Volume 5, Issue 5, May – 2020 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
The Silent Anaemia Epidemic in Children
Samuel Mwesige Annete Nankwanga
Department of Biochemistry Department of Biochemistry and Sports Science
School of Health Sciences School of Biosciences, College of Natural Sciences
Soroti University, Uganda Makerere University, Uganda
Didas Mushabe
Medical Research Council,
Uganda Virus Research Institute, LSHTM, Uganda.
Abstract:- Anaemia (haemoglobin level < 11 g/dl) is a the prevalence was at 22% amongst adolescents and adults
silent epidemic that affects about 293.1 million children aged 16years and over (Akwale et al, 2004). Presently,
aged <5 years worldwide with 28.5% of those located in Global estimate of childhood Anaemia is at 293.1 million
sub-Sahara Africa. Child hood Anaemia is associated children aged <5 years with 28.5% of those located in Sub-
with poor cognition, reduced growth, problems with Sahara Africa. Child hood Anaemia is associated with
immune function and ultimately decreased survival. increased risk of death, impairment of the cognitive and
Uganda’s childhood Anaemia is insidious, multifactorial motor development, growth, immune function and physical
and undefined. The objectives of the study were to work capacity and ultimately decreased survival (Soares,
determine the prevalence, severity and leading cause of 2011).
Anaemia amongst children ≤ 12 years attending Virika
hospital. The cross-sectional study employed both Anaemia is usually multifactorial in origin with
qualitative and semi-quantitative methods. Participants malaria playing a key aetiologic role in endemic countries
were sampled by convenience and simple random like tropical regions. Infants are vulnerable to malaria from
techniques. Parents were given short interviews to the age of approximately three months, when the immunity
obtain participants demographic and necessary acquired from the mothers starts to wear off. Hospital series
information. Blood, stool and anthropometric show that in the areas of intense transmission, most cases of
measurements were obtained from the participants and severe malarial Anaemia, blood transfusions, and deaths
tested for complete blood count, malaria, HIV, sickle occur in infants and children less than five years old
cell disease, helminthes and malnutrition respectively. (Biemba et al, 2000). Malaria causes Anaemia through
Data was analyzed using Excel computer program. haemolysis and increased splenic clearance of red blood
cells and cytokine- induced dyserythropoesis (Mendez,
Results show that Prevalence of Anaemia in 2000, Nagel, 2002 & Ekvall, 2003). Severe malarial
children is high, presenting mostly in moderate form. Anaemia is presumed to account for more than half of all
Malnutrition plays a major role in the development of childhood deaths in Africa with case fatality rates in
Anaemia. Nutritional support and awareness are key hospitals ranging between 8% and 18% (Slutcher et al,
aspects in prevention of Anaemia development and 1994). Case fatality from severe Anaemia in the community
progression. Other control interventions may include is likely to be much higher, since the majority of the
provision of improved diagnostic tests, optimizing hospital cases will have received a lifesaving blood
compliance, appropriating referral practices, transfusion.
implementation of standard treatment guidelines and
research. HIV/AIDS is another factor that has been linked to
childhood Anaemia. HIV causes cytokine-mediated
Keywords:- Anaemia, Prevalence, Severity and Etiology. inflammation, resulting into iron sequestration in
macrophages and decreased iron absorption in the small
I. INTRODUCTION intestines. A number of studies carried out in high HIV
prevalence areas concur that there is a strong association
Anaemia (haemoglobin level < 11 g/dl) remains one between HIV/AIDS and Anaemia (Mukaya (2009, Calis et
of the most intractable public health problems affecting al, 2008 & Lewis et al, 2005). School age children are fond
more than half of all pregnant women and children less of harboring the greatest number of worms, with children
than 5 years old (Demaeyer et al, 1995 & Cheesbrough, below 24 months having intestinal helminthes infection rate
2006). In 1993-2005, nearly 300 million children ranging from 2% to 80% (Montresor et al, 2000). This puts
worldwide had Anaemia while in Sub Saharan Africa, two children at risk of Anaemia since worms are associated to
thirds (83.5 million children) were Anaemic (Soares, 2011). iron deficiency (Tatale et al, 1998). Out of more than 10
In West Africa, the numbers of childhood Anaemia cases million deaths that occur each year in children less than
were highest in Burkina Faso, followed by Ghana and Mali five years old in developing countries, malnutrition
with malnutrition playing a central causative role in attributes half of the deaths directly or indirectly (Black et
preschool children (Soares, 2011). In Tanzania, the al, 2003). Poor nutrition and micronutrient deficiencies
prevalence of Anaemia amongst people aged 15-65 years exacerbate severity of infectious diseases resulting into
was estimated at 43.4% (Tatala et al, 1998) while in Kenya Anaemia. Many African children live in a state of
IJISRT20MAY776 www.ijisrt.com 1087
Volume 5, Issue 5, May – 2020 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
precarious iron balance which affects their erythropoietic II. MATERIALS AND METHODS
activities leading to Anaemia. Infants with a low total body
index as a consequence of low birth weight or maternal iron A. Study design and population set up
deficiency are particularly prone to iron deficiency and Across-sectional study was designed to determine the
Anaemia. Haemoglobinopathies are clinical syndromes prevalence, severity and leading cause of Anaemia in
resulting from disorders of haemoglobin (Cheesbrough, children ≤12 years who were attending outpatient
2006). These abnormalities are categorized into cultural department Virika hospital. The study was conducted in a
variants, failure to synthesize haemoglobin and failure to period of 50 days from May to July 2012 at Virika hospital,
complete the normal neonatal switch from fetal to adult Kabarole district. A sample size of 230 children were
haemoglobin. The commonest of these disorders are sickle enrolled following exclusion and inclusion criteria.
