You might also like
- Physical Activity Guidelines For Older AdultsDocument5 pagesPhysical Activity Guidelines For Older AdultsmartinNo ratings yet
- 2002-Meisler-Importancia de FZ y Flex en AFDocument6 pages2002-Meisler-Importancia de FZ y Flex en AFChuleNo ratings yet
- Exercise Guidelines For Chronic Kidney Disease PatientsDocument3 pagesExercise Guidelines For Chronic Kidney Disease Patientsluis Gomez VallejoNo ratings yet
- Tiffanny Ocktivianie Tobing - Quiz of Physical Activity, Excercise and RehabilitationDocument3 pagesTiffanny Ocktivianie Tobing - Quiz of Physical Activity, Excercise and RehabilitationTiffanny Ocktivianie TobingNo ratings yet
- Develop Med Child Neuro - 2016 - Verschuren - Exercise and Physical Activity Recommendations For People With Cerebral PalsyDocument11 pagesDevelop Med Child Neuro - 2016 - Verschuren - Exercise and Physical Activity Recommendations For People With Cerebral PalsyCláudia SilvaNo ratings yet
- Physical Inactivity Is Now Identified As The Fourth: Lesson 2Document8 pagesPhysical Inactivity Is Now Identified As The Fourth: Lesson 2Yzabelle EncoyNo ratings yet
- Benefits of Exercise in The Older PopDocument11 pagesBenefits of Exercise in The Older PopRafael PortoNo ratings yet
- Schutzer, KA. Et Al. (2004) - Barriers and Motivations To Exercise in Older Adults PDFDocument6 pagesSchutzer, KA. Et Al. (2004) - Barriers and Motivations To Exercise in Older Adults PDFDiana SilvaNo ratings yet
- Effectiveness of Physical ExercisesDocument5 pagesEffectiveness of Physical ExercisesNicole LabradoNo ratings yet
- Physical Activity and Exercise For Older People DuDocument3 pagesPhysical Activity and Exercise For Older People DuTari AudinaNo ratings yet
- AAA Lesson 1 8Document55 pagesAAA Lesson 1 8Ani TubeNo ratings yet
- Viewcontent CgiDocument13 pagesViewcontent CgimariaNo ratings yet
- Exercise For AdultsDocument7 pagesExercise For AdultsPelina LazariNo ratings yet
- Physical ActivityDocument5 pagesPhysical ActivityshaviraNo ratings yet
- Exercise for GeriatricsDocument9 pagesExercise for GeriatricsP.Senthil SelvamNo ratings yet
- 2018%2F7856823Document4 pages2018%2F7856823itskasho0332No ratings yet
- Mcadafa-Tema 1-Costache Cosmin-AndreiDocument8 pagesMcadafa-Tema 1-Costache Cosmin-AndreiCostache Cosmin-AndreiNo ratings yet
- Circoutcomes 118 005263 PDFDocument3 pagesCircoutcomes 118 005263 PDFStella UrdinolaNo ratings yet
- Long QuizDocument6 pagesLong QuizMae EsmadeNo ratings yet
- ACE PT5th Manual Ch1Document34 pagesACE PT5th Manual Ch1Eliot Kh100% (2)
- Role and Scope of Practice For The Personal TrainerDocument34 pagesRole and Scope of Practice For The Personal Trainerislam100% (1)
- Doctors' lack of exercise training limits physical activity prescriptionDocument3 pagesDoctors' lack of exercise training limits physical activity prescriptionMartijn JohanNo ratings yet
- Water-Versus Land-Based Exercise Effects On Physical Fitness in Older WomenDocument8 pagesWater-Versus Land-Based Exercise Effects On Physical Fitness in Older WomenHONGJY100% (1)
- Eng 2 Exercise Research PaperDocument12 pagesEng 2 Exercise Research Paperapi-534316399No ratings yet
- Exercise PhysiologyDocument27 pagesExercise PhysiologyJericho PanisNo ratings yet
- Coverage For QuizDocument12 pagesCoverage For QuizSaila mae SurioNo ratings yet
- 2008 Physical Activity Guidelines: National Council On Strength & FitnessDocument2 pages2008 Physical Activity Guidelines: National Council On Strength & FitnessPaulo ZulluNo ratings yet
- Jama Physical ActivityDocument3 pagesJama Physical ActivityflorNo ratings yet
