You might also like
- Auto-Inflammatory Syndromes: Pathophysiology, Diagnosis, and ManagementFrom EverandAuto-Inflammatory Syndromes: Pathophysiology, Diagnosis, and ManagementPetros EfthimiouNo ratings yet
- Applied Genomics: Data Mining Reveals Species-Specific Malaria Diagnostic Targets More Sensitive Than 18S rRNADocument8 pagesApplied Genomics: Data Mining Reveals Species-Specific Malaria Diagnostic Targets More Sensitive Than 18S rRNAApplied molecular biotechnologyNo ratings yet
- Anti-Msp-10 Igg Indicates Recent Exposure To Plasmodium Vivax Infection in The Peruvian AmazonDocument16 pagesAnti-Msp-10 Igg Indicates Recent Exposure To Plasmodium Vivax Infection in The Peruvian AmazonEdgar Huerta CardenasNo ratings yet
- Multiplex Real-Time PCR Detection of P FalciparumDocument7 pagesMultiplex Real-Time PCR Detection of P FalciparumAlemayehu Letebo AlbejoNo ratings yet
- Accepted ManuscriptDocument7 pagesAccepted ManuscriptNaomiNo ratings yet
- Ultrasensitive CRISPR-based Diagnostic For Field-Applicable Detection of Plasmodium Species in Symptomatic and Asymptomatic MalariaDocument10 pagesUltrasensitive CRISPR-based Diagnostic For Field-Applicable Detection of Plasmodium Species in Symptomatic and Asymptomatic MalariaMilena MurilloNo ratings yet
- 3-Article Text-9-1-10-20190830Document4 pages3-Article Text-9-1-10-20190830Richard SalvatoNo ratings yet
- Field Evaluation of The ICT Malaria P.F Immunochromatographic Test For Detection of Plasmodium FalciparumDocument6 pagesField Evaluation of The ICT Malaria P.F Immunochromatographic Test For Detection of Plasmodium FalciparumPace RaditNo ratings yet
- Whole Genome Analysis of Extensively Drug Resistant Mycobacterium Tuberculosis Strains in PeruDocument13 pagesWhole Genome Analysis of Extensively Drug Resistant Mycobacterium Tuberculosis Strains in PeruCarlos AscNo ratings yet
- Research Article Plasmodium FalciparumDocument5 pagesResearch Article Plasmodium FalciparumIsmail IkhsanNo ratings yet
- Comparative Analysis Diff Malaria ParasiteDocument7 pagesComparative Analysis Diff Malaria ParasiteMichaelNo ratings yet
- Malaria Paper 2 MANGOLDDocument6 pagesMalaria Paper 2 MANGOLDfajardianhNo ratings yet
- The Lancet MalariaDocument18 pagesThe Lancet MalariaRodrigo PazNo ratings yet
- Binax 28Document4 pagesBinax 28pieterinpretoria391No ratings yet
- Type: Electronic/Moderated Poster PresentationDocument1 pageType: Electronic/Moderated Poster PresentationvhatmaNo ratings yet
- Treatment of Malaria in The United StatesDocument14 pagesTreatment of Malaria in The United StatesmeinytonyNo ratings yet
- Article Monkeypox GeneXpert 2Document6 pagesArticle Monkeypox GeneXpert 2jalal.nourlil13No ratings yet
- Ashley2018 Lancet - MALARIA PDFDocument14 pagesAshley2018 Lancet - MALARIA PDFAngel Orlando LanderNo ratings yet
- Malaria FalciparumDocument6 pagesMalaria FalciparumAnonymous G20oAbl6p8No ratings yet
- Random Distribution of Mixed Species Malaria Infections in Papua New GuineaDocument7 pagesRandom Distribution of Mixed Species Malaria Infections in Papua New GuineaAwliyana Risla PutriNo ratings yet
- MosquitoDocument3 pagesMosquitoVanessaAngNo ratings yet
- 929Document7 pages929Hijrawati IrhaeNo ratings yet
