You might also like
- Ohc'C - J (Lechmihîm CM - (M - L (Ncham) (F - : PSSM DPD DPDDocument8 pagesOhc'C - J (Lechmihîm CM - (M - L (Ncham) (F - : PSSM DPD DPDVlad IliescuNo ratings yet
- Clinical Record Form: Check Blood Pressure, Temperature and PulseDocument5 pagesClinical Record Form: Check Blood Pressure, Temperature and PulseVlad IliescuNo ratings yet
- Mini-Mental State Examination (MMSE)Document2 pagesMini-Mental State Examination (MMSE)Besth HutabaratNo ratings yet
- Viva PaperDocument5 pagesViva PaperVlad IliescuNo ratings yet
- Neurological Examination PDFDocument98 pagesNeurological Examination PDFVimal NishadNo ratings yet
- Mini-Mental State Examination (MMSE)Document2 pagesMini-Mental State Examination (MMSE)Besth HutabaratNo ratings yet
- Comparative Oral Health Status of An Adult Sudanese Population Using Miswak or Toothbrush RegularlyDocument11 pagesComparative Oral Health Status of An Adult Sudanese Population Using Miswak or Toothbrush RegularlyVlad IliescuNo ratings yet
- Miswak An Aspect of Dental Care in IslamDocument12 pagesMiswak An Aspect of Dental Care in IslamVlad IliescuNo ratings yet
- Neurological Examination PDFDocument98 pagesNeurological Examination PDFVimal NishadNo ratings yet
- Order of Neurological ExaminationDocument2 pagesOrder of Neurological ExaminationVlad IliescuNo ratings yet
- Miswak Users' Behavior Model Based On The Theory of Planned Behavior in The Country With The Largest Muslim PopulationDocument8 pagesMiswak Users' Behavior Model Based On The Theory of Planned Behavior in The Country With The Largest Muslim PopulationVlad IliescuNo ratings yet
- Comparative Study To Assess The Effect of Chewing Stick and Toothbrush On Oral Hygiene and Periodontal Status Among Indian PopulationDocument7 pagesComparative Study To Assess The Effect of Chewing Stick and Toothbrush On Oral Hygiene and Periodontal Status Among Indian PopulationVlad IliescuNo ratings yet
- SIGN 138 - Dental Interventions To Prevent Caries in ChildrenDocument52 pagesSIGN 138 - Dental Interventions To Prevent Caries in ChildrenayuNo ratings yet
- 1 s2.0 S0378874111005101 Main PDFDocument5 pages1 s2.0 S0378874111005101 Main PDFVlad IliescuNo ratings yet
- A Clinical Guide To OcclusionDocument75 pagesA Clinical Guide To OcclusionVlad Iliescu100% (1)
- Delivering Better Oral HealthDocument102 pagesDelivering Better Oral Healthsavrasx100% (1)
- New Classification of Perio DiseaseDocument5 pagesNew Classification of Perio DiseaseVlad IliescuNo ratings yet
- Vertebral LevelsDocument3 pagesVertebral LevelsSheikha100% (4)
- Anatomy of The Face and Neck: Peter M. PrendergastDocument18 pagesAnatomy of The Face and Neck: Peter M. PrendergastPaul SalahoruNo ratings yet
- Form EEA PR Guidance Notes v3Document40 pagesForm EEA PR Guidance Notes v3Vlad IliescuNo ratings yet
- Radiographic Steps For NotesDocument2 pagesRadiographic Steps For NotesVlad IliescuNo ratings yet
- 005 15853ns1103 32 40Document9 pages005 15853ns1103 32 40Vlad IliescuNo ratings yet
- Residence CardDocument85 pagesResidence CardMargit NagyNo ratings yet
- BSP - BPE GuidelinesDocument2 pagesBSP - BPE GuidelinesVlad IliescuNo ratings yet
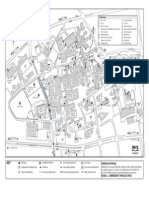
- Foresterhill: Health CampusDocument0 pagesForesterhill: Health CampusVlad IliescuNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Peaphy Week 3 - Activity 1 - Group 2Document3 pagesPeaphy Week 3 - Activity 1 - Group 2John Paul DioneoNo ratings yet
- Neurology & Pupils (No 467)Document231 pagesNeurology & Pupils (No 467)Mohamed GaberNo ratings yet
- 10 Muscular System Gross AnatomyDocument50 pages10 Muscular System Gross Anatomyvladu2004100% (1)