- 34.the Physical Therapist's Role in Physical Activity PromotionDocument5 pages34.the Physical Therapist's Role in Physical Activity Promotionanggie mosqueraNo ratings yet
- Ejercicio Enfermo Renal EsDocument15 pagesEjercicio Enfermo Renal EsOscarDavidGordilloGonzalezNo ratings yet
- Musculoskeletal Wps OfficeDocument27 pagesMusculoskeletal Wps OfficeSteffanie TalaueNo ratings yet
- 10 1016@j Mcna 2019 10 003Document10 pages10 1016@j Mcna 2019 10 003Arnold BarraNo ratings yet
- Effects of Circuit Training on Health Fitness of B.Ed. StudentsDocument24 pagesEffects of Circuit Training on Health Fitness of B.Ed. StudentsBilisuma MuletaNo ratings yet
- 60ish Youngsters Need Strength TrainingDocument5 pages60ish Youngsters Need Strength TrainingArun KapaniaNo ratings yet
- PE 12 Fitness Exercise: The Premier State University in Zamboanga Del NorteDocument11 pagesPE 12 Fitness Exercise: The Premier State University in Zamboanga Del NorteMARK ANTHONY FERNANDEZNo ratings yet
- UntitledDocument5 pagesUntitledkennethquenanoNo ratings yet
- Path FitDocument11 pagesPath FitChristin Me LocsinNo ratings yet
- Cardiovascular and Behavioral Effects of Aerobic Exercise Training in Healthy Older Men and WomenDocument11 pagesCardiovascular and Behavioral Effects of Aerobic Exercise Training in Healthy Older Men and WomenSilvana CarneiroNo ratings yet
- A Framework For Exercise Prescription: DOI: 10.1097/TGR.0000000000000011Document23 pagesA Framework For Exercise Prescription: DOI: 10.1097/TGR.0000000000000011Lft Ediel PiñaNo ratings yet
- Nutrition and Physical Activity InterventionsDocument28 pagesNutrition and Physical Activity Interventionsoknutricion1No ratings yet
- Articulo Salud PublicaDocument18 pagesArticulo Salud PublicaCatherinne Quiñonez GutierrezNo ratings yet
- 2021A Regular Exercise and Patterns of Response Across Multiple Cardiometabolic Traits - The HERITAGE Family StudyDocument7 pages2021A Regular Exercise and Patterns of Response Across Multiple Cardiometabolic Traits - The HERITAGE Family StudyDavid Peñalver NavarroNo ratings yet
- Exercise Prescription in Oncology Patients: General PrinciplesDocument9 pagesExercise Prescription in Oncology Patients: General PrinciplesІра ГориньNo ratings yet
- Cir 0000000000001035Document12 pagesCir 0000000000001035LeblancNo ratings yet
- DownloadDocument9 pagesDownloadcesar8319No ratings yet
- AF y SobrevivenciaDocument7 pagesAF y SobrevivenciaarcadetorNo ratings yet
- Effects of Different Exercise Interventions On Risk of Falls A Systematic ReviewDocument10 pagesEffects of Different Exercise Interventions On Risk of Falls A Systematic ReviewLeonardoValenzuelaNo ratings yet
- PE - MUSCLE and BONE STRENGHTENING EVENTSDocument5 pagesPE - MUSCLE and BONE STRENGHTENING EVENTSJanelle TenebrosoNo ratings yet
- The Parts of Physical FitnessDocument12 pagesThe Parts of Physical FitnessDe Jesus Joshua PaulNo ratings yet
- Exercise and Older Patients - Prescribing Guidelines PDFDocument8 pagesExercise and Older Patients - Prescribing Guidelines PDFMuhammad ReyhanNo ratings yet
- Exercice Is MedicineDocument55 pagesExercice Is MedicineDario MoralesNo ratings yet
- Health-Lifestyles-Final-Recommendation-Statement USPSTF in Adults Without Risks 2017Document8 pagesHealth-Lifestyles-Final-Recommendation-Statement USPSTF in Adults Without Risks 2017Kathy VelasquezNo ratings yet
- HOPE 1 Module 1 (Exercise For Fitness)Document10 pagesHOPE 1 Module 1 (Exercise For Fitness)Ma.Angelica B. AcedillaNo ratings yet
