You might also like
- Ni Hms 892467Document17 pagesNi Hms 892467jindgi23No ratings yet
- Case Definition and Culture Are People All The SameDocument3 pagesCase Definition and Culture Are People All The SameDiana BNo ratings yet
- Papers Sds JournalDocument18 pagesPapers Sds Journalfatimasaeed2772No ratings yet
- The Emotional Pain and Distress of Borderline Personality DisorderDocument9 pagesThe Emotional Pain and Distress of Borderline Personality Disorderme13No ratings yet
- Cultural Distress Complex PTSDDocument14 pagesCultural Distress Complex PTSDCesia Constanza Leiva GonzalezNo ratings yet
- Anthropology, Expressed Emotion, and Outcomes in SchizophreniaDocument46 pagesAnthropology, Expressed Emotion, and Outcomes in Schizophreniaphilia0207No ratings yet
- A Review of The Korean Cultural Syndrome Hwa-ByungDocument18 pagesA Review of The Korean Cultural Syndrome Hwa-Byungkashyapi thakuriaNo ratings yet
- PA en Depresión en Irán 2018Document7 pagesPA en Depresión en Irán 2018Alfredo PérezNo ratings yet
- HHS Public AccessDocument27 pagesHHS Public Accessbob antonioNo ratings yet
- ACross CulturalTestoftheTraumaModelofDissociation2Document24 pagesACross CulturalTestoftheTraumaModelofDissociation2Fulop NoemiNo ratings yet
- Negative Thoughts in Depression: A Study in IranDocument7 pagesNegative Thoughts in Depression: A Study in IranAnonymous tIwg2AyNo ratings yet
- DSM-5 and Culture - The Need To Move Towards A Shared Model of Care Within A More Equal Patient-Physician PartnershipDocument3 pagesDSM-5 and Culture - The Need To Move Towards A Shared Model of Care Within A More Equal Patient-Physician PartnershipPearl SkyNo ratings yet
- Religious Healing Practices and Their Ethical ImplicationsDocument19 pagesReligious Healing Practices and Their Ethical ImplicationsChau Minh TrietNo ratings yet
- Low - 1981 - The Meaning of Nervios A Sociocultural Analysis oDocument23 pagesLow - 1981 - The Meaning of Nervios A Sociocultural Analysis oLaura PalermoNo ratings yet
- Racism and Mental Health and The Role of Mental Health ProfessionalsDocument8 pagesRacism and Mental Health and The Role of Mental Health ProfessionalsDaniel MNo ratings yet
- Culture and PTSD: Trauma in Global and Historical PerspectiveFrom EverandCulture and PTSD: Trauma in Global and Historical PerspectiveNo ratings yet
- Effective Psychotherapy in A Racially and Culturally Diverse Society - Bhui & N MorganDocument8 pagesEffective Psychotherapy in A Racially and Culturally Diverse Society - Bhui & N MorgancaveolemuresNo ratings yet
- Valid Measurement of Trauma Among RefugeesDocument10 pagesValid Measurement of Trauma Among RefugeesSara SáNo ratings yet
- 19 Perceptions PDFDocument6 pages19 Perceptions PDFIJELS Research JournalNo ratings yet
- 1 s2.0 S0147176722000591 MainDocument10 pages1 s2.0 S0147176722000591 MainBianca ZupcauNo ratings yet
- Чувство себя - анорексияDocument23 pagesЧувство себя - анорексияNatalia KopyakovaNo ratings yet
- Boughton & Street (2007)Document11 pagesBoughton & Street (2007)hero holoNo ratings yet
- Chinese Conception of Mental Illness Comparative Culture AnalysisDocument8 pagesChinese Conception of Mental Illness Comparative Culture AnalysismutiahnisaNo ratings yet
- Chinese Conception of Mental Illness: A Comparative Culture AnalysisDocument8 pagesChinese Conception of Mental Illness: A Comparative Culture AnalysisKATERENo ratings yet
- Cross-Cultural Studies of Depression PDFDocument34 pagesCross-Cultural Studies of Depression PDFStiven Tovar ClarosNo ratings yet
- 2001 The Explanatory Models of Mental Health Amongst Low-Income Women and Health Care Practitioners in LusakaDocument8 pages2001 The Explanatory Models of Mental Health Amongst Low-Income Women and Health Care Practitioners in LusakaLuana SouzaNo ratings yet
- Cultural Differences in Emotions: A Context For Interpreting Emotional ExperiencesDocument16 pagesCultural Differences in Emotions: A Context For Interpreting Emotional ExperiencesRita1976No ratings yet
