You might also like
- Children at Risk - An Evaluation of Factors Contributing To Child Abuse and NeglectDocument318 pagesChildren at Risk - An Evaluation of Factors Contributing To Child Abuse and NeglectAlguémNo ratings yet
- The Addicted Child: A Parent's Guide to Adolescent Substance AbuseFrom EverandThe Addicted Child: A Parent's Guide to Adolescent Substance AbuseNo ratings yet
- Sro Report Finalv2Document42 pagesSro Report Finalv2NEWS CENTER MaineNo ratings yet
- Psychiatric Diagnosis: Challenges and ProspectsFrom EverandPsychiatric Diagnosis: Challenges and ProspectsIhsan M. SalloumRating: 5 out of 5 stars5/5 (1)
- Rhetorical Analysis The C Word in The Hallways Taylor KoontzDocument2 pagesRhetorical Analysis The C Word in The Hallways Taylor Koontzapi-26773884750% (2)
- Summary of Andrew J. Wakefield's Waging War On The Autistic ChildFrom EverandSummary of Andrew J. Wakefield's Waging War On The Autistic ChildNo ratings yet
- Assessing and Treating Serious Juvenile OffendersDocument8 pagesAssessing and Treating Serious Juvenile OffendersDesmond HumeNo ratings yet
- Cognitive and Behavioral Interventions in the Schools: Integrating Theory and Research into PracticeFrom EverandCognitive and Behavioral Interventions in the Schools: Integrating Theory and Research into PracticeRosemary FlanaganNo ratings yet
- Ending The Commerical Sexual Expolitation of Children: A Call For Multi-System Collaboration in CaliforniaDocument100 pagesEnding The Commerical Sexual Expolitation of Children: A Call For Multi-System Collaboration in CaliforniaMarsh Law Firm PLLCNo ratings yet
- C4D VAC Systematic Review ReportDocument79 pagesC4D VAC Systematic Review ReportsofiabloemNo ratings yet
- Teenage Health Concerns: How Parents Can Manage Eating Disorders In Teenage ChildrenFrom EverandTeenage Health Concerns: How Parents Can Manage Eating Disorders In Teenage ChildrenNo ratings yet
- Categories of High Needs StudentsDocument3 pagesCategories of High Needs Studentsapi-338157510No ratings yet
- Integrative Dual Diagnosis Treatment Approach to an Individual with Alcoholism and Coexisting Endogenous DepressionFrom EverandIntegrative Dual Diagnosis Treatment Approach to an Individual with Alcoholism and Coexisting Endogenous DepressionRating: 2 out of 5 stars2/5 (1)
- CDC Connectiveness BookletDocument24 pagesCDC Connectiveness BookletDominique Harmon100% (1)
- Improving the Quality of Child Custody Evaluations: A Systematic ModelFrom EverandImproving the Quality of Child Custody Evaluations: A Systematic ModelNo ratings yet
- Child on Child Sexual Abuse Literature ReviewDocument30 pagesChild on Child Sexual Abuse Literature ReviewGino MaccioNo ratings yet
- Bullying and Self-Exclusion: Who Cares?: Roundtable ReportDocument26 pagesBullying and Self-Exclusion: Who Cares?: Roundtable ReportAlex PavelNo ratings yet
- Emotional Child AbuseDocument3 pagesEmotional Child Abuseredz00No ratings yet
- Disorders RushedDocument40 pagesDisorders Rushedapi-391411195No ratings yet
- Growth and Development: Yarsi School of MedicineDocument32 pagesGrowth and Development: Yarsi School of MedicineLia Noor AnggrainiNo ratings yet
- 04 EmotionalDocument2 pages04 EmotionalSandra Barnett CrossanNo ratings yet
- What Is Manipulative Behavior AnywayDocument18 pagesWhat Is Manipulative Behavior AnywayMichael BurgessNo ratings yet
- Behavioral Treatment and Normal Educational and Intellectual Functioning in /bung Autistic ChildrenDocument7 pagesBehavioral Treatment and Normal Educational and Intellectual Functioning in /bung Autistic ChildrenMariaNo ratings yet