- Prescription of Resistance Training For Healthy PopulationsDocument12 pagesPrescription of Resistance Training For Healthy PopulationsChristine LeeNo ratings yet
- Fritschi 2014 PDFDocument8 pagesFritschi 2014 PDFCinthiaDReisNo ratings yet
- Feasibility and Safety of Intradialysis Yoga and Education in Maintenance Hemodialysis PatientsDocument9 pagesFeasibility and Safety of Intradialysis Yoga and Education in Maintenance Hemodialysis PatientsrizkaNo ratings yet
- 267 FullDocument6 pages267 FullobedidomNo ratings yet
- HHS Public Access: Exercise and Physical Activity Recommendations For People With Cerebral PalsyDocument22 pagesHHS Public Access: Exercise and Physical Activity Recommendations For People With Cerebral PalsyBryan Alexis Rodriguez CastroNo ratings yet
- The Ethics of Exercise in Eating Disorders Can An Ethic - 2017 - Journal of SpoDocument4 pagesThe Ethics of Exercise in Eating Disorders Can An Ethic - 2017 - Journal of SpoSisi WeeraNo ratings yet
- Cuidados Del Adulto MayorDocument9 pagesCuidados Del Adulto MayorBeatrizNo ratings yet
- Health Assessment ChecklistDocument19 pagesHealth Assessment Checklistramzan aliNo ratings yet
- Unit Vii Assessment of The Abdomen, Anus and RectumDocument86 pagesUnit Vii Assessment of The Abdomen, Anus and Rectumramzan aliNo ratings yet
- Unit5 Assessment of The Abdomen, Anus and RectumDocument95 pagesUnit5 Assessment of The Abdomen, Anus and Rectumramzan aliNo ratings yet
- NCBI BookshelfDocument9 pagesNCBI Bookshelframzan aliNo ratings yet
- Braden Scale Powerpoint PDFDocument29 pagesBraden Scale Powerpoint PDFsilvia90% (10)
- Importance of Cultural Sensitivity in Therapeutic TransactionsDocument17 pagesImportance of Cultural Sensitivity in Therapeutic Transactionsramzan aliNo ratings yet
- Unit5 Assessment of The Abdomen, Anus and RectumDocument95 pagesUnit5 Assessment of The Abdomen, Anus and Rectumramzan aliNo ratings yet
- Tere Darbar Me Dil Thaam Ke Wo Aata HaiDocument2 pagesTere Darbar Me Dil Thaam Ke Wo Aata Hairamzan aliNo ratings yet
- Differentiating Delirium, Dementia, and DepressionDocument4 pagesDifferentiating Delirium, Dementia, and Depressionramzan aliNo ratings yet
- Dying With Dignity in The Intensive Care Unit: Review ArticleDocument9 pagesDying With Dignity in The Intensive Care Unit: Review ArticleRodrigoSachiFreitasNo ratings yet
- Dying With Dignity in The Intensive Care Unit: Review ArticleDocument9 pagesDying With Dignity in The Intensive Care Unit: Review ArticleRodrigoSachiFreitasNo ratings yet
- Delirium in The ElderlyDocument8 pagesDelirium in The Elderlyloko_knvbNo ratings yet
- Delirium Prevention Diagnosis and Management PDF 35109327290821Document21 pagesDelirium Prevention Diagnosis and Management PDF 35109327290821ramzan aliNo ratings yet
- Management: Delirium Assessment and Treatment For Older AdultsDocument2 pagesManagement: Delirium Assessment and Treatment For Older Adultsramzan aliNo ratings yet
- DeliriumDocument38 pagesDeliriumVicta RyzaNo ratings yet
- Detroyer2018 Article EffectOfAnInteractiveE-learninDocument9 pagesDetroyer2018 Article EffectOfAnInteractiveE-learninramzan aliNo ratings yet
- Implementing The Best Available Evidence in Early DeliriumDocument7 pagesImplementing The Best Available Evidence in Early Deliriumramzan aliNo ratings yet
- Implementing The Best Available Evidence in Early DeliriumDocument7 pagesImplementing The Best Available Evidence in Early Deliriumramzan aliNo ratings yet
- Delirium: A Guide For Patients, Family Members, and CaregiversDocument2 pagesDelirium: A Guide For Patients, Family Members, and Caregiversramzan aliNo ratings yet