- Culture Bound Syndrome-An Unprecedented Inclusion: October 2017Document7 pagesCulture Bound Syndrome-An Unprecedented Inclusion: October 2017Turfa AhmedNo ratings yet
- David, E. J. R. (2008) - A Colonial Mentality Model of Depression For Filipino Americans.Document10 pagesDavid, E. J. R. (2008) - A Colonial Mentality Model of Depression For Filipino Americans.April TogononNo ratings yet
- Is Culture An Independent Variable in Psycho Geriatrics. The Case of Brazilian and Japanese ElderlyDocument4 pagesIs Culture An Independent Variable in Psycho Geriatrics. The Case of Brazilian and Japanese ElderlyGeriatric_NeurologyNo ratings yet
- Clifford Et Al Negative and Positive Emotional ComplexityDocument8 pagesClifford Et Al Negative and Positive Emotional ComplexityTim DalgleishNo ratings yet
- Guide to Psychological Assessment with HispanicsFrom EverandGuide to Psychological Assessment with HispanicsLorraine T. BenutoNo ratings yet
- Pyc1512 Unit 2Document21 pagesPyc1512 Unit 2maciabhenguNo ratings yet
- Multicultural Applications of CBTDocument7 pagesMulticultural Applications of CBTpaula_fariaNo ratings yet
- Relevance of Culture-Bound Syndromes in The 21st Century: Antonio Ventriglio,, Oyedeji Ayonrinde, and Dinesh BhugraDocument4 pagesRelevance of Culture-Bound Syndromes in The 21st Century: Antonio Ventriglio,, Oyedeji Ayonrinde, and Dinesh BhugraTurfa AhmedNo ratings yet
- Pii - 0037-7856 (76) 90074-3Document10 pagesPii - 0037-7856 (76) 90074-3Arokkiaraj HellerNo ratings yet
- Jong2013 Collective Trauma ProcessingDocument18 pagesJong2013 Collective Trauma ProcessingLuana SouzaNo ratings yet
- Expressed Emotion Across CulturesDocument7 pagesExpressed Emotion Across Culturesappaloosa.musicalNo ratings yet
- Grief MattersDocument3 pagesGrief MattersshNo ratings yet
- Coming To Our Senses:Appreciating The Sensorial in Medical AnthropologyDocument35 pagesComing To Our Senses:Appreciating The Sensorial in Medical AnthropologyTori SheldonNo ratings yet
- Abnormal Psychology - ReviewerDocument16 pagesAbnormal Psychology - ReviewerVanessa GabonNo ratings yet
- Cultural Influences On Pain: Mrs Sue Peacock and Mrs Shilpa PatelDocument4 pagesCultural Influences On Pain: Mrs Sue Peacock and Mrs Shilpa PatelNugi PsNo ratings yet
- Depression and Gender: An International ReviewDocument7 pagesDepression and Gender: An International ReviewDeadly ChillerNo ratings yet
- 2017 Moreira-Almeida Methodological Guidelines To Investigate Anomalous ExperiencesDocument11 pages2017 Moreira-Almeida Methodological Guidelines To Investigate Anomalous ExperiencesmarciascognamilloNo ratings yet
- Depression, Emotion and the Self: Philosophical and Interdisciplinary PerspectivesFrom EverandDepression, Emotion and the Self: Philosophical and Interdisciplinary PerspectivesNo ratings yet
- Review: Dissociative Trance and Spirit Possession Challenges For Cultures-In-TransitionDocument18 pagesReview: Dissociative Trance and Spirit Possession Challenges For Cultures-In-TransitionSAMADHI FERNANDO SALGUERO SILESNo ratings yet
- Kleinman, Suffering and Its Professional TransformationDocument18 pagesKleinman, Suffering and Its Professional Transformationrachel.avivNo ratings yet
- Affective Disorders in Cultural Context: Laurence Kirmayer, and Danielle Groleau, PHDDocument14 pagesAffective Disorders in Cultural Context: Laurence Kirmayer, and Danielle Groleau, PHDvarhanNo ratings yet
- Psychological Healing: Historical and Philosophical Foundations of Professional PsychologyFrom EverandPsychological Healing: Historical and Philosophical Foundations of Professional PsychologyNo ratings yet
- Somatoform and Other Psychosomatic Disorders: A Dialogue Between Contemporary Psychodynamic Psychotherapy and Cognitive Behavioral Therapy PerspectivesFrom EverandSomatoform and Other Psychosomatic Disorders: A Dialogue Between Contemporary Psychodynamic Psychotherapy and Cognitive Behavioral Therapy PerspectivesChristos CharisNo ratings yet
