You might also like
- (LAPSUS) DemamDocument40 pages(LAPSUS) Demamratna sariNo ratings yet
- Management of Adult Patients With FeverDocument19 pagesManagement of Adult Patients With FeverMila AstariNo ratings yet
- Fever: EtiologyDocument7 pagesFever: EtiologyCzarina Mae JosonNo ratings yet
- TermoregulasiDocument22 pagesTermoregulasiAkhmad FatharoniNo ratings yet
- Fever v3Document82 pagesFever v3anil sahNo ratings yet
- Patient With Fever PDFDocument46 pagesPatient With Fever PDFNosheen hafeez100% (1)
- Fever, Chief Complaint, Clinical DiagnosisDocument57 pagesFever, Chief Complaint, Clinical DiagnosisAgung Tri LaksonoNo ratings yet
- Fever of Unknown OriginDocument33 pagesFever of Unknown OriginRanjit Kumar ShahNo ratings yet
- Altered Body Temperature: Presented By: Navjeet Kaur M.SC (NSG) 1 YRDocument68 pagesAltered Body Temperature: Presented By: Navjeet Kaur M.SC (NSG) 1 YRNithu NithuNo ratings yet
- Vital SignsDocument77 pagesVital SignschindabubaishakuNo ratings yet
- Endogenous Hyperthermia (Fever) &toxaemiaDocument9 pagesEndogenous Hyperthermia (Fever) &toxaemiazakaria hossainNo ratings yet
- Acute Febrile Illnesses: Solomon Bekele Sirak Melkeneh Sonia Worku Fri. May 15, 2014Document124 pagesAcute Febrile Illnesses: Solomon Bekele Sirak Melkeneh Sonia Worku Fri. May 15, 2014ashuNo ratings yet
- 4.2 - Fever-LsyDocument24 pages4.2 - Fever-Lsymirabel IvanaliNo ratings yet
- Clinical Manifestation of Bacterial and Viral InfectionDocument35 pagesClinical Manifestation of Bacterial and Viral InfectionSheryl ElitaNo ratings yet
- By DR Dimie OgoinaDocument35 pagesBy DR Dimie OgoinaIbrahim AkinbolaNo ratings yet
- Penatalaksanaan DemamDocument39 pagesPenatalaksanaan DemamClaraRotendownNo ratings yet
- DR D Ogoina Dept of Medicine Niger Delta UniversityDocument32 pagesDR D Ogoina Dept of Medicine Niger Delta UniversityPrincewill SeiyefaNo ratings yet
- Fever of Unknown OriginDocument26 pagesFever of Unknown OriginFiona Yona Sitali100% (1)
- FeverDocument12 pagesFeverSadr AkrmNo ratings yet
- Acute Febrile IllnessDocument23 pagesAcute Febrile IllnessSalih Anwar50% (2)
- Fev Mech PDFDocument7 pagesFev Mech PDFMitzu AlparisNo ratings yet
- Aproach To Patient With FeverDocument61 pagesAproach To Patient With Feverfatima fatima92% (12)
- Week 13 - Respiratory Disease, Continued.Document16 pagesWeek 13 - Respiratory Disease, Continued.shivani patelNo ratings yet
- DR - Debbie Latupeirissa, Spa Sub Divisi Infeksi Dan Penyakit Tropis SMF Kesehatan Anak Rsup FatmawatiDocument27 pagesDR - Debbie Latupeirissa, Spa Sub Divisi Infeksi Dan Penyakit Tropis SMF Kesehatan Anak Rsup FatmawatinikkennnNo ratings yet
- FebbreDocument17 pagesFebbreSolomon ElenaNo ratings yet
- Approach To The Febrile Patient: Dr.P.V.Balamurugan, M.D Senior Assistant Professor Dept. of Medicine GTMCH, TheniDocument85 pagesApproach To The Febrile Patient: Dr.P.V.Balamurugan, M.D Senior Assistant Professor Dept. of Medicine GTMCH, TheniAlp HatNo ratings yet
- Fever: Department of Pathological Physiology - 2018Document28 pagesFever: Department of Pathological Physiology - 2018meriem bouzidaniNo ratings yet
- Approach To FeverDocument80 pagesApproach To FeverRaditia AbrahamNo ratings yet
