You might also like
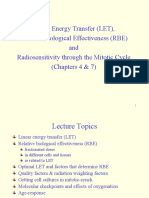
- Linear Energy Transfer (LET), Relative Biological Effectiveness (RBE) and Radiosensitivity Through The Mitotic Cycle (Chapters 4 & 7)Document41 pagesLinear Energy Transfer (LET), Relative Biological Effectiveness (RBE) and Radiosensitivity Through The Mitotic Cycle (Chapters 4 & 7)Silvana OliveiraNo ratings yet
- Fundamental Radiobiology 2019Document54 pagesFundamental Radiobiology 2019Gina R100% (1)
- Linear Quadratic (LQ) Model & Biological Based Treatment Planning - Dr. Manoj GuptaDocument60 pagesLinear Quadratic (LQ) Model & Biological Based Treatment Planning - Dr. Manoj GuptaSudhan Rajan100% (3)
- APPLICATION OF RADIOBIOLOGY PRINCIPLES IN RADIOTHERAPYDocument61 pagesAPPLICATION OF RADIOBIOLOGY PRINCIPLES IN RADIOTHERAPYnilesh kumarNo ratings yet
- NTCP TCPDocument54 pagesNTCP TCPSAlonii Chawla100% (2)
- 4 Radiobiology of Brachytherapy and The Dose-Rate EffectDocument27 pages4 Radiobiology of Brachytherapy and The Dose-Rate EffectDiana MitreaNo ratings yet
- Basics of RadiobiologyDocument61 pagesBasics of RadiobiologyLikhon Amin AponNo ratings yet
- Lethal and Nonlethal Chromosome Aberrations by Gamma Rays and Heavy Ions: A Cytogenetic Perspective On Dose Fractionation in Hadron RadiotherapyDocument10 pagesLethal and Nonlethal Chromosome Aberrations by Gamma Rays and Heavy Ions: A Cytogenetic Perspective On Dose Fractionation in Hadron RadiotherapyNICKNo ratings yet
- Radiobiology Challenge QuestionsDocument3 pagesRadiobiology Challenge QuestionsJhade RelletaNo ratings yet
- 2013-Furusawa-LET Radiobiological Description Carbon IonsDocument9 pages2013-Furusawa-LET Radiobiological Description Carbon Ionsbo zhaoNo ratings yet
- Fundamental Radiobiology OrtonDocument64 pagesFundamental Radiobiology OrtonhitsNo ratings yet
- X Rays, Gamma Rays, Cosmic Rays: Types of MutagensDocument9 pagesX Rays, Gamma Rays, Cosmic Rays: Types of MutagensNi Wayan SuliartiniNo ratings yet
- Bailey Prinsip Radiasi OnkologiDocument9 pagesBailey Prinsip Radiasi OnkologiInes Camilla PutriNo ratings yet
- Altered FractionationDocument49 pagesAltered FractionationShamsudheen CholayilNo ratings yet
- 3 Molecular and Cellular RadbiologyDocument46 pages3 Molecular and Cellular RadbiologyAngelo RamosNo ratings yet
- Radiotherapy: Basic Concepts and Recent AdvancesDocument17 pagesRadiotherapy: Basic Concepts and Recent AdvancesutokaNo ratings yet
- Brain Mets/Palliative/Oligo/Immuno - Breast - CNS/Peds - Constraints - GI - GU - Gyn - H&N/Skin - Heme - Sarcoma - Thorax - Rad Phys/BioDocument59 pagesBrain Mets/Palliative/Oligo/Immuno - Breast - CNS/Peds - Constraints - GI - GU - Gyn - H&N/Skin - Heme - Sarcoma - Thorax - Rad Phys/BioRabiya TahseenNo ratings yet
- Radio BiologyDocument26 pagesRadio BiologyMAN MedanNo ratings yet
- Radiobiology Essentials for Medical ImagingDocument3 pagesRadiobiology Essentials for Medical ImagingdonnaNo ratings yet
- 1 s2.0 S0360301622004187 MainDocument10 pages1 s2.0 S0360301622004187 Mainbo zhaoNo ratings yet
- Biophysical Modeling: Induction of Clustered DNA Lesions by Ionizing Radiation - Insights FromDocument22 pagesBiophysical Modeling: Induction of Clustered DNA Lesions by Ionizing Radiation - Insights FromrickNo ratings yet
- 4T3 Radiation TherapyDocument43 pages4T3 Radiation TherapydanaNo ratings yet
- 2015-Oncotarget-Activation of Homologous Recombination DNA Repair in Human Skin Fibroblasts Continuously Exposed To X-Ray RadiationDocument10 pages2015-Oncotarget-Activation of Homologous Recombination DNA Repair in Human Skin Fibroblasts Continuously Exposed To X-Ray Radiation小熊JoeNo ratings yet