- Psychopathy and Human Evil: An OverviewDocument25 pagesPsychopathy and Human Evil: An OverviewCristina MirceanNo ratings yet
- Screening Youth For Suicide Risk in MediDocument6 pagesScreening Youth For Suicide Risk in MediPánico FaunoNo ratings yet
- Clinical Assessment and Management of Child and Adolescent Psychiatric EmergenciesDocument39 pagesClinical Assessment and Management of Child and Adolescent Psychiatric EmergenciesRyan Lazatin100% (1)
- M-CHAT Scoring Key: Does Your Child Take An Interest in Other Children?Document1 pageM-CHAT Scoring Key: Does Your Child Take An Interest in Other Children?bramafixsNo ratings yet
- A Preliminary Report On The Police Foundation's Averted School Violence DatabaseDocument40 pagesA Preliminary Report On The Police Foundation's Averted School Violence Databaseepraetorian100% (1)
- Smartphone Use, Addiction, Narcissism, and Personality: A Mixed Methods InvestigationDocument20 pagesSmartphone Use, Addiction, Narcissism, and Personality: A Mixed Methods InvestigationDerek E. BairdNo ratings yet
- ICD-10 F60-62 Personality Disorders - F62.0 Chronic PTSDDocument8 pagesICD-10 F60-62 Personality Disorders - F62.0 Chronic PTSDDavid A CohenNo ratings yet
- BullyingDocument9 pagesBullyingGreer LevendalNo ratings yet
- Why Do LGBTQ Youths in America Feel The Need To Hide 1Document13 pagesWhy Do LGBTQ Youths in America Feel The Need To Hide 1api-609315513No ratings yet
- Ending Violence in Schools An Investment CaseDocument88 pagesEnding Violence in Schools An Investment CasesofiabloemNo ratings yet
- Family AbuseDocument31 pagesFamily Abuseapi-369534649No ratings yet
- DSM 5 and Child Psychiatric DisordersDocument5 pagesDSM 5 and Child Psychiatric Disordersfotinimavr94No ratings yet
- 2021-Editorial - Defining The Clinical Boundary of Disruptive Mood Dysregulation Disorder Symptoms in YouthDocument3 pages2021-Editorial - Defining The Clinical Boundary of Disruptive Mood Dysregulation Disorder Symptoms in YouthCaio MayrinkNo ratings yet
- Final Evidence TableDocument21 pagesFinal Evidence Tableapi-293253519No ratings yet
- Clincial Paper - PsychDocument12 pagesClincial Paper - Psychapi-651130562100% (1)
- No Excuse For Abuse in The FamilyDocument3 pagesNo Excuse For Abuse in The FamilyKazeem Owoyemi100% (1)
- Cognitive Schemas and Sexual Offending - Differences Between Rapists, Pedophilic and Nonpedophilic Child Molesters, and Nonsexual OffendersDocument12 pagesCognitive Schemas and Sexual Offending - Differences Between Rapists, Pedophilic and Nonpedophilic Child Molesters, and Nonsexual OffendersFrancois BlanchetteNo ratings yet
- Autism 206 AymakelidesDocument44 pagesAutism 206 AymakelidesȘtefana StefiNo ratings yet
- Risk Factors, Diagnosis, Prognosis and Treatment of AutismDocument36 pagesRisk Factors, Diagnosis, Prognosis and Treatment of AutismCarlos Peña PaterninaNo ratings yet
- Suspended Education Urban Middle Schools in Crisis by Daniel J. Losen and Russell J. SkibaDocument25 pagesSuspended Education Urban Middle Schools in Crisis by Daniel J. Losen and Russell J. SkibaUrbanYouthJusticeNo ratings yet
- Violence & Abuse in Same-Sex Relationships:: A Review of LiteratureDocument32 pagesViolence & Abuse in Same-Sex Relationships:: A Review of LiteraturealtheaNo ratings yet
- Ocd and Covid 19 A New FrontierDocument11 pagesOcd and Covid 19 A New FrontierNaswa ArviedaNo ratings yet
