You might also like
- Anticoagulation TherapyFrom EverandAnticoagulation TherapyJoe F. LauNo ratings yet
- Heparin drug monograph provides dosing, indications, and nursing considerationsDocument4 pagesHeparin drug monograph provides dosing, indications, and nursing considerationsTri Purma SariNo ratings yet
- Endocrinology Notes for Medical StudentsFrom EverandEndocrinology Notes for Medical StudentsRating: 4 out of 5 stars4/5 (1)
- Drug StudyDocument11 pagesDrug StudynessaNo ratings yet
- Complete Drug StudyDocument21 pagesComplete Drug StudyBea Dela CenaNo ratings yet
- PHINMA Nursing Drug StudyDocument2 pagesPHINMA Nursing Drug StudyArianne NicoleNo ratings yet
- Anti-Coagulant (Vte in Obstetrics) - Madam LiewDocument10 pagesAnti-Coagulant (Vte in Obstetrics) - Madam LiewNana YunusNo ratings yet
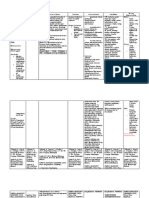
- Brand Name Generic Name Dosage Action Indication Contra-Indication Precautions Nursing ConsiderationDocument6 pagesBrand Name Generic Name Dosage Action Indication Contra-Indication Precautions Nursing ConsiderationDrexcy Jhoy San AntonioNo ratings yet
- Clopidogrel Mechanism of Action and Nursing ResponsibilitiesDocument13 pagesClopidogrel Mechanism of Action and Nursing ResponsibilitiesJimuel Brian ManelaNo ratings yet
- EnoxaparineDocument1 pageEnoxaparinePatricia MaglasangNo ratings yet
- Drug Name Dopamine Indications Contraindications Mechanism of Action Common Side-Effects Nursing ConsiderationsDocument4 pagesDrug Name Dopamine Indications Contraindications Mechanism of Action Common Side-Effects Nursing ConsiderationsPRINCESS LARA CASILAONo ratings yet
- Nursing responsibilities for CotrimoxazoleDocument5 pagesNursing responsibilities for CotrimoxazoleGwyn RosalesNo ratings yet
- Drug Study (Pe)Document15 pagesDrug Study (Pe)Jobelle AcenaNo ratings yet
- Drug Indication, Mode of Action, Dosage, Adverse Effects, and Nursing Responsibilities for HeparinDocument2 pagesDrug Indication, Mode of Action, Dosage, Adverse Effects, and Nursing Responsibilities for HeparinMagdayao Romamea100% (1)
- Tranexamic Acid Drug StudyDocument1 pageTranexamic Acid Drug StudyEsmareldah Henry Sirue100% (1)
- Clopidogrel Bisulfate (PLOGREL)Document2 pagesClopidogrel Bisulfate (PLOGREL)Kristine Young0% (1)
- Nursing responsibilities for mefenamic acidDocument4 pagesNursing responsibilities for mefenamic acidStephen VillegasNo ratings yet
- Drug StudyDocument1 pageDrug StudySherrie Ann Delos SantosNo ratings yet
- Drug Study2Document3 pagesDrug Study2Anjulie Austria SoNo ratings yet
- Name of Drug Mechanism of Action Indication Contraindication Adverse Effect Nursing Responsibility Generic Name: Brand Name: Classification: CnsDocument4 pagesName of Drug Mechanism of Action Indication Contraindication Adverse Effect Nursing Responsibility Generic Name: Brand Name: Classification: CnsRoxy TofyNo ratings yet
- Drug StudyDocument6 pagesDrug StudychaNo ratings yet
- Anticoagulant, Antithrombotic and Anti-Platelet DrugsDocument63 pagesAnticoagulant, Antithrombotic and Anti-Platelet Drugsruchipickle100% (1)
- Drug Study 2Document3 pagesDrug Study 2Roland YusteNo ratings yet
- Pharmacology II: Treatments for Blood Disorders and InflammationDocument61 pagesPharmacology II: Treatments for Blood Disorders and InflammationDiane BanuaNo ratings yet
- Reteplase (MIRel)Document23 pagesReteplase (MIRel)Jhoann JamanilaNo ratings yet
- Antifungal Agents: EchinocandinsDocument2 pagesAntifungal Agents: EchinocandinsCourtney TownsendNo ratings yet
- Nursing care for hydralazine administrationDocument27 pagesNursing care for hydralazine administrationChan SorianoNo ratings yet
- Drug StudyDocument4 pagesDrug StudyRochelle TenederoNo ratings yet