- Lecture - 2 - Bioradiation Radiation Biology - Mechanisms - 1Document7 pagesLecture - 2 - Bioradiation Radiation Biology - Mechanisms - 1Naglaa MostafaNo ratings yet
- Principles of Chemotherapy and Radiation in Gyne-OncoDocument5 pagesPrinciples of Chemotherapy and Radiation in Gyne-OncoChristine Evan HoNo ratings yet
- Treatment of Radiation Induced ErithemaDocument47 pagesTreatment of Radiation Induced ErithemaDimitar FilevskiNo ratings yet
- Exercises With Solutions in Radiation Physics) 5 Radiation BiologyDocument18 pagesExercises With Solutions in Radiation Physics) 5 Radiation BiologyDavitMartinezNo ratings yet
- ANANDocument11 pagesANANAron JaroNo ratings yet
- Sensing of DNA Damage: Advanced Article Xiaohong H. Yang, Lee ZouDocument7 pagesSensing of DNA Damage: Advanced Article Xiaohong H. Yang, Lee ZouqhqhqNo ratings yet
- Tim Henley Report6Document12 pagesTim Henley Report6Timothy Murray HenleyNo ratings yet
- Radiobiology 5 021023Document26 pagesRadiobiology 5 021023Nuha HamedNo ratings yet
- Slide 6Document8 pagesSlide 6MEOW41No ratings yet
- Molecular Biology-Lecture 1 5 QuestionsDocument20 pagesMolecular Biology-Lecture 1 5 QuestionsLara ShayaNo ratings yet
- Rad Bio Weekly NotesDocument3 pagesRad Bio Weekly NotesanyaashleyNo ratings yet
- Mechanism and Regulation of Human Non-Homologous Dna End-JoiningDocument9 pagesMechanism and Regulation of Human Non-Homologous Dna End-JoiningAbi Wombat MendiolitaNo ratings yet
- Radiotherapy: Basic Concepts and Recent Advances: Review ArticleDocument5 pagesRadiotherapy: Basic Concepts and Recent Advances: Review ArticleAde Febrian RamadhanNo ratings yet
- RADT214 202324 Radiobiology 6 031023Document40 pagesRADT214 202324 Radiobiology 6 031023Nuha HamedNo ratings yet
- On The Analysis of Clonogenic Survival Data: Statistical Alternatives To The Linear-Quadratic ModelDocument11 pagesOn The Analysis of Clonogenic Survival Data: Statistical Alternatives To The Linear-Quadratic ModelJesus RFNo ratings yet
- Radiobiology challenge questionsDocument3 pagesRadiobiology challenge questionsJhade RelletaNo ratings yet
- ELECTROGENETICS Summary From Web 1Document4 pagesELECTROGENETICS Summary From Web 1tonym35No ratings yet
- Stress-Induced Telomere Shortening Reduces Mutation Rate and Increases LifespanDocument11 pagesStress-Induced Telomere Shortening Reduces Mutation Rate and Increases LifespanAla TrusinaNo ratings yet
- Units of Radiation DoseDocument20 pagesUnits of Radiation DoseMadduri NithamNo ratings yet
- Quantitative Analysis of The Time-Course of Viral DNA Forms During The HIV-1 Life CycleDocument18 pagesQuantitative Analysis of The Time-Course of Viral DNA Forms During The HIV-1 Life CycleFrançois SAKKALNo ratings yet
- Radiobiology Gyn MarplesDocument26 pagesRadiobiology Gyn MarplesConferinta Tineri RadioterapeutiNo ratings yet
- Radiation OncDocument15 pagesRadiation OncMihreta MustaficNo ratings yet
- Mitochondrial Cytochrome C Oxidase Is Not The Primary AcceptorDocument8 pagesMitochondrial Cytochrome C Oxidase Is Not The Primary AcceptorAlejandro HerreraNo ratings yet
- Dissertation NMRDocument5 pagesDissertation NMRFindSomeoneToWriteMyCollegePaperUK100% (1)
- Radio BiologyDocument7 pagesRadio BiologyLucelle CoquillaNo ratings yet
- Radiobiology Behind Dose FractionationDocument86 pagesRadiobiology Behind Dose Fractionationgudeksha100% (1)
- DNA - Interactive Angents: Phạm Thu Trang: 21001842 Phan Trần Thảo Vy: 21001850Document9 pagesDNA - Interactive Angents: Phạm Thu Trang: 21001842 Phan Trần Thảo Vy: 21001850Phạm Thu TrangNo ratings yet