- Epidemiology of Plasmodium Infections in Flores Island, Indonesia Using Real-Time PCRDocument9 pagesEpidemiology of Plasmodium Infections in Flores Island, Indonesia Using Real-Time PCRTeuku M Arief YaminNo ratings yet
- Zoo 1Document3 pagesZoo 1nurul rezki fitrianiazisNo ratings yet
- Next Generation Sequencing of Microbial Cell Free DNA To Rapidly Detect Fluoribacter Bozemanae Pneumonia in An Immunocompromised HostDocument4 pagesNext Generation Sequencing of Microbial Cell Free DNA To Rapidly Detect Fluoribacter Bozemanae Pneumonia in An Immunocompromised HostAthenaeum Scientific PublishersNo ratings yet
- Poster Abstracts - OFID 2019:6 (Suppl 2) - S297Document1 pagePoster Abstracts - OFID 2019:6 (Suppl 2) - S297ELIONo ratings yet
- Rapid Antigen Detection Tests and Possible Implications For Self-Diagnostic Use 2003 s1477-8939 (03) 00037-1Document4 pagesRapid Antigen Detection Tests and Possible Implications For Self-Diagnostic Use 2003 s1477-8939 (03) 00037-1Radit YaNo ratings yet
- Clinical Microbiology and InfectionDocument20 pagesClinical Microbiology and InfectionArthur SchulzNo ratings yet
- Evaluation of Antibiotic Susceptibilities of Ehrlichia Canis, Ehrlichia Chaffeensis, and Anaplasma Phagocytophilum by Real-Time PCRDocument7 pagesEvaluation of Antibiotic Susceptibilities of Ehrlichia Canis, Ehrlichia Chaffeensis, and Anaplasma Phagocytophilum by Real-Time PCRyudhi arjentiniaNo ratings yet
- Scorpion Envenomation and Serotherapy inDocument7 pagesScorpion Envenomation and Serotherapy inrijal fahrijalNo ratings yet
- Barazorda 2021Document15 pagesBarazorda 2021Steve Vladimir Acedo LazoNo ratings yet
- 2017 Article 2875Document7 pages2017 Article 2875IFan Erian KurniawanNo ratings yet
- Legionnaires' Disease Seminar ReviewDocument10 pagesLegionnaires' Disease Seminar Reviewcrowned-lionNo ratings yet
- Antigen-Stimulated PBMC Transcriptional Protective Signatures For Malaria ImmunizationDocument18 pagesAntigen-Stimulated PBMC Transcriptional Protective Signatures For Malaria Immunizationyowan wandikboNo ratings yet
- Nonimaging Diagnostic Tests For Pneumonia: Anupama Gupta Brixey,, Raju Reddy,, Shewit P. GiovanniDocument14 pagesNonimaging Diagnostic Tests For Pneumonia: Anupama Gupta Brixey,, Raju Reddy,, Shewit P. GiovannikaeranNo ratings yet
- 2014 Boletin Epidemiologico Semana 24Document8 pages2014 Boletin Epidemiologico Semana 24alejandro nietoNo ratings yet
- TB JournalDocument1 pageTB JournalJudy Anne PatricioNo ratings yet
- 9670-Article Text-51322-1-10-20090205Document6 pages9670-Article Text-51322-1-10-20090205Ashraf AlbhlaNo ratings yet
- Watch out for surgery risk of KPC-producing K. pneumoniaeDocument7 pagesWatch out for surgery risk of KPC-producing K. pneumoniaeFurqanRidhaNo ratings yet
- Seminar: Elizabeth A Ashley, Aung Pyae Phyo, Charles J WoodrowDocument14 pagesSeminar: Elizabeth A Ashley, Aung Pyae Phyo, Charles J WoodrowMr. LNo ratings yet
- Artigo C Neoformans PDFDocument29 pagesArtigo C Neoformans PDFJorge Luis CarmoNo ratings yet
- Anti 21 Malaria Drug Discovery PDFDocument21 pagesAnti 21 Malaria Drug Discovery PDFTetteh JudeNo ratings yet
- Paper Primers MycoplasmaTSWJ2014-549858Document6 pagesPaper Primers MycoplasmaTSWJ2014-549858andrea nettle bareaNo ratings yet