- Drug Name Mechanism of Action Indication/ Contraindication Adverse Effect Nursing ResponsibilitiesDocument1 pageDrug Name Mechanism of Action Indication/ Contraindication Adverse Effect Nursing ResponsibilitiesJohnrick VenturaNo ratings yet
- Lovenox (Enoxaparin)Document1 pageLovenox (Enoxaparin)E100% (5)
- Micromonospora Purpurea. Action IsDocument3 pagesMicromonospora Purpurea. Action IsCarlos H. AcuñaNo ratings yet
- Gentamycin Drug StudyDocument2 pagesGentamycin Drug StudyShin Guevara100% (3)
- Tranexamic Acid: Generic NameDocument3 pagesTranexamic Acid: Generic NameDivine Grace Arreglo AbingNo ratings yet
- Furosemide Drug Study CompressDocument1 pageFurosemide Drug Study CompressAngelica TolledoNo ratings yet
- Tranexamic Acid Drug StudyDocument1 pageTranexamic Acid Drug StudyCen Janber Cabrillos67% (3)
- A Drug Study On: HeparinDocument8 pagesA Drug Study On: HeparinRaijenne VersolaNo ratings yet
- CoA Dis - RevDocument60 pagesCoA Dis - RevAzra Al AmanahNo ratings yet
- Enoxaparin Drug StudyDocument2 pagesEnoxaparin Drug StudyRohannah D. MalawadNo ratings yet
- Drug Study (Fluimicil, Atorvastatin, Piperacillin + Tazobactam..etc.)Document3 pagesDrug Study (Fluimicil, Atorvastatin, Piperacillin + Tazobactam..etc.)Kate PedzNo ratings yet
- Drug-Study NCPDocument5 pagesDrug-Study NCPMURILLO, FRANK JOMARI C.No ratings yet
- Drug Study TableDocument14 pagesDrug Study TableAl-Mujib TanogNo ratings yet
- Drug Study - Tobramycin & CelebrexDocument3 pagesDrug Study - Tobramycin & CelebrexjbespirituNo ratings yet
- Anticoagulation RegimensDocument1 pageAnticoagulation RegimensLame BossNo ratings yet
- Pharmacology Affecting CoagulationDocument19 pagesPharmacology Affecting CoagulationCurtney PedriaNo ratings yet
- Pharm Final Exam NotesDocument26 pagesPharm Final Exam Noteskatiana louis100% (1)
- Epo DrugstudyDocument3 pagesEpo DrugstudyKhatlen BagaresNo ratings yet
- RUG Tudy: College of NursingDocument3 pagesRUG Tudy: College of NursingYoko Mae YanoNo ratings yet
- Anti - Infectives AgentsDocument83 pagesAnti - Infectives AgentsRhien Yrah P. CabalongaNo ratings yet
- UROKINASE (Kinlytic)Document4 pagesUROKINASE (Kinlytic)Mikaela Gabrielle GeraliNo ratings yet
- Discharge PlanDocument14 pagesDischarge PlanAsniah Hadjiadatu AbdullahNo ratings yet
- Chapter 3 Hospital Pharmacy Notes Complete Notes by Noteskarts Acc To ER20Document25 pagesChapter 3 Hospital Pharmacy Notes Complete Notes by Noteskarts Acc To ER20Shamant TNo ratings yet
- Supply Chain and Inventory ControlDocument11 pagesSupply Chain and Inventory Controlharshit1509dNo ratings yet
- 7-Lipid DisorderDocument6 pages7-Lipid DisorderApple MaeNo ratings yet
- Chew, swallow or crush mebendazole tabletsDocument6 pagesChew, swallow or crush mebendazole tabletsDenvicNo ratings yet
- Cefixime and Azithromycin Drug GuideDocument3 pagesCefixime and Azithromycin Drug GuideArianne Joy SalvadorNo ratings yet
- MW2 DRUG STUDYDocument2 pagesMW2 DRUG STUDYc.cagas.529054No ratings yet
- Drug Analysis and NCP Ob Ward PoldoDocument9 pagesDrug Analysis and NCP Ob Ward PoldosatruetalagaNo ratings yet
- Drug StudyDocument4 pagesDrug StudyAda Eloisa AloveraNo ratings yet
- Chapter 37Document46 pagesChapter 37HannaNo ratings yet
- DRUG STUDY OrthoDocument6 pagesDRUG STUDY OrthoRalph Elvin MacanlalayNo ratings yet
- Management of Tetanus PatientsDocument7 pagesManagement of Tetanus PatientsApple MaeNo ratings yet
- Human Vaccines & Immunotherapeutics: Yong Liu, Xichao Mo, Xiaxia Yu, Jinxin Wang, Jinfei Tian, Jun Kuang & Jie PengDocument10 pagesHuman Vaccines & Immunotherapeutics: Yong Liu, Xichao Mo, Xiaxia Yu, Jinxin Wang, Jinfei Tian, Jun Kuang & Jie PengApple MaeNo ratings yet
- 19a-Reading 1Document28 pages19a-Reading 1Apple MaeNo ratings yet