- Fpsyt 14 1148170Document10 pagesFpsyt 14 1148170Alexa Ramírez ContrerasNo ratings yet
- Emotional Expressivity Predict Somatization 2018Document1 pageEmotional Expressivity Predict Somatization 2018h.kaviani88No ratings yet
- BetenskyDocument8 pagesBetenskyangeln0bleNo ratings yet
- Depression Anxiety Stress ScaleDocument29 pagesDepression Anxiety Stress ScaleBonita Asyigah0% (1)
- Subtipo SensorialDocument21 pagesSubtipo SensorialRosa Fonseca AguloNo ratings yet
- The Lay Concept of Mental Disorder A Cross-CultuDocument18 pagesThe Lay Concept of Mental Disorder A Cross-CultuAmritha V RaoNo ratings yet
- Hearing Voices: Qualitative Inquiry in Early PsychosisFrom EverandHearing Voices: Qualitative Inquiry in Early PsychosisNo ratings yet
- Multinomial Logistic Regression Basic RelationshipsDocument73 pagesMultinomial Logistic Regression Basic RelationshipslibremdNo ratings yet
- Zhang 2019 Plos NTDDocument20 pagesZhang 2019 Plos NTDlibremdNo ratings yet
- Arif 2017 Plos OneDocument19 pagesArif 2017 Plos OnelibremdNo ratings yet
- Zing 2018 Int HealthDocument8 pagesZing 2018 Int HealthlibremdNo ratings yet
- Cloete 2018 Scielo South AfricaDocument10 pagesCloete 2018 Scielo South AfricalibremdNo ratings yet
- Nguyen Minh Tuan 2013Document8 pagesNguyen Minh Tuan 2013libremdNo ratings yet
- Curriculum Vitae Ladson Hinton Personal Information: Lwhinton@ucdavis - EduDocument34 pagesCurriculum Vitae Ladson Hinton Personal Information: Lwhinton@ucdavis - EdulibremdNo ratings yet
- Boukary 2012 Plos OneDocument12 pagesBoukary 2012 Plos OnelibremdNo ratings yet
- Questions To Integrate A Gender Perspective Into Research CooperationDocument3 pagesQuestions To Integrate A Gender Perspective Into Research CooperationlibremdNo ratings yet
- 2017smart Watch CatalogDocument2 pages2017smart Watch CataloglibremdNo ratings yet
- Ensayos Clinicos PDFDocument51 pagesEnsayos Clinicos PDFlibremdNo ratings yet
- Eng PDFDocument52 pagesEng PDFlibremdNo ratings yet
- Quality of Life in Patients With Cutaneous LeishmaniasisDocument4 pagesQuality of Life in Patients With Cutaneous LeishmaniasislibremdNo ratings yet
- Tesis AlirezaDocument98 pagesTesis AlirezalibremdNo ratings yet
- No Woman Should Die Giving LifeDocument112 pagesNo Woman Should Die Giving LifelibremdNo ratings yet
- Nutrition Transition in 2 Lowland Bolivian Subsistence PopulationsDocument13 pagesNutrition Transition in 2 Lowland Bolivian Subsistence PopulationslibremdNo ratings yet
- Lec02 FramingTheQuestion Sec BDocument9 pagesLec02 FramingTheQuestion Sec BCharlie CaceresNo ratings yet
- Thesis+2016 - Nada AmroussiaDocument62 pagesThesis+2016 - Nada AmroussialibremdNo ratings yet
- Cineforum 2017: Director: Davis GuggenheimDocument1 pageCineforum 2017: Director: Davis GuggenheimlibremdNo ratings yet
- Clinical Dementia Rating Worksheet: Memory Questions For InformantDocument10 pagesClinical Dementia Rating Worksheet: Memory Questions For InformantlibremdNo ratings yet
- Personal and Political Histories in The Designing of Health ReformDocument8 pagesPersonal and Political Histories in The Designing of Health ReformlibremdNo ratings yet
- Trumble Etal 2015 JGDocument7 pagesTrumble Etal 2015 JGlibremdNo ratings yet
- Tarea SocialesDocument4 pagesTarea SocialeslibremdNo ratings yet
- Trumble Etal 2015 JGDocument7 pagesTrumble Etal 2015 JGlibremdNo ratings yet
- Modelo Articulo Risk Factors StatisticsDocument7 pagesModelo Articulo Risk Factors StatisticslibremdNo ratings yet
- Fahetal2010 PDFDocument10 pagesFahetal2010 PDFlibremdNo ratings yet
- CDC Diagnosis Guide Leishmaniasis PDFDocument4 pagesCDC Diagnosis Guide Leishmaniasis PDFlibremdNo ratings yet
- Author FormDocument2 pagesAuthor FormlibremdNo ratings yet
- Altizer Et Al. 2013 Climate Disease PDFDocument7 pagesAltizer Et Al. 2013 Climate Disease PDFlibremdNo ratings yet