- CASE STUDY - Conduct DisorderDocument4 pagesCASE STUDY - Conduct DisorderJona AddatuNo ratings yet
- Asperger's Syndrome An Introduction For EducatorsDocument7 pagesAsperger's Syndrome An Introduction For EducatorsDruga DanutNo ratings yet
- Child Custody and Juvenile ForensicsDocument9 pagesChild Custody and Juvenile ForensicsjhoyNo ratings yet
- Defusing Viol BehaviorDocument3 pagesDefusing Viol Behaviorbellydanceafrica9540No ratings yet
- Bender, Mirror, Mirror On The Wall, Reflecting On NarcissismDocument10 pagesBender, Mirror, Mirror On The Wall, Reflecting On NarcissismjuaromerNo ratings yet
- Biosketch Sample Forms DDocument3 pagesBiosketch Sample Forms DLindsayNo ratings yet
- Aspergers Syndrome Diagnosis and TreatmentDocument7 pagesAspergers Syndrome Diagnosis and TreatmentTilahun MogesNo ratings yet
- Federal Lawsuit in AJ Freund SlayingDocument36 pagesFederal Lawsuit in AJ Freund SlayingNational Content Desk100% (1)
- Social Skills DevelopmentWHITEDocument11 pagesSocial Skills DevelopmentWHITE__aguNo ratings yet
- Death Anxiety and Its Association With Hypochondriasis PDFDocument8 pagesDeath Anxiety and Its Association With Hypochondriasis PDFRebeca SilvaNo ratings yet
- Dissociative Identity Disorder-WikipediaDocument71 pagesDissociative Identity Disorder-Wikipediangdtri50% (2)
- Effective Treatments For Juvenile OffendersDocument8 pagesEffective Treatments For Juvenile OffendersAlguémNo ratings yet
- Adapting CBT For Children With An Autism Spectrum Disorder (ASD)Document3 pagesAdapting CBT For Children With An Autism Spectrum Disorder (ASD)Ina HasimNo ratings yet
- Final Report Child-Online-SurveyDocument96 pagesFinal Report Child-Online-SurveyhopeIshanzaNo ratings yet
- 1232 3 Fly Erasmund-Joint-Sport-EthicsDocument2 pages1232 3 Fly Erasmund-Joint-Sport-EthicshopeIshanzaNo ratings yet
- Fast Food Menu Version 5Document2 pagesFast Food Menu Version 5hopeIshanzaNo ratings yet
- BR and Sons Case Study Financial StatementsDocument2 pagesBR and Sons Case Study Financial StatementshopeIshanzaNo ratings yet
- Social Media's Impact on Football Fan EngagementDocument2 pagesSocial Media's Impact on Football Fan EngagementhopeIshanzaNo ratings yet
- Final Research Report Digital Woman July 2020Document22 pagesFinal Research Report Digital Woman July 2020hopeIshanzaNo ratings yet
- This Content Downloaded From 102.220.202.141 On Wed, 22 Feb 2023 10:17:28 UTCDocument21 pagesThis Content Downloaded From 102.220.202.141 On Wed, 22 Feb 2023 10:17:28 UTChopeIshanzaNo ratings yet
- Ad515-Barriers To E-Learning in Uganda-Afrobarometer Dispatch-10april22Document12 pagesAd515-Barriers To E-Learning in Uganda-Afrobarometer Dispatch-10april22hopeIshanzaNo ratings yet
- Football Clubs Need Community Support to SurviveDocument1 pageFootball Clubs Need Community Support to SurvivehopeIshanzaNo ratings yet
- Article 2Document14 pagesArticle 2hopeIshanzaNo ratings yet
- HNHMHDocument17 pagesHNHMHhopeIshanzaNo ratings yet
- DP 10398Document36 pagesDP 10398hopeIshanzaNo ratings yet
- The Effect of Parents' Attention On The Technology Usage of Children Between The Ages of Four and SixDocument9 pagesThe Effect of Parents' Attention On The Technology Usage of Children Between The Ages of Four and SixhopeIshanzaNo ratings yet
- 11 2020statistical Abstract 2020Document339 pages11 2020statistical Abstract 2020hopeIshanzaNo ratings yet
- Exploration of Anxiety Factors Among Students of Distance Learning: A Case Study of Allama Iqbal Open UniversityDocument12 pagesExploration of Anxiety Factors Among Students of Distance Learning: A Case Study of Allama Iqbal Open UniversityhopeIshanzaNo ratings yet