- Approach To The Febrile PatientsDocument50 pagesApproach To The Febrile PatientsAboubakar Moalim Mahad moh'dNo ratings yet
- FeverDocument39 pagesFeverKartika FitriNo ratings yet
- Alteration in Body TemperatureDocument19 pagesAlteration in Body Temperaturepravina praviNo ratings yet
- AFI Lecture UGDocument55 pagesAFI Lecture UGashuNo ratings yet
- Demam 3Document53 pagesDemam 3dulen dulenNo ratings yet
- DEMAM Pada Bayi Dan Anak UmyDocument40 pagesDEMAM Pada Bayi Dan Anak UmyFarika NorNo ratings yet
- FEVERDocument41 pagesFEVERNawaf AlrwuiliNo ratings yet
- Fever in The ICU AADocument50 pagesFever in The ICU AAabciximabNo ratings yet
- Fever Sepsis SyokDocument40 pagesFever Sepsis SyoknawriirwanNo ratings yet
- FEVER - FUO - RASH Into To Medicine - First YearDocument93 pagesFEVER - FUO - RASH Into To Medicine - First YearJoseph De JoyaNo ratings yet
- FeverDocument14 pagesFeverAhlam AliNo ratings yet
- K17. Parasit Yang Menyebabkan Infeksi OtakDocument71 pagesK17. Parasit Yang Menyebabkan Infeksi OtakSarahGustiaWoromboniNo ratings yet
- Fever in Children and FUODocument61 pagesFever in Children and FUOaldiansyahraufNo ratings yet
- Fever: Pathogenesis and TreatmentDocument31 pagesFever: Pathogenesis and TreatmentMin-Joo Esther ParkNo ratings yet
- I.M. Harry Series by Deeetch2021 Chapter 15: Fever: HyperpyrexiaDocument5 pagesI.M. Harry Series by Deeetch2021 Chapter 15: Fever: HyperpyrexiaDon Hale HilarioNo ratings yet
- Evaluation of The Febrile Patient A Case-Based Approach: Fevers and Fevers of Unknown OriginDocument97 pagesEvaluation of The Febrile Patient A Case-Based Approach: Fevers and Fevers of Unknown Originkrish vjNo ratings yet
- 9 Afi HDocument116 pages9 Afi HRuth DanielNo ratings yet
- Infection: Dr. Mehrunnisa Umar Assistant Professor Department of MedicineDocument57 pagesInfection: Dr. Mehrunnisa Umar Assistant Professor Department of MedicinedrusmanjamilhcmdNo ratings yet
- Prolonged FeverDocument45 pagesProlonged FeverAnastasiafynnNo ratings yet
- Hypothermia in Ill DogsDocument13 pagesHypothermia in Ill DogsdeisyNo ratings yet
- Harbakhash Singh Sandhar Textbook of Pathology: Reading ExcerptDocument6 pagesHarbakhash Singh Sandhar Textbook of Pathology: Reading ExcerptDwi Puja SetiawanNo ratings yet
- Fever in Children and FUODocument62 pagesFever in Children and FUOAmbartyas Niken WNo ratings yet
- Rheumatic Fever SymposiumDocument52 pagesRheumatic Fever SymposiumNamratha MedaNo ratings yet
- l07 - Fever & FuoDocument27 pagesl07 - Fever & FuoS sNo ratings yet
- Pathophysiology of Fever-Tropmed2013Document24 pagesPathophysiology of Fever-Tropmed2013Yessy Dwi Oktavia100% (1)
- Approach To Febrile PatientDocument79 pagesApproach To Febrile Patientadaneyihune100% (5)
- Prolong FeverDocument12 pagesProlong FeverNugroho prasetyoNo ratings yet
- Thermoregulation HANANDocument25 pagesThermoregulation HANANEsraa AltawaraNo ratings yet
- The Healing Power of Fever: Your Body's Natural Defense against DiseaseFrom EverandThe Healing Power of Fever: Your Body's Natural Defense against DiseaseNo ratings yet
- Special Operations Forces Medical HandbookFrom EverandSpecial Operations Forces Medical HandbookRating: 4.5 out of 5 stars4.5/5 (2)
- Cases 4,5, 6 InonDocument5 pagesCases 4,5, 6 InonMalika SadridinovaNo ratings yet