- Classical Conditioning and Operant Conditioning A Response Pattern Analysis (Prikom) PDFDocument365 pagesClassical Conditioning and Operant Conditioning A Response Pattern Analysis (Prikom) PDFNeysa Rekanidya Avianny100% (1)
- The Empathetic SchoolDocument9 pagesThe Empathetic SchoolLisbeth RamosOrtegaNo ratings yet
- The Psychology of EmotionsDocument60 pagesThe Psychology of Emotionskunal arenNo ratings yet
- Observation ChartDocument4 pagesObservation ChartFloortime Repository100% (1)
- Business Communication NotesDocument214 pagesBusiness Communication NotesAnonymous xpdTqv100% (1)
- Stress Relief with Emotional Freedom TechniqueDocument2 pagesStress Relief with Emotional Freedom TechniquesimasNo ratings yet
- (Northwestern University Press Studies in Russian Literature and Theory) Dostoïevski, Fedor Mikhailovitch_Dostoyevsky, Fyodor_Gogolʹ, Nikolaĭ Vasilʹevich_Gogol, Nikolaï Vasilievitch_Porter, Jillian_PoDocument211 pages(Northwestern University Press Studies in Russian Literature and Theory) Dostoïevski, Fedor Mikhailovitch_Dostoyevsky, Fyodor_Gogolʹ, Nikolaĭ Vasilʹevich_Gogol, Nikolaï Vasilievitch_Porter, Jillian_PoPedro MedeiNo ratings yet
- ErminaDocument32 pagesErminaMichael John Canare GloriaNo ratings yet
- Art Appreciation Self-Instructional Module - Weeks 2-4 Lesson 1Document14 pagesArt Appreciation Self-Instructional Module - Weeks 2-4 Lesson 1Angelica Rose Ponte100% (1)
- Evolutionary Psychology Fashionable Ideology or New FoundationDocument13 pagesEvolutionary Psychology Fashionable Ideology or New FoundationTauily TaunayNo ratings yet
- Nishant Audit Course ReportDocument19 pagesNishant Audit Course ReportNishant KhandharNo ratings yet
- Aura Chakra Soma (Em Ingles)Document8 pagesAura Chakra Soma (Em Ingles)CHAKRA5100% (1)
- Curatorial Rationale 1Document1 pageCuratorial Rationale 1api-351218907No ratings yet
- Kövecses EmotionconceptsDocument46 pagesKövecses Emotionconceptsivana иванаNo ratings yet
- Neuropsychologia: Maor Zeev-Wolf, Yuri RassovskyDocument8 pagesNeuropsychologia: Maor Zeev-Wolf, Yuri RassovskytratrNo ratings yet
- 7 Secrets From Ancient Wisdom For Anger ManagementDocument21 pages7 Secrets From Ancient Wisdom For Anger ManagementKanjaFitNo ratings yet
- (KMF1014) Assignment 3 by Group 3Document16 pages(KMF1014) Assignment 3 by Group 3Nur Sabrina AfiqahNo ratings yet
- Luis Jr. Amatosa - Priciples Module 1Document8 pagesLuis Jr. Amatosa - Priciples Module 1Luis Santos Amatosa Jr.No ratings yet
- 2021dmzself CareDocument32 pages2021dmzself CareRose GutierrezNo ratings yet
- Spontaneous Activity in Education by Montessori, Maria, 1870-1952Document164 pagesSpontaneous Activity in Education by Montessori, Maria, 1870-1952Gutenberg.org100% (5)
- Artigo - A Focusing-Oriented Approach Couples TherapyDocument16 pagesArtigo - A Focusing-Oriented Approach Couples TherapyGabriel RochaNo ratings yet
- Reading 1 Reading Comprehension Exercises 100187Document1 pageReading 1 Reading Comprehension Exercises 100187Al-Farisi Wisanggeni CigadingNo ratings yet
- 10 Keys To HappinessDocument3 pages10 Keys To HappinessJanieNo ratings yet
- Innovation Radar 2Document12 pagesInnovation Radar 2andsaitoNo ratings yet
- AFASES 2016: Case Study of Child Sexual AbuseDocument6 pagesAFASES 2016: Case Study of Child Sexual AbuseAzlin IdayuNo ratings yet
- Psychosocial Perspectives on Gender and SexualityDocument27 pagesPsychosocial Perspectives on Gender and SexualityHector CandidoNo ratings yet
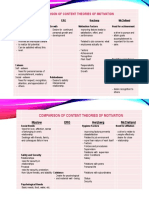
- COMPARISON OF MOTIVATION THEORIESDocument2 pagesCOMPARISON OF MOTIVATION THEORIESMelNo ratings yet
- Lesson 04Document9 pagesLesson 04gyanaspiritualproductsNo ratings yet
- PR Chapter 1-5 Tangina Natapos ManDocument53 pagesPR Chapter 1-5 Tangina Natapos ManErni LatogaNo ratings yet
- Approaches of CunsellingDocument5 pagesApproaches of CunsellingNelson Grande CalimagNo ratings yet