cell disease. The homozygous form of sickle cell disease is
caused by substitution of valine instead of glutamic acid in B. Methods and laboratory analyses
position 6 of the B- globin chain. As a result of this, The study employed both qualitative and semi-
abnormal haemoglobin is formed which has poor solubility quantitative methods which allowed the researcher to
and deformability in the de-oxygenated state and can obtain demographic and numerical data from the
polymerize within the red blood cells. The red blood cells participants. Demographic information, blood and stool
show a characteristic change due to polymer formation, samples were collected (MOH, 2008) from every child after
they become distorted and rigid hence sickle cells. These consent was sought from the parent/guardian. Every
rigid cells block blood capillaries resulting into haemolytic participant underwent a blood tests for haemoglobin
Anaemia (Cheesbrough, 2006). In light of the above, it is concentration, HIV, malaria, sickle cell disease, stool test
crystal clear that malaria, helminthes, malnutrition, for helminthes infection and assessment for nutritional
heamoglobinopathies and HIV/AIDS play a big in the status.
development of Anaemia. This study took the opportunity
to assess presence of the above aetiological factors in Haemoglobin measurement: Venous blood was
children and determine the leading cause of Anaemia as aseptically drawn from antecubital or great saphenous
one of the study objectives. vein into an EDTA tube (Sarstedt AG & Co,
Numbrecht, Germany) from the participant. The tube
Anaemia most times is insidious. The moderate to was gently inverted 8-10 times to enable thorough
mild Anaemia forms remain undetected by health workers mixing. A complete blood count (CBC) was performed
and in the community resulting into silent morbidity and to estimate haemoglobin concentrations using
mortality. In management of Anaemia, blood transfusion is Humacount haematology analyser.
routinely used as supportive treatment for severe Anaemia
based on patients’ haemoglobin levels. However, most Malaria microscopy: A drop of capillary blood
hospitals still use inaccurate haemoglobinometers that may aseptically collected from the participant’s finger/ heel
produce imprecise results. This implies that there are higher was spread on the glass slide to make a thick smear
chances that blood transfusion is prescribed on basis of (Cheesbrough, 2006). Following air-drying, the smear
inaccurate haemoglobin measurement which squarely was stained by Field technique (Warhurst & Williams,
exposes patients to HIV and other blood-borne pathogens. 1996) and examined for presence of malaria parasites
Additionally, Blood transfusion itself is a costly medical using Zeiss microscope.
practice and that also requires trained personnel. Virika
hospital blood transfusion (2011) report indicates that a HIV serology: HIV antibody testing was carried out on
good number of children below 12 years admitted at the the participants’ EDTA venous blood using the National
hospital are associated with Anaemia and every four out of HIV testing algorithm comprised of Determine, Stat-
ten hospitalized children receive blood transfusion. pak and Unigold kits (supplied by Abbot Systems)
Furthermore, a higher percentage of child death at the
hospital has been also linked to Anaemia (HFVH, 2010), a Sickle cell test: The patient’s EDTA blood sample was
hypothesis that needs to be verified. subjected to the standard heamoglobin solubility test
followed by a variety of centrifugation and filtration
The purpose of this study is to (1) determine the procedures. The resultant haemoglobin was measured
prevalence of Anaemia in children ≤12 years attending spectrophotometrically and categorized into phenotype
Virika hospital, (2) determine the severity of Anaemia AA, AS or SS (Randolph, 2012).
amongst the children, and (3) examine the leading cause of
Anaemia amongst the children. Stool analysis: 2grams of stool was collected from each
participant in a stool container upon instructions given
to the guardian. The samples were processed by direct
preparation and formal saline methods (Sartaj et. al.,
1991) and the slides examined for parasites using Zeiss
microscope.
IJISRT20MAY776 www.ijisrt.com 1088
Volume 5, Issue 5, May – 2020 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
Nutritional status assessment: Anthropometric
assessment of every participant’s weight, age and height
was done. Body mass index (BMI) was calculated and
compared to with percentiles of age on Center for
Disease Control/ National Center of Health Statistics
BMI growth chart for children to obtain the participants
nutritional status (Tamsin et, al., 2003)
C. Quality control
Every respondent was given a number and allowed to
participate only once in the study to avoid repetition of test
results. Both positive and negative controls were included
in every days testing of participants samples. All laboratory
analyses followed the standard operating procedures.
D. Ethical consideration
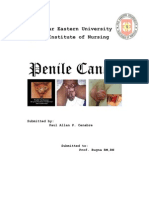
Fig 1:- Shows frequency and percentage distribution of
Written ethical approval was obtained from the
mild, moderate and severe degrees of Anaemia amongst the
Faculty of Research and Ethics Committee (FREC)
subjects
department of Mbarara University of Science and
Technology. Permission was also sought from Virika
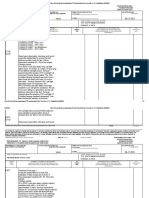
C. Aetiology of Anaemia
hospital administration who allowed the study to take place.
Out of 102 Anaemic clients, 38 (37%) were associated
Informed consent was sought from all the subjects who
with malnutrition, 35 (34.3%) had malaria, 9 (8.8%) had
participated in the study. All information obtained from the
helminthes, 8 (7.8%) had sickle cell disorder, 2 (1.7%) had
study was kept confidential.