- Leukemias: The Development of LeukemiaDocument66 pagesLeukemias: The Development of LeukemiaMalika SadridinovaNo ratings yet
- Disorders of Intestinal AbsorptionDocument83 pagesDisorders of Intestinal AbsorptionMalika SadridinovaNo ratings yet
- Vitamin KDocument25 pagesVitamin KMalika SadridinovaNo ratings yet
- Dehydration 'Acid Base Balance DisordersDocument38 pagesDehydration 'Acid Base Balance DisordersMalika SadridinovaNo ratings yet
- CasesDocument4 pagesCasesMalika SadridinovaNo ratings yet
- Acid Base Disturbances - 2Document31 pagesAcid Base Disturbances - 2Malika SadridinovaNo ratings yet
- Disseminated Intravascular Coagulation (DIC)Document33 pagesDisseminated Intravascular Coagulation (DIC)Malika SadridinovaNo ratings yet
- HemophiliaDocument34 pagesHemophiliaMalika SadridinovaNo ratings yet
- Are Mobile Phones Essential or DangerousDocument3 pagesAre Mobile Phones Essential or DangerousMalika SadridinovaNo ratings yet
- Spare The Rod Spoil The ChildDocument1 pageSpare The Rod Spoil The ChildMalika SadridinovaNo ratings yet
- A Literary Analysis of The Lottery by Shirley JacksonDocument3 pagesA Literary Analysis of The Lottery by Shirley JacksonMalika SadridinovaNo ratings yet
- Child AbuseDocument3 pagesChild AbuseMalika SadridinovaNo ratings yet
- Loneliness in of Mice and MenDocument4 pagesLoneliness in of Mice and MenMalika SadridinovaNo ratings yet
- Anti Abortion EssayDocument2 pagesAnti Abortion EssayMalika SadridinovaNo ratings yet
- What Can Be Done To Help Save The EarthDocument2 pagesWhat Can Be Done To Help Save The EarthMix XimNo ratings yet
- Apple Ipod Marketing PlanDocument8 pagesApple Ipod Marketing PlanMalika SadridinovaNo ratings yet
- A Persuasive Speech Against Underage DrinkingDocument3 pagesA Persuasive Speech Against Underage DrinkingMalika SadridinovaNo ratings yet
- Why Smoking Is Bad For EveryoneDocument1 pageWhy Smoking Is Bad For EveryoneMalika SadridinovaNo ratings yet
- Advantages and Disadvantages of Hstorical Cost AccountingDocument3 pagesAdvantages and Disadvantages of Hstorical Cost AccountingMalika SadridinovaNo ratings yet
- The American DreamDocument1 pageThe American DreamMalika SadridinovaNo ratings yet
- Causes of The French Revolution of 1789Document2 pagesCauses of The French Revolution of 1789Malika SadridinovaNo ratings yet
- A Persuasive Speech Against Underage DrinkingDocument3 pagesA Persuasive Speech Against Underage DrinkingMalika SadridinovaNo ratings yet
- Animal Testing Pros and ConsDocument6 pagesAnimal Testing Pros and ConsMalika SadridinovaNo ratings yet
- Importance of EducationDocument1 pageImportance of EducationMalika SadridinovaNo ratings yet
- Importance of EducationDocument1 pageImportance of EducationMalika SadridinovaNo ratings yet
- Peds 2015-3501 Full PDFDocument19 pagesPeds 2015-3501 Full PDFJehan VahlepyNo ratings yet
- Vomiting in ChildrenDocument3 pagesVomiting in Childrenartz_dhanaNo ratings yet
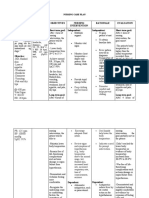
- NCP For Parent and Child PDFDocument3 pagesNCP For Parent and Child PDFMariana Mikaela AlagarNo ratings yet
- Fundamentals of Nursing Gladys Bautista Jaime 2010Document10 pagesFundamentals of Nursing Gladys Bautista Jaime 2010Clarissa GuifayaNo ratings yet
