You might also like
- Ankle Practical CRFDocument8 pagesAnkle Practical CRFapi-640939939No ratings yet
- PE Cases Part 1Document15 pagesPE Cases Part 1Kylie YuNo ratings yet
- Sharpen The Saw - Activity WorksheetDocument6 pagesSharpen The Saw - Activity WorksheetClarence Tan100% (1)
- Study Guide Questions: 9.4: Assessment, 6Document7 pagesStudy Guide Questions: 9.4: Assessment, 6api-502504563No ratings yet
- Study Guide Questions: 9.4: Magee D, Edition (2014), Page 759-759 Provided As An ExemplarDocument9 pagesStudy Guide Questions: 9.4: Magee D, Edition (2014), Page 759-759 Provided As An Exemplarapi-479716004No ratings yet
- PCP Weekly Questions WK 9Document6 pagesPCP Weekly Questions WK 9api-502171898No ratings yet
- Week 3 Portfolio QuestionsDocument5 pagesWeek 3 Portfolio Questionsapi-479716004No ratings yet
- Case 2: Ask The Questions About What Pain Activity Causes The Pain?Document8 pagesCase 2: Ask The Questions About What Pain Activity Causes The Pain?api-479717740No ratings yet
- Exam HipDocument14 pagesExam HipsingwongcsNo ratings yet
- Week 1 Portfolios QuestionsDocument7 pagesWeek 1 Portfolios Questionsapi-479716004No ratings yet
- Pth636-Case6 With FeedbackDocument2 pagesPth636-Case6 With Feedbackapi-619891965No ratings yet
- Week 4 Case 4 Chir13009Document6 pagesWeek 4 Case 4 Chir13009api-502504563No ratings yet
- Aman Case Presentation (MPT)Document36 pagesAman Case Presentation (MPT)Aman hussainNo ratings yet
- Lec7 Assessment of SpineDocument35 pagesLec7 Assessment of Spinesana mumtazNo ratings yet
- Schuster AthleticPelvisDocument26 pagesSchuster AthleticPelvisTheScribbl3rNo ratings yet
- Student Hip 2015Document8 pagesStudent Hip 2015Anonymous JhEds4No ratings yet
- Low Back Pain Lapkas 2Document27 pagesLow Back Pain Lapkas 2rini najoanNo ratings yet
- Case Study 3 Chiro 2020Document4 pagesCase Study 3 Chiro 2020api-479783350No ratings yet
- EPN Session 7Document9 pagesEPN Session 7Muhammmad RozakhNo ratings yet
- Week 7 QuestionsDocument9 pagesWeek 7 Questionsapi-502504563No ratings yet
- Facet Related Interventions Who, When and Where: Dr.D.K. BahetiDocument40 pagesFacet Related Interventions Who, When and Where: Dr.D.K. BahetineareastspineNo ratings yet
- Week 1 Case 1: Ben Presenting ComplaintDocument7 pagesWeek 1 Case 1: Ben Presenting Complaintapi-479754549No ratings yet
- Week 3 PCP Q ADocument5 pagesWeek 3 PCP Q Aapi-477982644No ratings yet
- CHIR12007 Clinical Assessment and Diagnosis Portfolio Exercises Week 5Document4 pagesCHIR12007 Clinical Assessment and Diagnosis Portfolio Exercises Week 5api-479849199No ratings yet
- Case Record 01 PDFDocument11 pagesCase Record 01 PDFNuwan KonaraNo ratings yet
- HW4A SpineDocument3 pagesHW4A SpineMary StrangeNo ratings yet
- Case StudyDocument6 pagesCase StudyMurad KurdiNo ratings yet
- OSCE Memorandum 2017Document15 pagesOSCE Memorandum 2017Natalie HuiNo ratings yet
- Week 4 Case 4 Chir13009Document9 pagesWeek 4 Case 4 Chir13009api-479720222No ratings yet
- Lower Extremity Amputation #8Document7 pagesLower Extremity Amputation #8Mary StrangeNo ratings yet
- Cervical Radiculopathy With Neurological DeficitDocument5 pagesCervical Radiculopathy With Neurological DeficitHager salaNo ratings yet