HIV/AIDS and 10 (10.4%) had unknown aetiology.
Malnutrition contributed to highest number of anaemia
E. Data analysis
cases
Data was cleaned, entered into excel for analysis and
presented in form of frequency tables and figures.
III. RESULTS
The study was hospital based, a reason that could
explain the 100% response rate. Out of 230 children, 132
(57%) were females while 98 (43%) were males.
A. Prevalence of Anaemia
The number of children with Anaemia was 102 (44%)
while those without Anaemia were 128 (56%). In the study,
prevalence meant the percentage of children diagnosed with
Anaemia, therefore prevalence was 44%.
Subject Frequency Percentage
Distribution
Anaemia 102 44
No Anaemia 128 56
Fig 2:- Shows percentage causes of Anaemia
Table 1:- Shows frequency and percentage distribution of
Anaemia amongst the subjects
IV. DISCUSSION
B. Severity of Anaemia
The cross-sectional study was conducted at Virika
Severity of Anaemia referred to as degree of its
hospital, where 230 children were recruited by convenience
presentation. Out of 102 Anaemic clients, 20 (19.7%) had
and simple random sampling. Social-demographic data and
severe Anaemia, 42 (41.1%) had moderate Anaemia and 40
clinical details were collected. Blood samples were
(39.2%) had mild Anaemia.
collected and analyzed for CBC, malaria, HIV, Sickle cell
disorder and stool for presence of helminthes. The
participants’ nutritional status was done by
anthropometrically assessing their weight, age and height.
Results indicated that prevalence of Anaemia was 44%
(102 patients). The high burden of Anaemia was attributed
to its insidious nature that allows affected patients live in
silence death without being diagnosed or treated. The
IJISRT20MAY776 www.ijisrt.com 1089
Volume 5, Issue 5, May – 2020 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
second reason was public unawareness of the silent integrated HIV-care network in Rwenzori region that has
epidemic given the fact that 89.9% of the study participants played an important role in HIV prevention and
showed knowledge gap on interviews. management. 10% of the Anaemia cases were of unknown
cause. This calls for more studies in Anaemia aetiology,
Mukaya (2009) conducted a similar cross- sectional prevention and treatment.
descriptive study in the emergency Medical ward of
Mulago hospital, where 395 patients were recruited by V. CONCLUSION
systematic random sampling. A complete blood count and
peripheral film examination were done. Results indicated Prevalence of Anaemia in children is high in moderate
Anaemia prevalence of 64.6%, a high value that can be form and malnutrition is a major predisposing factor. The
linked to chronic diseases common among patients control of Anaemia should be made a priority by
attending Medical ward of Mulago hospital. Another considering an integrated community and hospital based
similar study was carried out by Mbuya (2003) using approach involving diagnostics, treatment, prevention and
cluster sampling to survey 2417 households at random in research strands.
four contiguous districts in south- eastern United Republic
of Tanzania in mid-1999. Overall, 58 %( 1722) of RECOMMENDATIONS
participants had Hb <11g/dl, 39 % (775) had Hb <8g/dl
and 3 %( 65) had Hb <5g/dl. The study also found out that The government should provide a community based
the highest prevalence of Anaemia of all the three levels nutritional support program targeting high risk groups such
was in children aged 6-11 months. Both studies by Mukaya as giving supplements to children and educating parents on
(2009) and Mbuya (2003) concur with this present study nutritional values.
that Anaemia is indeed a silent epidemic that calls for
urgent intervention such as availing of improved diagnostic Ministry of Health should design Anaemia control
tests, optimizing compliance, appropriating referral programs that could include availability of improved
practices and treatment guidelines. diagnostic tests, optimizing compliance, appropriating
referral practices and implementation of standard treatment
The study also assessed degree of presentation of guidelines.
Anaemia amongst the participants. Out of 102 Anaemic
clients, 20 (19.7%) had Severe Anaemia, 42 (41.1%) had Allocating funds into Anaemia research.
Moderate Anaemia and 40 (39.2%) had Mild Anaemia.
Majority of the children who had Moderate- Mild Anaemia Conflict of interest
had no clinical signs, a condition that could slowly enhance Authors declare no conflict of interest
progression of the disease to its severe state. Two similar
studies by Soares (2011) and Mukaya (2009) carried out in ACKNOWLEDGMENTS
West Africa and Uganda respectively also depicted
Moderate Anaemia as the highest degree of presentation. The main author wishes to thank the co-authors for
This burden requires a concerted effort such as community the supervision and academic contribution towards this
based Anaemia control programs and appropriating funds report. Our sincere gratitude to the subjects who
into research to develop better diagnostic and treatment participated in study.
targets.
REFERENCES
Out of 102 Anaemic clients, 38 (37%) were associated
with malnutrition, 35 (34.3%) had malaria, 9 (8.8%) had [1]. Akwale WS, Lum JK, Kaneko A et al (2004).
helminthes, 8 (7.8%) had sickle cell disease, 2 (1.7%) had Anaemia and malaria at different altitudes in the
HIV/AIDS and 10 (10.4%) were of unknown cause. The western highlands of Kenya; 91[2]; 167-175
leading cause of Anaemia was malnutrition, which was also [2]. Black RE, Morris SS, Bryce J. (2003). Where and
reflected in the poor feeding habits amongst the why are 10 million children dying every year? Lancet
participants. Under nutrition in children leads to 361; 2226-2234.
micronutrient deficiency like iron. This affects [3]. Biemba G, Dolmans D, Thuma PE, Weiss G, Gordeuk
erythropoeitc activities as well as aggravating severity of VR. (2000). Severe anaemia in Zambian children with
other diseases, resulting into Anaemia. Malaria was second plasmodium falciparum malaria. Trop Med int. Health
to malnutrition despite participants reporting regular use of 5; 9-16.
