 pagesDrug Gordons PeNicko Pazon AranasNo ratings yet
- Central Session FungalDocument17 pagesCentral Session Fungaldocjeevan89No ratings yet
- Drugstudy EamcDocument5 pagesDrugstudy EamckillthealarmistNo ratings yet
- Drug StudyDocument3 pagesDrug StudyalysNo ratings yet
- CP Drug StudyDocument8 pagesCP Drug StudyXerczhiel Faye RioNo ratings yet
- Amoxicillin, Ferrous SulfateDocument2 pagesAmoxicillin, Ferrous SulfateAngelyn BucasoNo ratings yet
- MB Yeasts PassDocument1 pageMB Yeasts PassJulia IshakNo ratings yet
- Medications That Can Cause Peripheral NeuropathyDocument1 pageMedications That Can Cause Peripheral NeuropathySaljavNo ratings yet
- Antivirals: Drug Clinical Use Drug Type Action Side Effect Drug Interaction Pharmacokinetic S Other DetailsDocument10 pagesAntivirals: Drug Clinical Use Drug Type Action Side Effect Drug Interaction Pharmacokinetic S Other DetailshectorNo ratings yet
- Pathophysiology of Transitional Cell CarcinomaDocument10 pagesPathophysiology of Transitional Cell CarcinomaJheanAlphonsineT.MeansNo ratings yet
- Hematology 2 ReviewerDocument4 pagesHematology 2 ReviewerAnn YeongNo ratings yet
- Notes: Non-Urothelial Bladder CancersDocument5 pagesNotes: Non-Urothelial Bladder CancersTrivedi NisargNo ratings yet
- 4上cs 第一次心智圖Document1 page4上cs 第一次心智圖Eric LinNo ratings yet
- Name of Drug Generic (Brand) Classification Dose/ Frequency/ Route Mechanism of Action Indication Contraindication Side Effects Nursing PrecautionDocument1 pageName of Drug Generic (Brand) Classification Dose/ Frequency/ Route Mechanism of Action Indication Contraindication Side Effects Nursing PrecautionJulia Shane Barrios100% (1)
- Glomerular Disease and DiureticsDocument26 pagesGlomerular Disease and DiureticsDapot SianiparNo ratings yet
- NeisseriaDocument28 pagesNeisseriaZeth MoturiNo ratings yet
- Sinusitis Complications - DR - AnupDocument33 pagesSinusitis Complications - DR - AnupDr. Janarthanan VNo ratings yet
- Fluid:serum Protein Fluid: Serum LDDocument3 pagesFluid:serum Protein Fluid: Serum LDFiverNo ratings yet
- Anti Thrombotic Drugs and Transfusion MedicineDocument5 pagesAnti Thrombotic Drugs and Transfusion MedicineIS99057No ratings yet
- UC & Crohn's DiseaseDocument3 pagesUC & Crohn's DiseaseYalin AbouhassiraNo ratings yet
- BangkasDocument5 pagesBangkasJulianne BangkasNo ratings yet
- Drug Study. GeamhDocument5 pagesDrug Study. GeamhMacky RobentaNo ratings yet
- Microbiology - ParasitologyDocument14 pagesMicrobiology - Parasitologytdci.franceskorineganzaNo ratings yet
- DR Anna Mira Lubis - Diagnostic Approach of ThrombocytopeniaDocument36 pagesDR Anna Mira Lubis - Diagnostic Approach of Thrombocytopeniayosua simarmataNo ratings yet
- Pathophysiology On Cellulitis On Left Facial AreaDocument9 pagesPathophysiology On Cellulitis On Left Facial AreaAdiNo ratings yet
- Rheumatologic Renal Disease: SLE vs. SclerodermaDocument2 pagesRheumatologic Renal Disease: SLE vs. SclerodermaKenNo ratings yet
- Adults and Pediatric Patients Weighing More Than 40kg InterventionsDocument11 pagesAdults and Pediatric Patients Weighing More Than 40kg Interventionschinchin ramosNo ratings yet
- Measles (Rubeola/Morbilli) : Pre-EruptiveDocument28 pagesMeasles (Rubeola/Morbilli) : Pre-EruptiveErjen Alexandria SiaNo ratings yet
- Drug StudyDocument7 pagesDrug StudyJoseph Angelo Fortuna CarmonaNo ratings yet
- Algoritmo Fiebre de Origen DesconocidoDocument1 pageAlgoritmo Fiebre de Origen Desconocidoluisa gonzálezNo ratings yet
- Snake BiteDocument29 pagesSnake BiteOby BedahNo ratings yet
- Drugstudy 2Document5 pagesDrugstudy 2Westley RubinoNo ratings yet
- Module 6.4 ParasitesDocument6 pagesModule 6.4 ParasitesPNo ratings yet
- Ceftriaxone Drug Study 1-BurnDocument2 pagesCeftriaxone Drug Study 1-BurnLalaine BautistaNo ratings yet
- AMPICILLINDocument4 pagesAMPICILLINKate ArañezNo ratings yet
- Untitled DocumentDocument2 pagesUntitled DocumentRosemarie EustaquioNo ratings yet
- Rheumatology - Approach To Joint PainDocument1 pageRheumatology - Approach To Joint PainJasmine KangNo ratings yet