- Human Vaccines & Immunotherapeutics: Yong Liu, Xichao Mo, Xiaxia Yu, Jinxin Wang, Jinfei Tian, Jun Kuang & Jie PengDocument10 pagesHuman Vaccines & Immunotherapeutics: Yong Liu, Xichao Mo, Xiaxia Yu, Jinxin Wang, Jinfei Tian, Jun Kuang & Jie PengApple MaeNo ratings yet
- NOSUN College of Nursing, Pharmacy and Allied Health SciencesDocument1 pageNOSUN College of Nursing, Pharmacy and Allied Health SciencesApple MaeNo ratings yet
- N OR S U: Egros Iental Tate NiversityDocument2 pagesN OR S U: Egros Iental Tate NiversityApple MaeNo ratings yet
- Medical Management (Schizophrenia)Document5 pagesMedical Management (Schizophrenia)Apple MaeNo ratings yet
- Tetanus (Lockjaw): Causes, Symptoms, Diagnosis and TreatmentDocument5 pagesTetanus (Lockjaw): Causes, Symptoms, Diagnosis and TreatmentApple MaeNo ratings yet
- Related Readings: N OR S UDocument3 pagesRelated Readings: N OR S UApple MaeNo ratings yet
- 8-Growth & DevelopmentDocument1 page8-Growth & DevelopmentApple MaeNo ratings yet
- Dissociative DisordersDocument17 pagesDissociative Disordersapi-3797941100% (4)
- N OR S U: Egros Iental Tate NiversityDocument2 pagesN OR S U: Egros Iental Tate NiversityApple MaeNo ratings yet
- Pathophysiology of Dengue FeverDocument1 pagePathophysiology of Dengue FeverApple Mae100% (1)
- Antipsychotic Drugs: Conventional AntipsychoticsDocument16 pagesAntipsychotic Drugs: Conventional AntipsychoticsApple MaeNo ratings yet
- VITAMIN-E and KDocument4 pagesVITAMIN-E and KApple MaeNo ratings yet
- Nursing ManagementDocument1 pageNursing ManagementApple MaeNo ratings yet
- Minor Surgery Is Defines As A Set of Procedures in Which Short Surgical Techniques Are Applied OnDocument11 pagesMinor Surgery Is Defines As A Set of Procedures in Which Short Surgical Techniques Are Applied OnApple MaeNo ratings yet
- Goals and dreams assignmentDocument3 pagesGoals and dreams assignmentApple MaeNo ratings yet
- N OR S U: Clinical DataDocument2 pagesN OR S U: Clinical DataApple MaeNo ratings yet
- Scenario Liver Cirrhosis Stage 2Document1 pageScenario Liver Cirrhosis Stage 2Apple MaeNo ratings yet
- N OR S U: Egros Iental Tate NiversityDocument2 pagesN OR S U: Egros Iental Tate NiversityApple MaeNo ratings yet
- Pre and Post TestDocument4 pagesPre and Post TestApple MaeNo ratings yet
- Same-Day Surgery Patient Prep ChecklistDocument1 pageSame-Day Surgery Patient Prep ChecklistApple MaeNo ratings yet
- I. Cutting and DissectingDocument10 pagesI. Cutting and DissectingApple MaeNo ratings yet
- Covid-19 Faqs: Last Updated: 2 March 2020Document6 pagesCovid-19 Faqs: Last Updated: 2 March 2020Apple MaeNo ratings yet
- Minor Surgery Procedures GuideDocument11 pagesMinor Surgery Procedures GuideApple MaeNo ratings yet
- Sample Presentation ScriptDocument3 pagesSample Presentation ScriptApple MaeNo ratings yet
- Wound CareDocument6 pagesWound CareApple MaeNo ratings yet
- Eating disorders are not choices but serious mental illnessesDocument2 pagesEating disorders are not choices but serious mental illnessesApple MaeNo ratings yet
- 16-Skin Safety and Health Prevention An Overview of Chemicals in Cosmetic Products (2019) PDFDocument8 pages16-Skin Safety and Health Prevention An Overview of Chemicals in Cosmetic Products (2019) PDFApple MaeNo ratings yet
- TesiDocument9 pagesTesiRian SeptianNo ratings yet
- Practice Test Pediatric Nursing 100 ItemsDocument17 pagesPractice Test Pediatric Nursing 100 ItemsKarla FralalaNo ratings yet
- 2 Vol. 8 Issue 1 January 2017 IJPSR RE 1872Document12 pages2 Vol. 8 Issue 1 January 2017 IJPSR RE 1872Fadhil Muhammad AwaluddinNo ratings yet
- Justificacion 7mm MetalDocument5 pagesJustificacion 7mm MetalMIGUELNo ratings yet
- Physiology Dynamic Study ModulesDocument25 pagesPhysiology Dynamic Study ModulesKaitlyn TranNo ratings yet