ITN’s and observing other malaria control measures. [4]. Calis JC, Phiri KS, Faragher EB, et al (2008). Severe
Malarial Anaemia was high among children who either had anaemia in Malawian children. Nengl J Med; 358[9];
severe or poorly treated malaria. Helminthic Anaemia was 888-899.
majorly due to hookworm infection observed in children [5]. Cheesbrough, M. (2006). District laboratory practice
under five years of age. Sickle cell disorder (HBSS or in tropical countries. 2nd edition. United States of
HBAS) was observed in 7.3% of Anaemic participants. America: Cambridge University press.
HBSS and HBAS accounted for 90% and 10% of sickle [6]. Demaeyer, E. (1985). The prevalence of anaemia in
cell Anaemia respectively. HIV/AIDS was least (1.7%) of the world. Geneva: World Health Organization. Stat
the aetiological factors. This is probably because of an Q38; 302-316.
IJISRT20MAY776 www.ijisrt.com 1090
Volume 5, Issue 5, May – 2020 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
[7]. Ekvall, H. (2003). Malaria and anaemia. Curr opin [22]. Tatale S, Svanberg U, Mduma B. (1998). Low dietary
Hematol. 10; 108-144. iron availability is a major cause of anaemia, a
[8]. HFVH, (2010). Orientation guideline for new nutrition survey in the lindi district of Tanzania. Am J
employees. Holy Family Virika Hospital: Board of clin Nutr; 68[1]; 171-178.
directors. [23]. Virika hospital blood transfusion report (2011).
[9]. Humacount haematology analyzer user manual 2.5 Annual health report, laboratory department.
release. Human diagnostics worldwide. Germany, pgs [24]. Warhurst D. C, Williams J. E. (1996). Laboratory
6and11. diagnosis of Malaria, PHLS Malaria Reference
[10]. Lewis DK, et al (2005). Treatable factors associated Laboratory, London School of Hygiene and Tropical
with severe anaemia in adults in medical wards in Medicine. J clini Pathol 1996; 49;533-538
Blantyre-malawi, an area of high HIV sero-
prevalence. Trans R soc Trop med Hyg; 99(8); 561-
567.
[11]. Mbuya, C. (2003). The silent burden of anaemia in
Tanzanian children; a community based study by
Tanzania essential Health interventions project, united
republic of Tanzania: Ministry of Health.
[12]. Menendez C, Fleming AF, Alonso PL. (2000).
Malaria-related anaemia. Parasitol today 16; 469-476.
[13]. Mukaya JE, Ddungu H, Ssali F, O’shea T, Crowther
MA. (2009). Prevalence and morphological types of
anaemia and hookworm infestation in medical
emergence ward at Mulago Hospital. Kampala:
Makerere University. 99; 881-886.
[14]. MOH (2008). Standard operating procedures for
essential laboratory tests. Uganda; AMREF. pgs2, 4,
6, 12, 18 and 90.
[15]. Montressor A, Awasthi S, Crompton DW. (2003). Use
of benzimidazoles in children younger than 24 months
for the treatment of soil transmitted helminthiasis.
Acta Trop 86;223-232
[16]. Nagel RL. (2002). Malarial anaemia. 26; 329-343.
[17]. Randolph TR, Wheelhouse J. (2012). Novel test
method (sickle confirm) to differentiate sickle cell
anaemia from sickle cell trait for potential use in
developing countries. Clin Lab Sci. 25(1):26-34
[18]. Sartaj Wali, Nisar Ahmed, Mirza Naqi Zafar. (1991).
Laboratory techniques for examination of interstinal
parasites.s Dr. Ziauddin hospital Laboratory, Ziauddin
hospital, Allama Rashid Turabi Road, Karachi.
[19]. Slutcher L, Taylor TE, Wirima JJ, Steketee RW.
(1994). Hospital morbidity and mortality due to
malaria associated severe anaemia in two areas of
Malawi with different patterns of malaria infections.
Trans R soc Trop Med Hyg 88; 548-551.
[20]. Soares M, Archie CA. (2011). Mapping the risk of
anaemia in preschool-age children; the contribution of
malnutrition, malaria and helminthes infections in
East Africa. Kenya: Kenya medical research institute.
PLOS med 8[6]; e1000438. Doi; 10.1371/journal.
Pmed. 1000438. Email; rmagalhaes@sph.uq.edu.au.
[21]. Tamsin Knox A, Melissa Zafonte-Sanders, Cade
Fields-Gardener, Karol Moen, Diana Johansen,
Nicholas Paton. (2003). Assessment of nutritional
status, body composition and Human
Immunodeficiency Virus-associated morphologic
changes. Clinical infectious Diseases, Volume 36,
Issue Suppliment. Pages S63-S68.