- A Study On Internet Addiction Among Teenagers in SDocument7 pagesA Study On Internet Addiction Among Teenagers in ShopeIshanzaNo ratings yet
- Group Counseling Session 1 ExperienceDocument2 pagesGroup Counseling Session 1 ExperiencehopeIshanzaNo ratings yet
- Customers Satisfaction On AirtelDocument46 pagesCustomers Satisfaction On AirtelChandu PrinceNo ratings yet
- Parental/Child Attachment - Child SurveyDocument4 pagesParental/Child Attachment - Child SurveyhopeIshanzaNo ratings yet
- Homolka Thesis 12 - 5 - 2013Document86 pagesHomolka Thesis 12 - 5 - 2013hopeIshanzaNo ratings yet
- Entrepreneurial Marketing - ENTR703Document344 pagesEntrepreneurial Marketing - ENTR703hopeIshanzaNo ratings yet
- NODocument1 pageNOhopeIshanzaNo ratings yet
- Group Counseling Session 4 ExperienceDocument1 pageGroup Counseling Session 4 ExperiencehopeIshanzaNo ratings yet
- Questionaire GuideDocument3 pagesQuestionaire GuidehopeIshanzaNo ratings yet
- Gestalt Therapy ApproachDocument3 pagesGestalt Therapy ApproachhopeIshanzaNo ratings yet
- Group Counseling Session 2 ExperienceDocument1 pageGroup Counseling Session 2 ExperiencehopeIshanzaNo ratings yet
- I Welcomed and Recorded Attendance For Members PresentedDocument1 pageI Welcomed and Recorded Attendance For Members PresentedhopeIshanzaNo ratings yet
- Strengths Faith ConsistenciesDocument4 pagesStrengths Faith ConsistencieshopeIshanzaNo ratings yet
- Strengths Faith ConsistenciesDocument4 pagesStrengths Faith ConsistencieshopeIshanzaNo ratings yet
- Assumptions/ Basic Concepts Methods/Techniques in Group Therapeutic Goals Role & Functions of Group Leader Multicultural Issues Consistency/ConflictDocument3 pagesAssumptions/ Basic Concepts Methods/Techniques in Group Therapeutic Goals Role & Functions of Group Leader Multicultural Issues Consistency/ConflicthopeIshanzaNo ratings yet
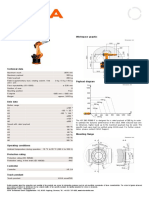
- KR 280 R3080 F technical specificationsDocument1 pageKR 280 R3080 F technical specificationsDorobantu CatalinNo ratings yet
- Acid-Base Neut Inquiry Student Handout JN KEYDocument5 pagesAcid-Base Neut Inquiry Student Handout JN KEYbradle2005No ratings yet
- Marivy Abella ResearchDocument43 pagesMarivy Abella ResearchRo Gi LynNo ratings yet
- Course 1 ProjectDocument6 pagesCourse 1 ProjectDhruvNo ratings yet
- Sales Target Planning ToolkitDocument7 pagesSales Target Planning ToolkitCarmenLarisaNo ratings yet
- Midcheek Lift Using Facial Soft-Tissue Spaces of The MidcheekDocument11 pagesMidcheek Lift Using Facial Soft-Tissue Spaces of The MidcheekЩербакова ЛенаNo ratings yet
- Itp Concrete CoatingDocument4 pagesItp Concrete Coatingkaml100% (1)
- Las 4.4 - Hope 4 - Mountaineering (Hiking, Trekking, Camping, Orienteering)Document5 pagesLas 4.4 - Hope 4 - Mountaineering (Hiking, Trekking, Camping, Orienteering)Maricel EsperatNo ratings yet
- Lesson Plan For Demonstration (COT) : School Grade Level Teacher Learning Area Teaching Dates and Time QuarterDocument6 pagesLesson Plan For Demonstration (COT) : School Grade Level Teacher Learning Area Teaching Dates and Time Quartermaritel dawaNo ratings yet
- Kwame Ture InterviewDocument8 pagesKwame Ture InterviewSumayya K AliNo ratings yet
- Probability Concepts and Random Variable - SMTA1402: Unit - IDocument105 pagesProbability Concepts and Random Variable - SMTA1402: Unit - IVigneshwar SNo ratings yet