- HyperthermiaDocument3 pagesHyperthermiaKatrina Yvet BacomoNo ratings yet
- Impaired Verbal CommunicationDocument6 pagesImpaired Verbal CommunicationLaura Sansonetti100% (1)
- Pneumonia Nursing Care Plans - 10 Nursing Diagnosis - NurseslabsDocument34 pagesPneumonia Nursing Care Plans - 10 Nursing Diagnosis - NurseslabsMenard Velasco100% (1)
- PDFDocument7 pagesPDFayuNo ratings yet
- °F Normal Body Temperature Ranges: 0 - 2 Years 3 - 10 Years 11 - 65 Years 65 YearsDocument2 pages°F Normal Body Temperature Ranges: 0 - 2 Years 3 - 10 Years 11 - 65 Years 65 YearsGershon Bolaños BernalNo ratings yet
- Case Presentation 2Document11 pagesCase Presentation 2Angel Jonele ManongsongNo ratings yet
- DR Stuart Crisp DR Per Grinsted: Written byDocument8 pagesDR Stuart Crisp DR Per Grinsted: Written byRizky MarethaNo ratings yet
- Pediatrics Exam QuestionsDocument3 pagesPediatrics Exam QuestionsHUSSAM22100% (2)
- 7th Floor, Iloilo City Hall Building, Plaza Libertad, Iloilo City 5000Document18 pages7th Floor, Iloilo City Hall Building, Plaza Libertad, Iloilo City 5000Jeremae VentarNo ratings yet
- Evaluation of Efficacy and Safety of Fixed Dose Combination of Cefixime and Ofloxacin PDFDocument8 pagesEvaluation of Efficacy and Safety of Fixed Dose Combination of Cefixime and Ofloxacin PDFAlyn Paul EmnacenNo ratings yet
- Effectiveness of Tepid Sponge Compresses and Plaster Compresses On Children'S Fever Temperature TyphoidDocument11 pagesEffectiveness of Tepid Sponge Compresses and Plaster Compresses On Children'S Fever Temperature TyphoidAyasNo ratings yet
- Dengue Fever Fact SheetDocument1 pageDengue Fever Fact Sheetiamketul6340No ratings yet
- CASESDocument24 pagesCASESMuhammed FirozNo ratings yet
- Describe The Four Main Symptoms of ImciDocument2 pagesDescribe The Four Main Symptoms of ImciMartha JulyNo ratings yet
- Everybody S Guide To Homeopathic Medicines Stephen Cummings Dana Ullman.07301 - 2influenza PDFDocument14 pagesEverybody S Guide To Homeopathic Medicines Stephen Cummings Dana Ullman.07301 - 2influenza PDFKuldeep KoulNo ratings yet
- Covid LeukemiaDocument9 pagesCovid LeukemiamahadianismailnstNo ratings yet
- د حامد عطية الباطنه-1Document674 pagesد حامد عطية الباطنه-1josed100% (1)
- Dehydration: By: M. SofyanDocument2 pagesDehydration: By: M. Sofyansofyan novrizalNo ratings yet
- 5 Benign Febrile Convulsions Nursing Care PlansDocument19 pages5 Benign Febrile Convulsions Nursing Care PlansRoanna Alyssa Sy Jimenez75% (4)
- Republic of The Philippines University Town, Northern Samar Web: EmailDocument5 pagesRepublic of The Philippines University Town, Northern Samar Web: EmailJane MinNo ratings yet
- Rheumatic Fever Small Group DiscussionDocument13 pagesRheumatic Fever Small Group DiscussionLyca Mae AurelioNo ratings yet
- Materia Medica - by N. M. ChoudhuryDocument849 pagesMateria Medica - by N. M. ChoudhuryDean WinchesterNo ratings yet
- Fever: Clinical DescriptionDocument6 pagesFever: Clinical DescriptionNama ManaNo ratings yet
- Guideline For Case ManagementDocument78 pagesGuideline For Case ManagementkukadiyaNo ratings yet
- Chikungunya Virus DiseaseDocument25 pagesChikungunya Virus DiseasemamaluNo ratings yet
- Paracetamol EnglishDocument16 pagesParacetamol EnglishAjitabh YadavNo ratings yet