IJISRT20MAY776 www.ijisrt.com 1091
You might also like
- Evidence of Harm: Mercury in Vaccines and the Autism Epidemic: A Medical ControversyFrom EverandEvidence of Harm: Mercury in Vaccines and the Autism Epidemic: A Medical ControversyRating: 4 out of 5 stars4/5 (13)
- JurnaL MalariaDocument10 pagesJurnaL Malariamufida harianiNo ratings yet
- Multiple Myeloma and Other Plasma Cell NeoplasmsFrom EverandMultiple Myeloma and Other Plasma Cell NeoplasmsMeletios A. DimopoulosNo ratings yet
- Hypoglycemia and Anemia Associated With Malaria Among Pregnant Mothers Living With HIV Attending Aminu Kano Teaching Hospital, Kano State-NigeriaDocument6 pagesHypoglycemia and Anemia Associated With Malaria Among Pregnant Mothers Living With HIV Attending Aminu Kano Teaching Hospital, Kano State-NigeriaUMYU Journal of Microbiology Research (UJMR)No ratings yet
- The Relationship Between Malnutrition, Immunity and Malaria Transmission in ChildrenDocument7 pagesThe Relationship Between Malnutrition, Immunity and Malaria Transmission in Childrensandeep raiNo ratings yet
- Childhood Iron Deficiency Anemia Leads To Recurrent Respiratory Tract Infections and GastroenteritisDocument8 pagesChildhood Iron Deficiency Anemia Leads To Recurrent Respiratory Tract Infections and GastroenteritisAbdurrahman HasanuddinNo ratings yet
- Research Article: Longer Breastfeeding Associated With Childhood Anemia in Rural South-Eastern NigeriaDocument7 pagesResearch Article: Longer Breastfeeding Associated With Childhood Anemia in Rural South-Eastern NigeriaRayhand MubarakhNo ratings yet
- Anemia Kerangka TeoriDocument10 pagesAnemia Kerangka TeoriHasan BasriNo ratings yet
- Semalign Samuel - Teshale Darebo - Derese Tamiru Desta - Afework MulugetaDocument10 pagesSemalign Samuel - Teshale Darebo - Derese Tamiru Desta - Afework MulugetaAjay DNo ratings yet
- Anemia and Associated Factors Among Adolescent Girls Living in Aw-Barre Refugee Camp, Somali Regional State, Southeast EthiopiaDocument12 pagesAnemia and Associated Factors Among Adolescent Girls Living in Aw-Barre Refugee Camp, Somali Regional State, Southeast EthiopiaEzhaty Diah RianiNo ratings yet
- Research ArticleDocument7 pagesResearch ArticleerikaNo ratings yet
- Project WorkDocument45 pagesProject WorkFanenter EmmanuelNo ratings yet
- Abubakar Et AlDocument5 pagesAbubakar Et Alkang.asep008No ratings yet
- 15 - 93-98 Ujmr 034Document6 pages15 - 93-98 Ujmr 034KHADIJA TELANo ratings yet
- AnemiaDocument9 pagesAnemiaJhonatan David Diaz IdarragaNo ratings yet
- Anemia2014 108593Document9 pagesAnemia2014 108593AaronMaroonFiveNo ratings yet
- 1471 2334 13 123Document10 pages1471 2334 13 123Laurelle Winnie Kouankep WandjiNo ratings yet
- Bacteriological Prevalence Tuberculosis Among Children Seen Health Facilities Nasarawa State Nigeria 2576 8484 EAST 18 121Document5 pagesBacteriological Prevalence Tuberculosis Among Children Seen Health Facilities Nasarawa State Nigeria 2576 8484 EAST 18 121fatimakh462No ratings yet
- Iron Deficiency Anemia Among Preschooi Children (2-5) Years in Gaza StripDocument17 pagesIron Deficiency Anemia Among Preschooi Children (2-5) Years in Gaza StripMohammedAAl-HaddadAbo-alaaNo ratings yet
- 2020Document18 pages2020SANDIE SORELLENo ratings yet
- International Journal Health Research: Peer-Reviewed Online JournalDocument6 pagesInternational Journal Health Research: Peer-Reviewed Online JournaldsNo ratings yet
- Journal of Parasitology: Prevalence of Parasitic Infections in Children of Boke, GuineaDocument7 pagesJournal of Parasitology: Prevalence of Parasitic Infections in Children of Boke, GuineaSohrab RohaneNo ratings yet
- Journal Pmed 1003787Document20 pagesJournal Pmed 1003787GAYATHIRINo ratings yet
- Prevalence of Anemia Among Pregnant Women Attending Antenatal Care at Tikur Anbessa Specialized Hospital Addis Ababa Ethiopia 2329 8790.1000125Document6 pagesPrevalence of Anemia Among Pregnant Women Attending Antenatal Care at Tikur Anbessa Specialized Hospital Addis Ababa Ethiopia 2329 8790.1000125thaynara robertoNo ratings yet
- C3A826C63688Document8 pagesC3A826C63688LAWSON IYENE-EMINo ratings yet
- The Lancet Regional Health - Western PacificDocument7 pagesThe Lancet Regional Health - Western PacificDeddy DeddyNo ratings yet
- Malaria JournalDocument5 pagesMalaria JournalUDNo ratings yet
- Anemia Prevalence, Severity Level and Its Predictors Among Antenatal Care Attending Pregnant Women in Butajira General Hospital Southern EthiopiaDocument9 pagesAnemia Prevalence, Severity Level and Its Predictors Among Antenatal Care Attending Pregnant Women in Butajira General Hospital Southern EthiopiaJournal of Nutritional Science and Healthy DietNo ratings yet
- Global Trends of Diarrhea Diseases in Children: February 2018Document16 pagesGlobal Trends of Diarrhea Diseases in Children: February 2018Lisa SariNo ratings yet
- NullDocument9 pagesNullAliah FadhillahNo ratings yet
- 1 - s2.0 - S1525505020307769 - Main With Cover Page v2Document8 pages1 - s2.0 - S1525505020307769 - Main With Cover Page v2nurhasanah nanaNo ratings yet