- Participation RubricDocument2 pagesParticipation RubricCarmen Ibañez AlvarezNo ratings yet
- Clinical Practice Guidelines On Postmenopausal Osteoporosis: An Executive Summary and Recommendations - Update 2019-2020Document17 pagesClinical Practice Guidelines On Postmenopausal Osteoporosis: An Executive Summary and Recommendations - Update 2019-2020Marwa YassinNo ratings yet
- Dip HIV Man (SA) Past Papers - 2015 2nd Semester 24-1-2017Document2 pagesDip HIV Man (SA) Past Papers - 2015 2nd Semester 24-1-2017matenten100% (1)
- 14 Ways To Acquire KnowledgeDocument4 pages14 Ways To Acquire KnowledgeRenato MiguelNo ratings yet
- Review of Dr. Mark Cheng's "Prehab-Rehab 101" SeriesDocument6 pagesReview of Dr. Mark Cheng's "Prehab-Rehab 101" SeriesWilliam TortorielloNo ratings yet
- I Am Sharing 'ASSIGNMENT MAT099 - E08G5 - WRTTEN REPORT' With YouDocument23 pagesI Am Sharing 'ASSIGNMENT MAT099 - E08G5 - WRTTEN REPORT' With YouaqilNo ratings yet
- EAPP Report - Advertisement FallacyDocument13 pagesEAPP Report - Advertisement FallacyくんcharlsNo ratings yet
- GCMS-QP2010 User'sGuide (Ver2.5) PDFDocument402 pagesGCMS-QP2010 User'sGuide (Ver2.5) PDFnguyenvietanhbtNo ratings yet
- Header LpuDocument3 pagesHeader LpuL.a.ZumárragaNo ratings yet
- Excerpts From The Way of The Samurai (Shīdo) : Primary Source Document With Questions (DBQS)Document2 pagesExcerpts From The Way of The Samurai (Shīdo) : Primary Source Document With Questions (DBQS)Valeria MontalvaNo ratings yet
- Faktor OrganisasiDocument9 pagesFaktor OrganisasiNur Fatin NabilahNo ratings yet
- Muhammad Farrukh QAMAR - Assessment 2 Student Practical Demonstration of Tasks AURAMA006 V2Document19 pagesMuhammad Farrukh QAMAR - Assessment 2 Student Practical Demonstration of Tasks AURAMA006 V2Rana Muhammad Ashfaq Khan0% (1)
- Transcricao How To Be Happy (Before Success) - by Earl NightingaleDocument62 pagesTranscricao How To Be Happy (Before Success) - by Earl NightingalepauloalaraNo ratings yet
- Rabbani Env 3Document298 pagesRabbani Env 3Arnob SarkerNo ratings yet
- Providing Clean Water and Financial Assistance in Binangonan RizalDocument29 pagesProviding Clean Water and Financial Assistance in Binangonan RizalArebeeJayBelloNo ratings yet
- Building Power and InfluenceDocument5 pagesBuilding Power and InfluenceQuang-Nam Nguyen100% (1)
- CXO 7050 Rev 14.3.13 PDFDocument1 pageCXO 7050 Rev 14.3.13 PDFrajaramghoshNo ratings yet
- Logging Levels in Log4j - Tutorialspoint ExamplesDocument3 pagesLogging Levels in Log4j - Tutorialspoint ExamplesJai PannuNo ratings yet
- Breaking the Habit of Being YourselfFrom EverandBreaking the Habit of Being YourselfRating: 4.5 out of 5 stars4.5/5 (1456)
- Summary: Atomic Habits by James Clear: An Easy & Proven Way to Build Good Habits & Break Bad OnesFrom EverandSummary: Atomic Habits by James Clear: An Easy & Proven Way to Build Good Habits & Break Bad OnesRating: 5 out of 5 stars5/5 (1633)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The 7 Habits of Highly Effective People: The Infographics EditionFrom EverandThe 7 Habits of Highly Effective People: The Infographics EditionRating: 4 out of 5 stars4/5 (2475)
- The Mountain is You: Transforming Self-Sabotage Into Self-MasteryFrom EverandThe Mountain is You: Transforming Self-Sabotage Into Self-MasteryRating: 4.5 out of 5 stars4.5/5 (877)
- Permission to Be Gentle: 7 Self-Love Affirmations for the Highly SensitiveFrom EverandPermission to Be Gentle: 7 Self-Love Affirmations for the Highly SensitiveRating: 4.5 out of 5 stars4.5/5 (14)