- Delirium in The Acute Care Setting: Characteristics, Diagnosis and TreatmentDocument66 pagesDelirium in The Acute Care Setting: Characteristics, Diagnosis and TreatmentIsrael Sánchez AlvarezNo ratings yet
- Delirium in The ElderlyDocument8 pagesDelirium in The Elderlyloko_knvbNo ratings yet
- Clinical Pearls in GeriatricsDocument1 pageClinical Pearls in Geriatricsramzan aliNo ratings yet
- DeliriumDocument38 pagesDeliriumVicta RyzaNo ratings yet
- WHO MHGap Guide English PDFDocument121 pagesWHO MHGap Guide English PDFYolanda Dwi OktaviyaniNo ratings yet
- Bed Bath Procedure: Presented By: Prof - Vijayreddy Vandali Dept of Medical-Surgical Nursing IndiaDocument17 pagesBed Bath Procedure: Presented By: Prof - Vijayreddy Vandali Dept of Medical-Surgical Nursing Indiaramzan aliNo ratings yet
- Lesson Plan DeliriumDocument9 pagesLesson Plan DeliriumSILUVERU SALOMI100% (1)
- Maintaining Personal HygieneDocument6 pagesMaintaining Personal Hygieneramzan aliNo ratings yet
- Oral Hygiene Care GuideDocument1 pageOral Hygiene Care Guideramzan aliNo ratings yet
- 8 Matching QuestionsDocument14 pages8 Matching Questionsramzan aliNo ratings yet
- Hildebrandt 2000 PDFDocument12 pagesHildebrandt 2000 PDFAlexandre FerreiraNo ratings yet
- ACSM's Exercise Is Medicine. A Clinician's Guide To Exercise Prescription (2009)Document274 pagesACSM's Exercise Is Medicine. A Clinician's Guide To Exercise Prescription (2009)Eduardo Pedro100% (5)
- Assessing Physical Activities for Health OptimizationDocument15 pagesAssessing Physical Activities for Health OptimizationJoanna Marie RamosNo ratings yet
- Effectiveness of Bread and Pastry ProducDocument11 pagesEffectiveness of Bread and Pastry ProducRogelyn RendoqueNo ratings yet
- Global: Physical Activity Questionnaire (GPAQ)Document2 pagesGlobal: Physical Activity Questionnaire (GPAQ)saya hanahNo ratings yet
- Physical Activity and Sedentary Behaviour: A Brief To SupportDocument8 pagesPhysical Activity and Sedentary Behaviour: A Brief To SupportPhilippe Ceasar C. BascoNo ratings yet
- Mastered and Least Mastered MAPEH CompetenciesDocument4 pagesMastered and Least Mastered MAPEH CompetenciesLyza SuribenNo ratings yet
- PE1 DANCE FUNDAMENTALSDocument8 pagesPE1 DANCE FUNDAMENTALSDM Camilot IINo ratings yet
- PE 3 Modules StudentsDocument96 pagesPE 3 Modules StudentsRosemarie R. Reyes50% (2)
- Pointers For Grade 11Document2 pagesPointers For Grade 11Ella Jane Manolos PaguioNo ratings yet
- Active Video Games Helps Some Kids Get Active by Jennifer WarnerDocument2 pagesActive Video Games Helps Some Kids Get Active by Jennifer WarnerAdexentrix WPNo ratings yet
- Physical Education Lesson Plan on Fitness and Lifestyle DiseasesDocument6 pagesPhysical Education Lesson Plan on Fitness and Lifestyle DiseasesRocelgie Jimenez100% (2)
- Table of Contents - RPMSDocument2 pagesTable of Contents - RPMSMaria Virginia FernandezNo ratings yet
- Cool Azul Sports GelDocument1 pageCool Azul Sports GelroslizamhNo ratings yet
- GMSD Cold Weather Advisory GuidelinesDocument1 pageGMSD Cold Weather Advisory Guidelinesapi-341432319No ratings yet
- Pelvic Floor Physiotherapy HOACllDocument9 pagesPelvic Floor Physiotherapy HOACllEsteban CayuelasNo ratings yet
- Cap Wellness InitiativeDocument15 pagesCap Wellness Initiativeapi-525572309No ratings yet
- Q4 HOPE 2 - Module 4Document9 pagesQ4 HOPE 2 - Module 4May Ann GodezanoNo ratings yet
- Safety Nutrition and Health in Early Education 6th Edition Robertson Test BankDocument32 pagesSafety Nutrition and Health in Early Education 6th Edition Robertson Test Bankmilterjubilatepo8y1b100% (25)