- Deworming As A Measure of The Prevalence of Soil Transmitted Helminths Among Primary School Children in Bonny Local Government Area of Rivers StateDocument8 pagesDeworming As A Measure of The Prevalence of Soil Transmitted Helminths Among Primary School Children in Bonny Local Government Area of Rivers StateInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Correlation Between Malaria and Anemia: A Review: Nelini, Ramadhan TosepuDocument9 pagesThe Correlation Between Malaria and Anemia: A Review: Nelini, Ramadhan TosepuNeliniNo ratings yet
- Habitos Dietarios Asociados Con Anemia GestacionalDocument8 pagesHabitos Dietarios Asociados Con Anemia GestacionalJaime Andres Pardo RomeroNo ratings yet
- 2023 Anemia and Associated Factors Among Internally Displaced Children at Debark...Document21 pages2023 Anemia and Associated Factors Among Internally Displaced Children at Debark...Olga CîrsteaNo ratings yet
- Ndeezi2016 PDFDocument6 pagesNdeezi2016 PDFAnn Irene DomnicNo ratings yet
- Entamoeba HistolyticaDocument6 pagesEntamoeba HistolyticaWan Nur AnisaNo ratings yet
- Jurnal AnemiaDocument4 pagesJurnal AnemiaLaila RizqiyahNo ratings yet
- Zinc Deficiency in Children With Dengue Viral InfectionDocument5 pagesZinc Deficiency in Children With Dengue Viral InfectionSabariaNo ratings yet
- SAM Under 5Document6 pagesSAM Under 5BerhanuNo ratings yet
- Review On The Aflatoxins' Contamination of Foods and Public Health Effects Among Nigerian PopulationDocument17 pagesReview On The Aflatoxins' Contamination of Foods and Public Health Effects Among Nigerian PopulationUMYU Journal of Microbiology Research (UJMR)No ratings yet
- Prevalence HIVanemiaDocument8 pagesPrevalence HIVanemiatendaicrosbyNo ratings yet
- JournalDocument13 pagesJournalYasin HrNo ratings yet
- Prevalence of Hookworm Infection Among Patients Attending Aminu Kano Teaching Hospital Kano, NigeriaDocument3 pagesPrevalence of Hookworm Infection Among Patients Attending Aminu Kano Teaching Hospital Kano, NigeriaZulfan RifqiawanNo ratings yet
- Jurnal Diare 1Document6 pagesJurnal Diare 1andani delabeneNo ratings yet
- JPNC-10-00404Document7 pagesJPNC-10-00404Tomas YeheisNo ratings yet
- PGH 107 04 198Document4 pagesPGH 107 04 198shjahsjanshaNo ratings yet
- 2017 Article 71Document8 pages2017 Article 71Sahil DhamijaNo ratings yet
- Diagnostics 11 00794 v2Document11 pagesDiagnostics 11 00794 v2Adn crnNo ratings yet
- Prevalence and Determinants of Anaemia Among Children Aged 0-59 Months in A Rural Region of Armenia A Case-Control StudyDocument11 pagesPrevalence and Determinants of Anaemia Among Children Aged 0-59 Months in A Rural Region of Armenia A Case-Control StudyAsdfNo ratings yet
- RP-Case History of A Child With Sickle Cell Anemia in IndiaDocument5 pagesRP-Case History of A Child With Sickle Cell Anemia in IndiaMarie Kelsey Acena MacaraigNo ratings yet
- Kaposi SarcomaDocument14 pagesKaposi Sarcomaedgar mandengNo ratings yet
- Anemia InggrisDocument14 pagesAnemia InggrisNurul AwaliNo ratings yet
- Prevalence and Determinants of Anemia in Pregnancy, Sana'a, YemenDocument8 pagesPrevalence and Determinants of Anemia in Pregnancy, Sana'a, YemenIJPHSNo ratings yet
- Prevalence of Hookworm Infection Among Patients Attending Aminu Kano Teaching Hospital Kano, NigeriaDocument3 pagesPrevalence of Hookworm Infection Among Patients Attending Aminu Kano Teaching Hospital Kano, NigeriaMeenachi ChidambaramNo ratings yet
- IJP Volume 8 Issue 9 Pages 12011-12021Document11 pagesIJP Volume 8 Issue 9 Pages 12011-12021rullyNo ratings yet
- Jurnal SesDocument6 pagesJurnal SesItzar Chaidir IslamNo ratings yet
- Anemii PDF 008Document12 pagesAnemii PDF 008Ocha24 TupamahuNo ratings yet
- Impact of Malaria at The End of Pregnancy On Infant Mortality and MorbidityDocument9 pagesImpact of Malaria at The End of Pregnancy On Infant Mortality and MorbidityDebby Astasya AnnisaNo ratings yet
- International Journal of Infectious DiseasesDocument9 pagesInternational Journal of Infectious DiseasesHope ChrisNo ratings yet
- Cyber Security Awareness and Educational Outcomes of Grade 4 LearnersDocument33 pagesCyber Security Awareness and Educational Outcomes of Grade 4 LearnersInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Factors Influencing The Use of Improved Maize Seed and Participation in The Seed Demonstration Program by Smallholder Farmers in Kwali Area Council Abuja, NigeriaDocument6 pagesFactors Influencing The Use of Improved Maize Seed and Participation in The Seed Demonstration Program by Smallholder Farmers in Kwali Area Council Abuja, NigeriaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Parastomal Hernia: A Case Report, Repaired by Modified Laparascopic Sugarbaker TechniqueDocument2 pagesParastomal Hernia: A Case Report, Repaired by Modified Laparascopic Sugarbaker TechniqueInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Smart Health Care SystemDocument8 pagesSmart