- BED Formula PDFDocument15 pagesBED Formula PDFMichelle Mora MariñoNo ratings yet
- 2 Fundamental Principles of Radiobiology PDFDocument27 pages2 Fundamental Principles of Radiobiology PDFAngelo RamosNo ratings yet
- Basic Molecular BiologyDocument10 pagesBasic Molecular BiologyPaolaNo ratings yet
- Cytogenetic Aspects of Neutron - Cytogenetic Aspects of Neutron-Induced Cellular ResponseDocument15 pagesCytogenetic Aspects of Neutron - Cytogenetic Aspects of Neutron-Induced Cellular Responseisee journalNo ratings yet
- Mod Rich 2006Document6 pagesMod Rich 2006Macarena Fernández VillarroelNo ratings yet
- Lecture - 5 - Elements of Radiation BiologyDocument46 pagesLecture - 5 - Elements of Radiation Biologyhannan alnzi100% (1)
- Radiobiology principlesDocument3 pagesRadiobiology principlesAloha GosiengfiaoNo ratings yet
- Mbii - l15 - Dna RepairDocument6 pagesMbii - l15 - Dna RepairMiles NsgNo ratings yet
- Radiobiology Iaea DiapositivasDocument88 pagesRadiobiology Iaea DiapositivasLida Velasquez SierraNo ratings yet
- Analytical Characterization of BiotherapeuticsFrom EverandAnalytical Characterization of BiotherapeuticsJennie R. LillNo ratings yet
- EK Chemistry PDFDocument364 pagesEK Chemistry PDFray100% (8)
- Radiation Oncology Prioritisation Guidelines SummaryDocument4 pagesRadiation Oncology Prioritisation Guidelines SummaryrayNo ratings yet
- Palliative Radiotherapy WorksheetDocument4 pagesPalliative Radiotherapy WorksheetrayNo ratings yet
- ProcedureDocument13 pagesProcedurerayNo ratings yet
- Even/homogenous Dose Distribution Across PTV: WedgesDocument5 pagesEven/homogenous Dose Distribution Across PTV: WedgesrayNo ratings yet
- 501 Critical Reading QuestionsDocument283 pages501 Critical Reading Questionsapi-3813392100% (9)
- RADT115 2014 Test 2 Posted On Moodle On 9 May 16Document5 pagesRADT115 2014 Test 2 Posted On Moodle On 9 May 16rayNo ratings yet
- UMAT 2016 Short Test BookletDocument36 pagesUMAT 2016 Short Test BookletAnonymous rJmcI51No ratings yet
- Rebound Returns - Asos Private Bag 211022 Laurence Stevens Drive Auckland 2154 Freepost No 252061Document1 pageRebound Returns - Asos Private Bag 211022 Laurence Stevens Drive Auckland 2154 Freepost No 252061rayNo ratings yet
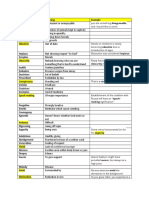
- Medical Word Meanings and ExamplesDocument9 pagesMedical Word Meanings and ExamplesrayNo ratings yet
- Rad 112 Cancer Cell BiologyDocument7 pagesRad 112 Cancer Cell BiologyrayNo ratings yet
- Word Definitions and ExamplesDocument8 pagesWord Definitions and ExamplesrayNo ratings yet
- Cervix WorksheetDocument4 pagesCervix WorksheetrayNo ratings yet
- MU Calc AnswersDocument2 pagesMU Calc AnswersrayNo ratings yet
- Radt 215Document5 pagesRadt 215rayNo ratings yet
- BREAST Worksheet: Treatment Site: Right BreastDocument4 pagesBREAST Worksheet: Treatment Site: Right BreastrayNo ratings yet
- Case StudyDocument8 pagesCase StudyrayNo ratings yet
- Word Definitions and ExamplesDocument8 pagesWord Definitions and ExamplesrayNo ratings yet
- Case Study: Raymond HoveDocument20 pagesCase Study: Raymond HoverayNo ratings yet
- Cervix Formative AssesmentDocument4 pagesCervix Formative AssesmentrayNo ratings yet
- 10cm 1 10cm 1 10cm 1: Decreased FF Increased MUDocument2 pages10cm 1 10cm 1 10cm 1: Decreased FF Increased MUrayNo ratings yet
- Radiobio EQD2 QuestionsDocument2 pagesRadiobio EQD2 QuestionsrayNo ratings yet
- Brain Module WorksheetDocument5 pagesBrain Module WorksheetrayNo ratings yet