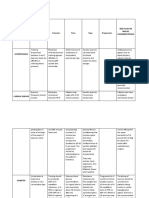
- Medical Conditions Frequency Intensity Time Type Progression Red Flags or Special ConsideratrionsDocument4 pagesMedical Conditions Frequency Intensity Time Type Progression Red Flags or Special ConsideratrionsClaire Madriaga GidoNo ratings yet
- Lesson Plan COT 1 2021 2022Document3 pagesLesson Plan COT 1 2021 2022seph bronNo ratings yet
- Etec 500 Assignment 2b Final Draft - Research Analysis and CritiqueDocument11 pagesEtec 500 Assignment 2b Final Draft - Research Analysis and Critiqueapi-127920431No ratings yet
- Mainstreaming Physical Activity in Landscape Architecture DesignDocument176 pagesMainstreaming Physical Activity in Landscape Architecture DesignAlgi FahriNo ratings yet
- DLL in Health 7 3rd QuarterDocument2 pagesDLL in Health 7 3rd QuarterJuna Lyn Hermida ArellonNo ratings yet
- DLL Mapeh May 29 June 2 2023Document3 pagesDLL Mapeh May 29 June 2 2023Cezar John SantosNo ratings yet
- Optimizing Exercise and Physical Activity in Older PeopleDocument356 pagesOptimizing Exercise and Physical Activity in Older PeopleNimouzha Imho100% (1)
- Omnibus Health Guidelines For The Elderly 2022Document81 pagesOmnibus Health Guidelines For The Elderly 2022Raymunda Rauto-avila100% (1)
- Elective II Group 1 Chronic IllnessDocument31 pagesElective II Group 1 Chronic IllnessAldrine Albor Anyayahan INo ratings yet
- Pathfit 1 Module 3 Week 4Document6 pagesPathfit 1 Module 3 Week 4KrisChan ProdNo ratings yet
- Effect of A Program of Physical Activity Motivated by Lipid Parameters of Patients With Obesity and or Overweight PDFDocument6 pagesEffect of A Program of Physical Activity Motivated by Lipid Parameters of Patients With Obesity and or Overweight PDFMarlio Andres Vargas PolaniaNo ratings yet
- Body by Science: A Research Based Program for Strength Training, Body building, and Complete Fitness in 12 Minutes a WeekFrom EverandBody by Science: A Research Based Program for Strength Training, Body building, and Complete Fitness in 12 Minutes a WeekRating: 4.5 out of 5 stars4.5/5 (84)
- Chair Yoga: Sit, Stretch, and Strengthen Your Way to a Happier, Healthier YouFrom EverandChair Yoga: Sit, Stretch, and Strengthen Your Way to a Happier, Healthier YouRating: 3.5 out of 5 stars3.5/5 (5)
- Functional Training and Beyond: Building the Ultimate Superfunctional Body and MindFrom EverandFunctional Training and Beyond: Building the Ultimate Superfunctional Body and MindRating: 4.5 out of 5 stars4.5/5 (1)
- Chakras and Yoga: Finding Inner Harmony Through Practice, Awaken the Energy Centers for Optimal Physical and Spiritual Health.From EverandChakras and Yoga: Finding Inner Harmony Through Practice, Awaken the Energy Centers for Optimal Physical and Spiritual Health.Rating: 4 out of 5 stars4/5 (2)
- Boundless: Upgrade Your Brain, Optimize Your Body & Defy AgingFrom EverandBoundless: Upgrade Your Brain, Optimize Your Body & Defy AgingRating: 4.5 out of 5 stars4.5/5 (66)
- Relentless: From Good to Great to UnstoppableFrom EverandRelentless: From Good to Great to UnstoppableRating: 5 out of 5 stars5/5 (780)
- Power of 10: The Once-A-Week Slow Motion Fitness RevolutionFrom EverandPower of 10: The Once-A-Week Slow Motion Fitness RevolutionRating: 3.5 out of 5 stars3.5/5 (11)
- SAS Training Manual: How to get fit enough to pass a special forces selection courseFrom EverandSAS Training Manual: How to get fit enough to pass a special forces selection courseRating: 4 out of 5 stars4/5 (3)