Health Care SystemInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Blockchain Based Decentralized ApplicationDocument7 pagesBlockchain Based Decentralized ApplicationInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Unmasking Phishing Threats Through Cutting-Edge Machine LearningDocument8 pagesUnmasking Phishing Threats Through Cutting-Edge Machine LearningInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Study Assessing Viability of Installing 20kw Solar Power For The Electrical & Electronic Engineering Department Rufus Giwa Polytechnic OwoDocument6 pagesStudy Assessing Viability of Installing 20kw Solar Power For The Electrical & Electronic Engineering Department Rufus Giwa Polytechnic OwoInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- An Industry That Capitalizes Off of Women's Insecurities?Document8 pagesAn Industry That Capitalizes Off of Women's Insecurities?International Journal of Innovative Science and Research TechnologyNo ratings yet
- Visual Water: An Integration of App and Web To Understand Chemical ElementsDocument5 pagesVisual Water: An Integration of App and Web To Understand Chemical ElementsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Insights Into Nipah Virus: A Review of Epidemiology, Pathogenesis, and Therapeutic AdvancesDocument8 pagesInsights Into Nipah Virus: A Review of Epidemiology, Pathogenesis, and Therapeutic AdvancesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Smart Cities: Boosting Economic Growth Through Innovation and EfficiencyDocument19 pagesSmart Cities: Boosting Economic Growth Through Innovation and EfficiencyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Parkinson's Detection Using Voice Features and Spiral DrawingsDocument5 pagesParkinson's Detection Using Voice Features and Spiral DrawingsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Impact of Silver Nanoparticles Infused in Blood in A Stenosed Artery Under The Effect of Magnetic Field Imp. of Silver Nano. Inf. in Blood in A Sten. Art. Under The Eff. of Mag. FieldDocument6 pagesImpact of Silver Nanoparticles Infused in Blood in A Stenosed Artery Under The Effect of Magnetic Field Imp. of Silver Nano. Inf. in Blood in A Sten. Art. Under The Eff. of Mag. FieldInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Compact and Wearable Ventilator System For Enhanced Patient CareDocument4 pagesCompact and Wearable Ventilator System For Enhanced Patient CareInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Air Quality Index Prediction Using Bi-LSTMDocument8 pagesAir Quality Index Prediction Using Bi-LSTMInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Predict The Heart Attack Possibilities Using Machine LearningDocument2 pagesPredict The Heart Attack Possibilities Using Machine LearningInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Investigating Factors Influencing Employee Absenteeism: A Case Study of Secondary Schools in MuscatDocument16 pagesInvestigating Factors Influencing Employee Absenteeism: A Case Study of Secondary Schools in MuscatInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Relationship Between Teacher Reflective Practice and Students Engagement in The Public Elementary SchoolDocument31 pagesThe Relationship Between Teacher Reflective Practice and Students Engagement in The Public Elementary SchoolInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Diabetic Retinopathy Stage Detection Using CNN and Inception V3Document9 pagesDiabetic Retinopathy Stage Detection Using CNN and Inception V3International Journal of Innovative Science and Research TechnologyNo ratings yet
- An Analysis On Mental Health Issues Among IndividualsDocument6 pagesAn Analysis On Mental Health Issues Among IndividualsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Implications of Adnexal Invasions in Primary Extramammary Paget's Disease: A Systematic ReviewDocument6 pagesImplications of Adnexal Invasions in Primary Extramammary Paget's Disease: A Systematic ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Harnessing Open Innovation For Translating Global Languages Into Indian LanuagesDocument7 pagesHarnessing Open Innovation For Translating Global Languages Into Indian LanuagesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Keywords:-Ibadhy Chooranam, Cataract, Kann Kasam,: Siddha Medicine, Kann NoigalDocument7 pagesKeywords:-Ibadhy Chooranam, Cataract, Kann Kasam,: Siddha Medicine, Kann NoigalInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Utilization of Date Palm (Phoenix Dactylifera) Leaf Fiber As A Main Component in Making An Improvised Water FilterDocument11 pagesThe Utilization of Date Palm (Phoenix Dactylifera) Leaf Fiber As A Main Component in Making An Improvised Water FilterInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Impact of Digital Marketing Dimensions On Customer SatisfactionDocument6 pagesThe Impact of Digital Marketing Dimensions On Customer SatisfactionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Dense Wavelength Division Multiplexing (DWDM) in IT Networks: A Leap Beyond Synchronous Digital Hierarchy (SDH)Document2 pagesDense Wavelength Division Multiplexing (DWDM) in IT Networks: A Leap Beyond Synchronous Digital Hierarchy (SDH)International Journal of Innovative Science and Research TechnologyNo ratings yet