- Seminario 6 Inmunologia Clinica 2023-IIDocument15 pagesSeminario 6 Inmunologia Clinica 2023-IImiguel angel ascoy saucedoNo ratings yet
- Artículo 2 - The Diagnostic Performance of Classical Molecular Tests Used For Detecting Human PapillomavirusDocument7 pagesArtículo 2 - The Diagnostic Performance of Classical Molecular Tests Used For Detecting Human PapillomavirusAnthony McIvorNo ratings yet
- Prevalence of Malaria Infection in Some Localities of Fayoum GovernorateDocument92 pagesPrevalence of Malaria Infection in Some Localities of Fayoum GovernorateAlcaponi Orlando FuoriosoNo ratings yet
- HRP-2 Deletion - A Hole in The Ship of Malaria EliminationDocument2 pagesHRP-2 Deletion - A Hole in The Ship of Malaria EliminationAnil VermaNo ratings yet
- PCR - HPVDocument6 pagesPCR - HPVmelissaraujo.16No ratings yet
- Microorganisms 07 00179 With CoverDocument18 pagesMicroorganisms 07 00179 With CoverBenga TokanneNo ratings yet
- Urealyticum and Mycoplasma Hominis: Sexually-Transmitted Infections in UreaplasmaDocument4 pagesUrealyticum and Mycoplasma Hominis: Sexually-Transmitted Infections in UreaplasmaPaula Daniela Martinez ChavezNo ratings yet
- 3.09.11 Nonhuman PrimatesDocument6 pages3.09.11 Nonhuman PrimatesKìkøu KìkãmNo ratings yet
- Krettli2009 PDFDocument10 pagesKrettli2009 PDFAnisah MahardianiNo ratings yet
- Witkowski, Duru - Et - Al, Lancet ID - 2016Document39 pagesWitkowski, Duru - Et - Al, Lancet ID - 2016sylvi293No ratings yet
- Journal Pone 0249708Document11 pagesJournal Pone 0249708Tewfic SeidNo ratings yet
- Update On MalariaDocument8 pagesUpdate On MalariaVivi DeviyanaNo ratings yet
- Diagnostico de MalariaDocument9 pagesDiagnostico de MalariaLaura ReyesNo ratings yet
- Plasmodium Malariae The Persisting MysteriesDocument13 pagesPlasmodium Malariae The Persisting Mysteriesgerges8723No ratings yet
- 03 (2022) Targeting A Highly Repetitive Genomic Sequence??Document14 pages03 (2022) Targeting A Highly Repetitive Genomic Sequence??juliabatis04No ratings yet
- Encyclopedia of Infectious Diseases: Modern MethodologiesFrom EverandEncyclopedia of Infectious Diseases: Modern MethodologiesMichel TibayrencNo ratings yet
- CL 10 Sci Heredity Unit PaperDocument2 pagesCL 10 Sci Heredity Unit Paperdeep_72No ratings yet
- The Antibacterial and Antifungal Activity of Essential Oil Derived From The Flesh of Nutmeg Fruit 6155Document6 pagesThe Antibacterial and Antifungal Activity of Essential Oil Derived From The Flesh of Nutmeg Fruit 6155Zyuha AiniiNo ratings yet
- Personal Development (Practice Test)Document4 pagesPersonal Development (Practice Test)Sonny B. Nabaza100% (3)
- EECP IabpDocument16 pagesEECP IabpMythily VedhagiriNo ratings yet
- Đề Thi Hsg Tiếng Anh Vĩnh Phúc (Lớp 12)Document8 pagesĐề Thi Hsg Tiếng Anh Vĩnh Phúc (Lớp 12)Cù Minh HiếuNo ratings yet
- Algorithms For The Design of A Multi-Stage Adaptive Kanban SystemDocument33 pagesAlgorithms For The Design of A Multi-Stage Adaptive Kanban SystemKharisma ElanNo ratings yet
- Notice: Environmental Statements Notice of Intent: U. S. Navy Surveillance Towed Array Sensor System Low Frequency Active Sonar OperationsDocument2 pagesNotice: Environmental Statements Notice of Intent: U. S. Navy Surveillance Towed Array Sensor System Low Frequency Active Sonar OperationsJustia.comNo ratings yet