- Exercise 1Document6 pagesExercise 1api-455408952No ratings yet
- Lumbar Facet Syndrome - BogdukDocument8 pagesLumbar Facet Syndrome - BogdukSamSchroetkeNo ratings yet
- Week 1 Weekly QuestionsDocument6 pagesWeek 1 Weekly Questionsapi-502171898No ratings yet
- LL UL Musculoskeletal PE - PVD Varicose Veins ENT Headache PE PDFDocument187 pagesLL UL Musculoskeletal PE - PVD Varicose Veins ENT Headache PE PDFKalashini SenadheeraNo ratings yet
- Case HistoriesDocument5 pagesCase HistoriesJohn DorNo ratings yet
- 2 Acute Shoulder Pain Diagnosis and ManagementDocument42 pages2 Acute Shoulder Pain Diagnosis and Managementmk78_inNo ratings yet
- PCP Week 1Document8 pagesPCP Week 1api-512652362No ratings yet
- Shoulder Clinical Reasoning WorksheetDocument11 pagesShoulder Clinical Reasoning Worksheetapi-707436383No ratings yet
- Short Case II: Jufri Febrianto, MDDocument16 pagesShort Case II: Jufri Febrianto, MDsingle_ladyNo ratings yet
- Week 6Document8 pagesWeek 6api-479499469No ratings yet
- Week 7 Case Study 7 Chir13009Document12 pagesWeek 7 Case Study 7 Chir13009api-468597987No ratings yet
- CASE STUDY AND QUESTIONS: To Be Completed by The 19 July Week 1 Case 1: Ben Presenting ComplaintDocument6 pagesCASE STUDY AND QUESTIONS: To Be Completed by The 19 July Week 1 Case 1: Ben Presenting Complaintapi-479499469No ratings yet
- Spine: HistoryDocument6 pagesSpine: HistorySham SundarNo ratings yet
- Shoulder Pain-Pemalang 18 Des 22Document65 pagesShoulder Pain-Pemalang 18 Des 22yaang yuliana ciptaNo ratings yet
- Case Study 1 Chiro 2020Document6 pagesCase Study 1 Chiro 2020api-479783350No ratings yet
- Anterior Shoulder Pain: What Questions Would You Ask in The Subjective Examination?Document3 pagesAnterior Shoulder Pain: What Questions Would You Ask in The Subjective Examination?Kanwal KhanNo ratings yet
- Lab Guide: Musculoskeletal AssessmentDocument6 pagesLab Guide: Musculoskeletal AssessmentDaisy MellaNo ratings yet
- 3 Back and Joints March 2011Document19 pages3 Back and Joints March 2011suaqaziNo ratings yet
- Guide to Lower Back Pain Causes and Treatments (LBPDocument44 pagesGuide to Lower Back Pain Causes and Treatments (LBPMohammed Saad NabhanNo ratings yet
- Week 9 - PCPDocument7 pagesWeek 9 - PCPapi-479754549No ratings yet
- 221005-Z2 Juan Pieere Rep1 FHDocument4 pages221005-Z2 Juan Pieere Rep1 FHPieere M. AguilarNo ratings yet
- CASE STUDY AND QUESTIONS: To Be Completed by The 9th August Week 4: Case 4: AmberDocument7 pagesCASE STUDY AND QUESTIONS: To Be Completed by The 9th August Week 4: Case 4: Amberapi-479499469No ratings yet
- MSK 2 Case StudyDocument8 pagesMSK 2 Case StudyYumi KaitoNo ratings yet
- History NewDocument46 pagesHistory NewSaryia JavedNo ratings yet
- Week 7 Case Study 7 Chir13009 Tutors Notes 1Document10 pagesWeek 7 Case Study 7 Chir13009 Tutors Notes 1api-502171898No ratings yet
- Examination of The Lumbosacral SpineDocument28 pagesExamination of The Lumbosacral SpinepritishitiNo ratings yet
- Exam KneeDocument11 pagesExam KneesingwongcsNo ratings yet
- Week 4 Case 4 Chir13009 Tutors NotesDocument10 pagesWeek 4 Case 4 Chir13009 Tutors Notesapi-502171898No ratings yet