- Strong Is the New Beautiful: Embrace Your Natural Beauty, Eat Clean, and Harness Your PowerFrom EverandStrong Is the New Beautiful: Embrace Your Natural Beauty, Eat Clean, and Harness Your PowerRating: 4 out of 5 stars4/5 (5)
- The Yogi Code: Seven Universal Laws of Infinite SuccessFrom EverandThe Yogi Code: Seven Universal Laws of Infinite SuccessRating: 4.5 out of 5 stars4.5/5 (104)
- Peak: The New Science of Athletic Performance That is Revolutionizing SportsFrom EverandPeak: The New Science of Athletic Performance That is Revolutionizing SportsRating: 5 out of 5 stars5/5 (95)
- Wall Pilates: Quick-and-Simple to Lose Weight and Stay Healthy. A 30-Day Journey with + 100 ExercisesFrom EverandWall Pilates: Quick-and-Simple to Lose Weight and Stay Healthy. A 30-Day Journey with + 100 ExercisesNo ratings yet
- Endure: Mind, Body, and the Curiously Elastic Limits of Human PerformanceFrom EverandEndure: Mind, Body, and the Curiously Elastic Limits of Human PerformanceRating: 4.5 out of 5 stars4.5/5 (237)
- Muscle for Life: Get Lean, Strong, and Healthy at Any Age!From EverandMuscle for Life: Get Lean, Strong, and Healthy at Any Age!Rating: 4.5 out of 5 stars4.5/5 (22)
- The Calisthenics Codex: Fifty Exercises for Functional FitnessFrom EverandThe Calisthenics Codex: Fifty Exercises for Functional FitnessRating: 4 out of 5 stars4/5 (9)
- Hero Maker: 12 Weeks to Superhero Fit: A Hollywood Trainer's REAL Guide to Getting the Body You've Always WantedFrom EverandHero Maker: 12 Weeks to Superhero Fit: A Hollywood Trainer's REAL Guide to Getting the Body You've Always WantedRating: 4 out of 5 stars4/5 (1)
- Yamas & Niyamas: Exploring Yoga's Ethical PracticeFrom EverandYamas & Niyamas: Exploring Yoga's Ethical PracticeRating: 4.5 out of 5 stars4.5/5 (110)
- If You Like Exercise … Chances Are You’Re Doing It Wrong: Proper Strength Training for Maximum ResultsFrom EverandIf You Like Exercise … Chances Are You’Re Doing It Wrong: Proper Strength Training for Maximum ResultsRating: 4.5 out of 5 stars4.5/5 (7)
- 7 Weeks to 50 Pull-Ups: Strengthen and Sculpt Your Arms, Shoulders, Back, and Abs by Training to Do 50 Consecutive Pull-UpsFrom Everand7 Weeks to 50 Pull-Ups: Strengthen and Sculpt Your Arms, Shoulders, Back, and Abs by Training to Do 50 Consecutive Pull-UpsRating: 3.5 out of 5 stars3.5/5 (2)
- 7 Weeks to 10 Pounds of Muscle: The Complete Day-by-Day Program to Pack on Lean, Healthy Muscle MassFrom Everand7 Weeks to 10 Pounds of Muscle: The Complete Day-by-Day Program to Pack on Lean, Healthy Muscle MassRating: 4 out of 5 stars4/5 (2)
- Calisthenics: Guide for Bodyweight Exercise, Build your Dream Body in 30 MinutesFrom EverandCalisthenics: Guide for Bodyweight Exercise, Build your Dream Body in 30 MinutesRating: 3 out of 5 stars3/5 (5)
- Calisthenics: 12 Effective Exercises to Build Calisthenics Body in 14 DaysFrom EverandCalisthenics: 12 Effective Exercises to Build Calisthenics Body in 14 DaysRating: 3 out of 5 stars3/5 (5)
- Meat Is for Pussies: A How-To Guide for Dudes Who Want to Get Fit, Kick Ass, and Take NamesFrom EverandMeat Is for Pussies: A How-To Guide for Dudes Who Want to Get Fit, Kick Ass, and Take NamesRating: 3.5 out of 5 stars3.5/5 (8)
- Depression Hates a Moving Target: How Running With My Dog Brought Me Back From the BrinkFrom EverandDepression Hates a Moving Target: How Running With My Dog Brought Me Back From the BrinkRating: 4 out of 5 stars4/5 (35)
- Deezify's Epic Workout Handbook: An Illustrated Guide to Getting SwoleFrom EverandDeezify's Epic Workout Handbook: An Illustrated Guide to Getting SwoleRating: 5 out of 5 stars5/5 (1)