- New Patient Nutrition Assessment Form: (Person 1)Document12 pagesNew Patient Nutrition Assessment Form: (Person 1)Ayesha KhanNo ratings yet
- Effect of Textile Industry On Health FinalDocument2 pagesEffect of Textile Industry On Health FinalSudhir Jain100% (1)
- AS 1680.0-1998 Interior Lighting-Safe MovementDocument17 pagesAS 1680.0-1998 Interior Lighting-Safe Movementvxzvzxvzv0% (1)
- Nueva Ecija University of Science and Technology: Republic of The Philippines Cabanatuan CityDocument3 pagesNueva Ecija University of Science and Technology: Republic of The Philippines Cabanatuan CityKazuhero LagranaNo ratings yet
- Rheumatoid Arthritis Drug StudyDocument2 pagesRheumatoid Arthritis Drug StudyChristaNo ratings yet
- The Importance of NutritionDocument16 pagesThe Importance of NutritionRonna DipasupilNo ratings yet
- 50 Pediatric Anesthesia Questions: © 2004, Roy G. Soto, M.DDocument4 pages50 Pediatric Anesthesia Questions: © 2004, Roy G. Soto, M.DGanda SilitongaNo ratings yet
- Saudi Medical Licensing Examination - R (J) S3 Final 1 - R (HA and JW)Document9 pagesSaudi Medical Licensing Examination - R (J) S3 Final 1 - R (HA and JW)malik003No ratings yet
- Discuss Thoracic IncisionsDocument47 pagesDiscuss Thoracic IncisionsSucipto HartonoNo ratings yet
- Renal MCQ 4Document10 pagesRenal MCQ 4AzizNo ratings yet
- Trend Analysis of Exponential Increase of COVID-19 Cases in Pakistan: An InterpretationDocument21 pagesTrend Analysis of Exponential Increase of COVID-19 Cases in Pakistan: An InterpretationBongoNo ratings yet
- AAO - External Disease and CorneaDocument19 pagesAAO - External Disease and CorneaJohn Paul VillaflorNo ratings yet
- Print Kil DavidDocument9 pagesPrint Kil Davidapi-3806285No ratings yet
- Four Scenarios for the Future of BioSciences Report HighlightsDocument8 pagesFour Scenarios for the Future of BioSciences Report HighlightsTejaNo ratings yet
- Actue Management of Pneumonia in Adults PatienitDocument8 pagesActue Management of Pneumonia in Adults Patienitxiomara torresNo ratings yet
- Test Bank Fundamentals Nursing Care Skills 2nd Edition Ludwig BurtonDocument18 pagesTest Bank Fundamentals Nursing Care Skills 2nd Edition Ludwig Burtontammyshaffer12052000mfe100% (13)
- Nanotech MedDocument12 pagesNanotech MedDaphane Kate AureadaNo ratings yet
- 2007 CASLPA Position Paper On Dysphagia in AdultsDocument8 pages2007 CASLPA Position Paper On Dysphagia in AdultsEva Sala RenauNo ratings yet
- Science Investigatory ProjectDocument16 pagesScience Investigatory ProjectZaira CasubuanNo ratings yet
- PTB Case-StudyDocument64 pagesPTB Case-StudyBeverly DatuNo ratings yet
- Autonomic Nervous SystemDocument13 pagesAutonomic Nervous SystemSreejesh Rk100% (1)
- Corpus Alienum VaginaeDocument3 pagesCorpus Alienum VaginaeIntan PermataNo ratings yet
- Powders and GranulesDocument18 pagesPowders and GranulesAlaa Salymeh100% (1)
- Daftar PustakaDocument2 pagesDaftar PustakaYuli ErmaNo ratings yet
- Principles of GeneticsDocument161 pagesPrinciples of GeneticsSomeone100% (3)
- Module 13 Taking Charge of Ones Health 1Document18 pagesModule 13 Taking Charge of Ones Health 1Jandrei Ezekiel LausNo ratings yet
- Analysis of Survival Data - LN - D Zhang - 05Document264 pagesAnalysis of Survival Data - LN - D Zhang - 05mirceacomanro2740100% (1)
- Subconjunctival HaemorrhageDocument7 pagesSubconjunctival HaemorrhageTry Ahmad MirzaNo ratings yet
- Dengue Hemorrhagic FeverDocument54 pagesDengue Hemorrhagic FeverfortuneayaNo ratings yet
- Α Α Α Α-Amylase-Eps: Biosystems S.ADocument1 pageΑ Α Α Α-Amylase-Eps: Biosystems S.ARisqon Anjahiranda AdiputraNo ratings yet