- Advancing Healthcare Predictions: Harnessing Machine Learning For Accurate Health Index PrognosisDocument8 pagesAdvancing Healthcare Predictions: Harnessing Machine Learning For Accurate Health Index PrognosisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Making of Object Recognition Eyeglasses For The Visually Impaired Using Image AIDocument6 pagesThe Making of Object Recognition Eyeglasses For The Visually Impaired Using Image AIInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Formulation and Evaluation of Poly Herbal Body ScrubDocument6 pagesFormulation and Evaluation of Poly Herbal Body ScrubInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Terracing As An Old-Style Scheme of Soil Water Preservation in Djingliya-Mandara Mountains - CameroonDocument14 pagesTerracing As An Old-Style Scheme of Soil Water Preservation in Djingliya-Mandara Mountains - CameroonInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Diklat Rekam MedikDocument196 pagesDiklat Rekam MedikMulyono Aba AthiyaNo ratings yet
- ISHRS 20th Abstract Book 2012 Bahamas FinalDocument418 pagesISHRS 20th Abstract Book 2012 Bahamas FinalAlan J Bauman MDNo ratings yet
- MSG83 Epidural Analgesia in Labour PDFDocument18 pagesMSG83 Epidural Analgesia in Labour PDFGrigore PopaNo ratings yet
- The Great Influenza of 1918Document2 pagesThe Great Influenza of 1918Lois StanleyNo ratings yet
- 05-Pharmacy (4) - 2Document4 pages05-Pharmacy (4) - 2Amjid AfridiNo ratings yet
- Cancer of The PenisDocument6 pagesCancer of The PenisPaul CenabreNo ratings yet
- AP Biology Lab Spread of Epidemic Diseases: Through Viral TransmissionDocument5 pagesAP Biology Lab Spread of Epidemic Diseases: Through Viral Transmissionapi-319552725No ratings yet
- Albendazole-Related Loa Loa EncephalopathyDocument2 pagesAlbendazole-Related Loa Loa EncephalopathyLucchéri Ndong AkomezogheNo ratings yet
- A Decade of Dementia Care Training Learning Needs PDFDocument10 pagesA Decade of Dementia Care Training Learning Needs PDFYovana Pachón PovedaNo ratings yet
- English For Nursing 2: Vocational English Teacher's BookDocument15 pagesEnglish For Nursing 2: Vocational English Teacher's BookSelina Nguyễn VuNo ratings yet
- Dr. Usha - Manpower Planning New HospitalsDocument34 pagesDr. Usha - Manpower Planning New HospitalsVelram ShanmugamNo ratings yet
- Handbook of MS - 2012Document93 pagesHandbook of MS - 2012miliindianuNo ratings yet
- Delivery of TwinsDocument25 pagesDelivery of TwinsCakraEkkyNo ratings yet
- Pathogenic Escherichia Coli Associated With DiarrheaDocument7 pagesPathogenic Escherichia Coli Associated With DiarrheaSiti Fatimah RadNo ratings yet
- Jornal Materniti Blues-1Document10 pagesJornal Materniti Blues-1Izmi NasutionNo ratings yet
- Jurnal Antibiotik Resistensi Pada Kasus OMSKDocument10 pagesJurnal Antibiotik Resistensi Pada Kasus OMSKAnonymous a2nxIq5No ratings yet
- Drug-Study-Po (1) EwesdfdsfdsfsddsfdsfdsDocument14 pagesDrug-Study-Po (1) EwesdfdsfdsfsddsfdsfdsIbrahim RegachoNo ratings yet
- Neurotrauma GuidelineDocument16 pagesNeurotrauma GuidelineSanta ChrisNo ratings yet
- Flowchart - Mental Health Act Treatment OrderDocument1 pageFlowchart - Mental Health Act Treatment OrderEdwin100% (1)
- Study of Prevalence and Awareness Regarding Thyroid Disorders in People of Western Nepal at Zenus HospitalDocument9 pagesStudy of Prevalence and Awareness Regarding Thyroid Disorders in People of Western Nepal at Zenus HospitalIJAR JOURNALNo ratings yet
- Warren Barr South LoopDocument7 pagesWarren Barr South LoopBeth LawrenceNo ratings yet
- Treating The Post-LVAD Patient in An Acute Inpatient Rehab SettingDocument7 pagesTreating The Post-LVAD Patient in An Acute Inpatient Rehab Settingkori holubNo ratings yet
- Rotation Plan of 4 BatchesDocument8 pagesRotation Plan of 4 BatchesRaniNo ratings yet
- Ajit Vilas Borade0 - ReportDocument2 pagesAjit Vilas Borade0 - ReportRaj Singh RajputNo ratings yet
- Activity Design Mrsia 2018 Final BudgetDocument3 pagesActivity Design Mrsia 2018 Final BudgetRJay Mon MarcosNo ratings yet
- Physical Education - Ppt. Lesson 2Document24 pagesPhysical Education - Ppt. Lesson 2toni tesoro100% (1)
- Modified Braden Q ScaleDocument8 pagesModified Braden Q Scaleapi-122501165No ratings yet
- Diagnosis Dengue Melalui Deteksi Antibodi Imunoglobulin G Spesifik Dalam Sampel Urine Dengan Teknik ELISADocument8 pagesDiagnosis Dengue Melalui Deteksi Antibodi Imunoglobulin G Spesifik Dalam Sampel Urine Dengan Teknik ELISANOVI WULANDARINo ratings yet
- Goldburg2019 PDFDocument43 pagesGoldburg2019 PDFsandeep lal vNo ratings yet
- Abruptio PlacentaDocument11 pagesAbruptio PlacentaAlynna ValbuenaNo ratings yet