- Activity 8 MycologyDocument3 pagesActivity 8 MycologyBrent Lee100% (1)
- Chemical Analysis of MANOIR XM AlloyDocument3 pagesChemical Analysis of MANOIR XM Alloyogun tokucNo ratings yet
- Bio 10th - Excretion - Extensive TestDocument1 pageBio 10th - Excretion - Extensive TestDharmendra SinghNo ratings yet
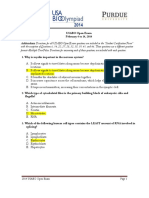
- USABO 14 Open Exam Final AnsDocument16 pagesUSABO 14 Open Exam Final AnsGuest SuiteNo ratings yet
- EX-CELL® EBx® PRO-II Serum-Free Medium Without L-GlutamineDocument2 pagesEX-CELL® EBx® PRO-II Serum-Free Medium Without L-GlutamineSAFC-Global100% (1)
- Perceived Stress ScaleDocument6 pagesPerceived Stress ScalevieffejonesNo ratings yet
- Test Bank For Understanding Pathophysiology 6th Edition by HuetherDocument24 pagesTest Bank For Understanding Pathophysiology 6th Edition by HuetherJulieCooperb25om100% (33)
- Soft Computing Unit-2Document61 pagesSoft Computing Unit-2namak sung loNo ratings yet
- Primal Healing - Access The Incredible Power of Feelings To Improve Your Health (PDFDrive)Document510 pagesPrimal Healing - Access The Incredible Power of Feelings To Improve Your Health (PDFDrive)Adriana Rosa100% (2)
- Exploring Life Through Science, Third Edition: Learning Progression ChartDocument10 pagesExploring Life Through Science, Third Edition: Learning Progression ChartKris GiaNo ratings yet
- The Five Major Brances of Chemistry and Their Sub-BranchesDocument3 pagesThe Five Major Brances of Chemistry and Their Sub-BranchesYenna Rezano LumbaNo ratings yet
- Biochemistry of InfertilityDocument6 pagesBiochemistry of InfertilityDianaNo ratings yet
- 09 10716 Perkembangan Larva Oryzias Javanicus Sebagai Kandidat Biota Formatedfinal2Document9 pages09 10716 Perkembangan Larva Oryzias Javanicus Sebagai Kandidat Biota Formatedfinal2Al- RezimNo ratings yet
- Complete Urinalysis Clinical MicrosDocument85 pagesComplete Urinalysis Clinical MicrosJoshua Elbanbuena100% (1)
- 1 s2.0 S1871678419304418 MainDocument9 pages1 s2.0 S1871678419304418 MainGurpreet SinghNo ratings yet
- Breathwork Basics EbookDocument11 pagesBreathwork Basics EbookBakulBadwalNo ratings yet
- MLTG Competency ProfileDocument18 pagesMLTG Competency ProfileJessie TNo ratings yet
- Biochem Exam Practice QuestionsDocument12 pagesBiochem Exam Practice Questionsihack_101No ratings yet
- Upstream & DownstreamDocument20 pagesUpstream & DownstreamLamtiarma PanjaitanNo ratings yet
- Anatomy and Physiology of Farm Animals GuideDocument51 pagesAnatomy and Physiology of Farm Animals Guidealexenneth canilaNo ratings yet
- Theory of Successful Aging (Flood)Document4 pagesTheory of Successful Aging (Flood)Chinnie Nicole RamosNo ratings yet
- Wilson, D.S., Hayes, S.C. & Biglan, A. (2018). Evolution and contextual behavioral science an integrated framework for understanding, predicting and influencing human behavior. Oakland Context Press..pdfDocument390 pagesWilson, D.S., Hayes, S.C. & Biglan, A. (2018). Evolution and contextual behavioral science an integrated framework for understanding, predicting and influencing human behavior. Oakland Context Press..pdfjesus100% (3)
- 06 Chapter 2Document40 pages06 Chapter 2Murali ShiramdasNo ratings yet