- The Sensitivity of The Bielschowsky Head-Tilt Test in Diagnosing Acquired Bilateral Superior Oblique ParesisDocument10 pagesThe Sensitivity of The Bielschowsky Head-Tilt Test in Diagnosing Acquired Bilateral Superior Oblique ParesisAnonymous mvNUtwidNo ratings yet
- Invitation To Health 17th Edition Hales Test BankDocument28 pagesInvitation To Health 17th Edition Hales Test Bankeelgrassbegum7pxg100% (21)
- Lange Ophthalmology Chapter 12. Strabismus : Print Close WindowDocument7 pagesLange Ophthalmology Chapter 12. Strabismus : Print Close Windowdhinesszone_88No ratings yet
- Pig EyeDocument6 pagesPig Eyeaims_sluNo ratings yet
- Extraocular Muscle InnervationDocument1 pageExtraocular Muscle InnervationRiski SudaenyNo ratings yet
- The Sclera - Maite Sainz de La MazaDocument331 pagesThe Sclera - Maite Sainz de La MazaDulnerio SengoNo ratings yet
- Full Download Personal Development For Life and Work 10th Edition Masters Test BankDocument28 pagesFull Download Personal Development For Life and Work 10th Edition Masters Test Bankjosephng4destNo ratings yet
- Feedback on extraocular muscle anatomyDocument21 pagesFeedback on extraocular muscle anatomyOscar Daniel MendezNo ratings yet
- ماكزلو3Document16 pagesماكزلو3haidergamer658No ratings yet
- Ophthalmology For The Primary Care PhysicianDocument393 pagesOphthalmology For The Primary Care PhysicianCatana TudorNo ratings yet
- Inferior Oblique MuscleDocument6 pagesInferior Oblique MuscleYunita ManurungNo ratings yet
- Osama’s Ophthalmology NotesDocument127 pagesOsama’s Ophthalmology NotesMd. Abdullah Rumman100% (1)
- About Cervicogenic Headache .... Imp.Document20 pagesAbout Cervicogenic Headache .... Imp.pervinkumarNo ratings yet
- SupsDocument3 pagesSupsasdfasdfawefawefNo ratings yet
- Dwnload Full Thomas Calculus 13th Edition Thomas Solutions Manual PDFDocument29 pagesDwnload Full Thomas Calculus 13th Edition Thomas Solutions Manual PDFtextury.exarchhz1nm8100% (12)
- Anatomy of The Eye and Orbit The Clinical EssentialsDocument687 pagesAnatomy of The Eye and Orbit The Clinical EssentialsDamian Torres SperanzaNo ratings yet
- Full Download Graphical Approach To College Algebra 6th Edition Hornsby Solutions ManualDocument29 pagesFull Download Graphical Approach To College Algebra 6th Edition Hornsby Solutions Manualyive.sweepsaw96u7t100% (26)
- Extraocular Muscle Anatomy and Physiology NotesDocument13 pagesExtraocular Muscle Anatomy and Physiology NotesRahul Jasu100% (1)
- Anatomy of Eye AppendigesDocument19 pagesAnatomy of Eye AppendigesSiyaNo ratings yet
- Dwnload Full Dynamic Business Law 4th Edition Kubasek Test Bank PDFDocument28 pagesDwnload Full Dynamic Business Law 4th Edition Kubasek Test Bank PDFantiquateouterlyhxhkwv100% (15)
- Eye Muscle Anatomy and FunctionsDocument35 pagesEye Muscle Anatomy and Functionswilliam williamNo ratings yet
- Some Aspects of Paralytic StrabismusDocument3 pagesSome Aspects of Paralytic StrabismusirijoaNo ratings yet
- S4 - Ojo FisiologiaDocument6 pagesS4 - Ojo FisiologiaLUIS FERNANDO MEZA GONZALESNo ratings yet
- Human Anatomy 9Th Edition Martini Test Bank Full Chapter PDFDocument60 pagesHuman Anatomy 9Th Edition Martini Test Bank Full Chapter PDFStevenAdkinsyjmd100% (6)
- Physical Exam of the Eye: Structures, Findings, DiagnosesDocument16 pagesPhysical Exam of the Eye: Structures, Findings, DiagnosesriveliNo ratings yet
- Management Information Systems Managing The Digital Firm 14th Edition Laudon Solutions ManualDocument29 pagesManagement Information Systems Managing The Digital Firm 14th Edition Laudon Solutions Manualgiaocleopatra192y100% (16)
- Anatomi 1Document82 pagesAnatomi 1Gek NissaNo ratings yet