- Introduction and Epithelial TissueDocument66 pagesIntroduction and Epithelial Tissueapi-294162496100% (1)
- A Working Manual of High Frequency CurrentsDocument307 pagesA Working Manual of High Frequency CurrentsEmerald Athanasiou100% (2)
- Material Safety Data Sheet: 1. Product and Company IdentificationDocument7 pagesMaterial Safety Data Sheet: 1. Product and Company IdentificationAyan BasakNo ratings yet
- Self Injection Made EasyDocument8 pagesSelf Injection Made EasyJames OkamotoNo ratings yet
- Effects of Transcutaneous Electrical Nerve Stimulation On Pain Pain Sensitivity and Function in People With Knee Osteoarthritis. A Randomized Controlled TrialDocument14 pagesEffects of Transcutaneous Electrical Nerve Stimulation On Pain Pain Sensitivity and Function in People With Knee Osteoarthritis. A Randomized Controlled TrialLorena Rico ArtigasNo ratings yet
- 85800-131 ERBE EN Application Brochure of Gastroenterology D064045Document24 pages85800-131 ERBE EN Application Brochure of Gastroenterology D064045GREYSON QCNo ratings yet
- IEC Submission FormDocument10 pagesIEC Submission FormAbhishek YadavNo ratings yet
- Sy - CCDO2 L3 Diploma in Aromatherapy SpecificataionDocument11 pagesSy - CCDO2 L3 Diploma in Aromatherapy SpecificataionJing CruzNo ratings yet
- Determination of Chlorogenic Acid, Baicalin and Forsythin in Shuanghuanglian Preparations by Hplc-DadDocument6 pagesDetermination of Chlorogenic Acid, Baicalin and Forsythin in Shuanghuanglian Preparations by Hplc-DadAndreeaMadalinaMihailaNo ratings yet
- JShotwell Week6Document50 pagesJShotwell Week6Priyanka GandhiNo ratings yet
- Drug Study ParacetamolDocument1 pageDrug Study ParacetamolIris BalinoNo ratings yet
- State of The Future of Resuscitation Proceedings Web VersionDocument60 pagesState of The Future of Resuscitation Proceedings Web VersionAdiel OjedaNo ratings yet
- Bio PiracyDocument20 pagesBio Piracyapi-3706215No ratings yet
- Necro Sutra Kevin SweeneyDocument13 pagesNecro Sutra Kevin SweeneyRulizNo ratings yet
- Antibiotik Rasional - DR DidiDocument42 pagesAntibiotik Rasional - DR DidiZunni HermawatiNo ratings yet
- Effects of LipokitDocument9 pagesEffects of LipokitIsaac HgNo ratings yet
- Electrical Safety Practices and Physiological EffectsDocument9 pagesElectrical Safety Practices and Physiological EffectsSmr OnlyNo ratings yet
- Bioscalar Energy: The Healing PowerDocument4 pagesBioscalar Energy: The Healing PowerSagarsinh RathodNo ratings yet
- H&H accredited training australasia incDocument139 pagesH&H accredited training australasia incBùi Thắng50% (2)
- NDT 45697 Efficacy of Second Generation Antipsychotics in Patients at 061813Document8 pagesNDT 45697 Efficacy of Second Generation Antipsychotics in Patients at 061813twahyuningsih_16No ratings yet
- Johnson & Johnson's Effective PR Saved TylenolDocument8 pagesJohnson & Johnson's Effective PR Saved Tylenolkusumawi2311No ratings yet
- Mixed Dentition Analysis / Orthodontic Courses by Indian Dental AcademyDocument14 pagesMixed Dentition Analysis / Orthodontic Courses by Indian Dental Academyindian dental academy100% (1)
- McIntyre Et Al-2002-European Journal of NeuroscienceDocument4 pagesMcIntyre Et Al-2002-European Journal of NeuroscienceLaura Elena Amaya DuránNo ratings yet
- Basic First Aid Training1Document30 pagesBasic First Aid Training1Richard LindsayNo ratings yet
- PWD All Outline 130819Document114 pagesPWD All Outline 130819Francis KaikumbaNo ratings yet
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (15)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Summary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (11)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)