- A Simple Guide to Popliteal Muscle Tear, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Popliteal Muscle Tear, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Correct Your Pelvis and Heal your Back-Pain: The Self-Help Manual for Alleviating Back-Pain and other Musculo-Skeletal Aches and PainsFrom EverandCorrect Your Pelvis and Heal your Back-Pain: The Self-Help Manual for Alleviating Back-Pain and other Musculo-Skeletal Aches and PainsNo ratings yet
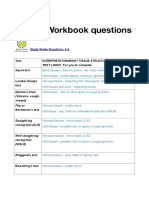
- Week 8 PCP Workbook QsDocument2 pagesWeek 8 PCP Workbook Qsapi-479849199No ratings yet
- Referral Letter cp2Document1 pageReferral Letter cp2api-479849199No ratings yet
- Portfolio Rubric 2020 Assessment 1Document3 pagesPortfolio Rubric 2020 Assessment 1api-479849199No ratings yet
- Portfolio Chir13008 - Assessment 1 Submission Addendum Form 2020 1Document2 pagesPortfolio Chir13008 - Assessment 1 Submission Addendum Form 2020 1api-479849199No ratings yet
- Week 10 PCP Workbook QsDocument4 pagesWeek 10 PCP Workbook Qsapi-479849199No ratings yet
- Week 5 PCP Workbook QsDocument3 pagesWeek 5 PCP Workbook Qsapi-479849199No ratings yet
- Week 6 PCP Workbook QsDocument6 pagesWeek 6 PCP Workbook Qsapi-479849199No ratings yet
- Week 7 PCP Workbook QsDocument2 pagesWeek 7 PCP Workbook Qsapi-479849199No ratings yet
- Week 4 PCP Workbook QsDocument6 pagesWeek 4 PCP Workbook Qsapi-479849199No ratings yet
- Shannonharrison 12062057 Reflection PCP ClustergroupvideoDocument4 pagesShannonharrison 12062057 Reflection PCP Clustergroupvideoapi-479849199No ratings yet
- Week 3 PCP Workbook QsDocument2 pagesWeek 3 PCP Workbook Qsapi-479849199No ratings yet
- Week 2 PCP Workbook QsDocument2 pagesWeek 2 PCP Workbook Qsapi-479849199No ratings yet
- Condition Differential Diagnosis/s DifferentiationDocument4 pagesCondition Differential Diagnosis/s Differentiationapi-479849199No ratings yet
- Shannonharrison 12062057 Reference List PCP ClustergroupvideoDocument3 pagesShannonharrison 12062057 Reference List PCP Clustergroupvideoapi-479849199No ratings yet
- Self-Directed LearningDocument3 pagesSelf-Directed Learningapi-479849199No ratings yet
- Exercise 1: CHIR12007 Clinical Assessment and Diagnosis Portfolio Exercises Week 7Document4 pagesExercise 1: CHIR12007 Clinical Assessment and Diagnosis Portfolio Exercises Week 7api-479720222No ratings yet
- Exercise 1Document4 pagesExercise 1api-479849199No ratings yet
- 4Document5 pages4api-479849199No ratings yet
- CHIR12007 Clinical Assessment and Diagnosis Portfolio Exercises Week 5Document4 pagesCHIR12007 Clinical Assessment and Diagnosis Portfolio Exercises Week 5api-479849199No ratings yet
- Shift Manager ResumeDocument2 pagesShift Manager ResumeAbdul NaeemNo ratings yet
- SINP International Skilled Workers: Expression of Interest (EOI) Selection ResultsDocument14 pagesSINP International Skilled Workers: Expression of Interest (EOI) Selection ResultsSaquib.MahmoodNo ratings yet
- Effective Leadership Theory Cases and Applications 1st Edition Humphrey Test BankDocument9 pagesEffective Leadership Theory Cases and Applications 1st Edition Humphrey Test Bankhillyobsidian8hi42g100% (36)
- Full Download Test Bank For The Sociology of Health Illness and Health Care A Critical Approach 7th Edition PDF Full ChapterDocument35 pagesFull Download Test Bank For The Sociology of Health Illness and Health Care A Critical Approach 7th Edition PDF Full Chapterforceepipubica61uxl95% (21)