- Rheumatology - Other Connective TissueDocument1 pageRheumatology - Other Connective TissueJasmine Kang100% (2)
- Pediatrics - Neonatal Jaundice PDFDocument2 pagesPediatrics - Neonatal Jaundice PDFJasmine KangNo ratings yet
- Pediatrics - Neonatal ICUDocument2 pagesPediatrics - Neonatal ICUJasmine KangNo ratings yet
- Pediatrics - OrthopedicsDocument2 pagesPediatrics - OrthopedicsJasmine KangNo ratings yet
- Pediatrics - Failure To Pass Meconium PDFDocument2 pagesPediatrics - Failure To Pass Meconium PDFJasmine KangNo ratings yet
- Pediatrics - ImmunodeficiencyDocument3 pagesPediatrics - ImmunodeficiencyJasmine KangNo ratings yet
- Pediatrics - Lower AirwayDocument3 pagesPediatrics - Lower AirwayJasmine KangNo ratings yet
- Quiz Answers Quiz2A KeyDocument3 pagesQuiz Answers Quiz2A KeyJasmine KangNo ratings yet
- Quiz Answers Quiz2B KeyDocument3 pagesQuiz Answers Quiz2B KeyJasmine KangNo ratings yet
- Presentation1 VDocument17 pagesPresentation1 VVikram.SNo ratings yet
- Final Exam Psychology G11Document4 pagesFinal Exam Psychology G11Meetali ArchitNo ratings yet
- Fermenting Yogurt at Home: Brian A. Nummer, Ph.D. National Center For Home Food Preservation October 2002Document6 pagesFermenting Yogurt at Home: Brian A. Nummer, Ph.D. National Center For Home Food Preservation October 2002MohsinNo ratings yet
- Introduction To Masonry StructuresDocument33 pagesIntroduction To Masonry StructuresNiraj JhaNo ratings yet
- DC TrainingDocument5 pagesDC TrainingVishal PanchaalNo ratings yet
- Dokumen - Tips - Syntax Tree Diagram in Japanese Tree Diagram in Japanese From Deep StructureDocument94 pagesDokumen - Tips - Syntax Tree Diagram in Japanese Tree Diagram in Japanese From Deep StructureAdisaka M HendiyantoNo ratings yet
- Chapter-1 EMDDocument62 pagesChapter-1 EMDParv ChoudharyNo ratings yet
- Chief Operating Officer VP in San Diego CA Resume Mitchell WhiteDocument4 pagesChief Operating Officer VP in San Diego CA Resume Mitchell WhiteMitchellWhiteNo ratings yet
- Civil Suit Against Establishment of Slaughter House at Pali in Faridabad Withot Approval of State Committee - Abhishek KadyanDocument29 pagesCivil Suit Against Establishment of Slaughter House at Pali in Faridabad Withot Approval of State Committee - Abhishek KadyanNaresh KadyanNo ratings yet
- Analysis of The Steel Joint With Four Bolts in The RowDocument8 pagesAnalysis of The Steel Joint With Four Bolts in The RowMahmoud El-KatebNo ratings yet
- Lifting Guidance For DN 2000 DN 2200 and DN 2400 Pipes PD38Document4 pagesLifting Guidance For DN 2000 DN 2200 and DN 2400 Pipes PD38sosi2020No ratings yet
- ERGNOMICSOFTRACTORvol 16 No 1Document112 pagesERGNOMICSOFTRACTORvol 16 No 1Yosun KarasuNo ratings yet
- Sleep-Disordered Breathing in Children: Practice GapsDocument13 pagesSleep-Disordered Breathing in Children: Practice GapsSofía Contreras SalazarNo ratings yet
- Periodic Table WorksheetDocument23 pagesPeriodic Table Worksheetlakshmi ghayathri N.M.No ratings yet
- E-Cigarette Aerosol Analysis ReportDocument6 pagesE-Cigarette Aerosol Analysis ReportUman KinapNo ratings yet
- Lance Design For Argon Bubbling in Molten MetalDocument12 pagesLance Design For Argon Bubbling in Molten MetalJOAN REYES MIRANDANo ratings yet
- Biosynthesis and Characterization of Copper Nanoparticles From TulsiDocument10 pagesBiosynthesis and Characterization of Copper Nanoparticles From TulsiRabeea NasirNo ratings yet
- Time TableDocument1 pageTime TableAbhishek ChandraNo ratings yet
- Discriminant Correspondence AnDocument10 pagesDiscriminant Correspondence AnalbgomezNo ratings yet
- Catalogo ShantuiDocument8 pagesCatalogo Shantuicefuneslpez100% (3)
- Edan I15 Blood Gas and Chemistry Analysis System Service ManualDocument104 pagesEdan I15 Blood Gas and Chemistry Analysis System Service ManualAIINo ratings yet
- ST 1 - Tle 6 - Q1Document2 pagesST 1 - Tle 6 - Q1RhoseNo ratings yet
- L 0207061 CRAFTSMAN ManualDocument65 pagesL 0207061 CRAFTSMAN Manualapplecakes2100% (1)