- Becoming Supernatural: How Common People Are Doing The UncommonFrom EverandBecoming Supernatural: How Common People Are Doing The UncommonRating: 5 out of 5 stars5/5 (1478)
- Maktub: An Inspirational Companion to The AlchemistFrom EverandMaktub: An Inspirational Companion to The AlchemistRating: 5 out of 5 stars5/5 (2)
- The Power of Now: A Guide to Spiritual EnlightenmentFrom EverandThe Power of Now: A Guide to Spiritual EnlightenmentRating: 4.5 out of 5 stars4.5/5 (4122)
- No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems ModelFrom EverandNo Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems ModelRating: 5 out of 5 stars5/5 (2)
- Summary of Atomic Habits: An Easy and Proven Way to Build Good Habits and Break Bad Ones by James ClearFrom EverandSummary of Atomic Habits: An Easy and Proven Way to Build Good Habits and Break Bad Ones by James ClearRating: 4.5 out of 5 stars4.5/5 (557)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- How to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipFrom EverandHow to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipRating: 4.5 out of 5 stars4.5/5 (1135)
- Eat That Frog!: 21 Great Ways to Stop Procrastinating and Get More Done in Less TimeFrom EverandEat That Frog!: 21 Great Ways to Stop Procrastinating and Get More Done in Less TimeRating: 4.5 out of 5 stars4.5/5 (3225)
- Seven Spiritual Laws of Success: A Practical Guide to the Fulfillment of Your DreamsFrom EverandSeven Spiritual Laws of Success: A Practical Guide to the Fulfillment of Your DreamsRating: 4.5 out of 5 stars4.5/5 (1548)
- The 5 Second Rule: Transform your Life, Work, and Confidence with Everyday CourageFrom EverandThe 5 Second Rule: Transform your Life, Work, and Confidence with Everyday CourageRating: 5 out of 5 stars5/5 (8)
- When You're Ready, This Is How You HealFrom EverandWhen You're Ready, This Is How You HealRating: 4.5 out of 5 stars4.5/5 (183)
- Chakras and Yoga: Finding Inner Harmony Through Practice, Awaken the Energy Centers for Optimal Physical and Spiritual Health.From EverandChakras and Yoga: Finding Inner Harmony Through Practice, Awaken the Energy Centers for Optimal Physical and Spiritual Health.Rating: 4 out of 5 stars4/5 (2)
- Neville Goddard Master Course to Manifest Your Desires Into Reality Using The Law of Attraction: Learn the Secret to Overcoming Your Current Problems and Limitations, Attaining Your Goals, and Achieving Health, Wealth, Happiness and Success!From EverandNeville Goddard Master Course to Manifest Your Desires Into Reality Using The Law of Attraction: Learn the Secret to Overcoming Your Current Problems and Limitations, Attaining Your Goals, and Achieving Health, Wealth, Happiness and Success!Rating: 5 out of 5 stars5/5 (284)
- When Things Fall Apart: Heart Advice for Difficult TimesFrom EverandWhen Things Fall Apart: Heart Advice for Difficult TimesRating: 4.5 out of 5 stars4.5/5 (3)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Bedtime Stories for Stressed Adults: Sleep Meditation Stories to Melt Stress and Fall Asleep Fast Every NightFrom EverandBedtime Stories for Stressed Adults: Sleep Meditation Stories to Melt Stress and Fall Asleep Fast Every NightRating: 4.5 out of 5 stars4.5/5 (124)
- The Little Book of Stoicism: Timeless Wisdom to Gain Resilience, Confidence, and CalmnessFrom EverandThe Little Book of Stoicism: Timeless Wisdom to Gain Resilience, Confidence, and CalmnessRating: 4.5 out of 5 stars4.5/5 (270)