- Nurses' disaster response competencies at health centers in Bireuen District, AcehDocument15 pagesNurses' disaster response competencies at health centers in Bireuen District, AcehWahyu HidayatiNo ratings yet
- NASKAH-PUBLIKASI (1) Nanot HalamanDocument13 pagesNASKAH-PUBLIKASI (1) Nanot HalamanNurul FitrianiNo ratings yet
- Conduct Disorder and Somatic Health in ChildrenDocument3 pagesConduct Disorder and Somatic Health in ChildrenJeric C. ManaliliNo ratings yet
- Daily Plan of Activities For High Risk OBDocument6 pagesDaily Plan of Activities For High Risk OBJR Rolf NeuqeletNo ratings yet
- Abstract of ThesisDocument2 pagesAbstract of ThesisdrkartikeytyagiNo ratings yet
- College of Liberal Arts University of LuzonDocument9 pagesCollege of Liberal Arts University of LuzonChristianne Joyse MerreraNo ratings yet
- BS BuzzDocument10 pagesBS BuzzBS Central, Inc. "The Buzz"No ratings yet
- Researchgate publication on delayed tooth eruptionDocument7 pagesResearchgate publication on delayed tooth eruptionResgitanadila MasyaNo ratings yet
- WKF Para-Karate Kata Competition RulesDocument14 pagesWKF Para-Karate Kata Competition RulesMohamad IbrahimNo ratings yet
- Understanding Borderline Personality DisorderDocument59 pagesUnderstanding Borderline Personality Disorderaakash atteguppeNo ratings yet
- MOM GA Transport & QAQC CoordinationDocument2 pagesMOM GA Transport & QAQC CoordinationErik EstradaNo ratings yet
- LP Trauma Kapitis PDFDocument29 pagesLP Trauma Kapitis PDFPajoNo ratings yet
- Training and DevelopmentDocument2 pagesTraining and DevelopmentBeing Rohit ThakurNo ratings yet
- Contemporary World Exemplar T L ModuleDocument111 pagesContemporary World Exemplar T L ModuleChrizelle Mae Rodriguez100% (1)
- Barriers To ListeningDocument2 pagesBarriers To ListeningHammad Ali ShahzadNo ratings yet
- 18.20.04 - BSSL Seafarers Health Self Declaration With COVID 19 Test And... (1) - 3Document3 pages18.20.04 - BSSL Seafarers Health Self Declaration With COVID 19 Test And... (1) - 3Dean IL RE JamesNo ratings yet
- Accomplishment Target For The Month of October C.Y. 2020Document16 pagesAccomplishment Target For The Month of October C.Y. 2020jamesdigolNo ratings yet
- UntitledDocument21 pagesUntitledYakoub AbdelliNo ratings yet
- Expected Coding and Decoding Questions For Ibps Po MainsDocument11 pagesExpected Coding and Decoding Questions For Ibps Po Mainsvirat kohli86% (7)
- Professional Teachers (Secondary) 10-2022 FilipinoDocument26 pagesProfessional Teachers (Secondary) 10-2022 FilipinoPRC Baguio100% (1)
- Selcoperm SES 125-2000 Electrochlorinator: Installation and Operating InstructionsDocument32 pagesSelcoperm SES 125-2000 Electrochlorinator: Installation and Operating InstructionsNorbert MeyerNo ratings yet
- Professional Hypnotherapist Diploma For Stress CourseDocument53 pagesProfessional Hypnotherapist Diploma For Stress CourseLuis Del Valle Torregrosa100% (1)
- Libro Letsgo - B1 PolitécnicoDocument172 pagesLibro Letsgo - B1 Politécnicolino.cambron.munNo ratings yet
- Vocab 2Document2 pagesVocab 2api-245567970No ratings yet
- Grade 11 - Final Exam PDDocument3 pagesGrade 11 - Final Exam PDGomez Agustin LeslieNo ratings yet