You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Seminar On Skilled Birth SBA ModuleDocument50 pagesSeminar On Skilled Birth SBA ModuleSangita Patir83% (40)
- Research Essay Riley Henning 2Document12 pagesResearch Essay Riley Henning 2api-509444264No ratings yet
- Maternity Exam 2Document56 pagesMaternity Exam 2Johanna Erazo Padilla80% (10)
- GD PMHDocument14 pagesGD PMHClareen JuanicoNo ratings yet
- How Do You Perform A Proper Physical Examination of The Breast?Document2 pagesHow Do You Perform A Proper Physical Examination of The Breast?Clareen JuanicoNo ratings yet
- And Vaginal Bleeding (In Ruptured Ectopic Pregnancy)Document9 pagesAnd Vaginal Bleeding (In Ruptured Ectopic Pregnancy)Clareen JuanicoNo ratings yet
- Abruptio Placentae: Insert or Drag & Drop Your PhotoDocument42 pagesAbruptio Placentae: Insert or Drag & Drop Your PhotoClareen JuanicoNo ratings yet
- Histological Diagnosis of Hydatidiform Moles: Histological Changes of Complete and Partial Moles AreDocument8 pagesHistological Diagnosis of Hydatidiform Moles: Histological Changes of Complete and Partial Moles AreClareen JuanicoNo ratings yet
- AtonyDocument3 pagesAtonyClareen JuanicoNo ratings yet
- Breast FeedingDocument5 pagesBreast FeedingClareen JuanicoNo ratings yet
- Pre Natal CareDocument4 pagesPre Natal CareClareen JuanicoNo ratings yet
- As Transient Hypertension If Evidence For Preeclampsia Does Not Develop and The Blood Pressure Returns To Normal by 12 Weeks PostpartumDocument5 pagesAs Transient Hypertension If Evidence For Preeclampsia Does Not Develop and The Blood Pressure Returns To Normal by 12 Weeks PostpartumClareen JuanicoNo ratings yet
- Juanico, Clareen Mae (Assignment)Document3 pagesJuanico, Clareen Mae (Assignment)Clareen JuanicoNo ratings yet
- B. Meckel's DiverticulumDocument3 pagesB. Meckel's DiverticulumClareen JuanicoNo ratings yet
- Puerperium: Striae GravidarumDocument5 pagesPuerperium: Striae GravidarumClareen JuanicoNo ratings yet
- Hysteroscopy Newsletter Vol 6 Issue 3 EnglishDocument21 pagesHysteroscopy Newsletter Vol 6 Issue 3 EnglishHisteroscopia.esNo ratings yet
- Developmental GeneticsDocument18 pagesDevelopmental Geneticsyuyu tuptupNo ratings yet
- NIC - Betacyanin To Semen SmearDocument6 pagesNIC - Betacyanin To Semen SmearNicole Jane RobesNo ratings yet
- Counseling For Family PlanningDocument90 pagesCounseling For Family PlanningShang DimolNo ratings yet
- Moral Issue Part 1 - EthicsDocument2 pagesMoral Issue Part 1 - EthicsJermain Liam EscuderoNo ratings yet
- LIFS 1902 - General Biology II: Video 4 - Human DevelopmentDocument20 pagesLIFS 1902 - General Biology II: Video 4 - Human DevelopmentGary TsangNo ratings yet
- Sperm A ToDocument16 pagesSperm A TogfujawatiNo ratings yet
- Jordie-Prenatal Care StudygramDocument7 pagesJordie-Prenatal Care StudygramNoreen Hannah GabrielNo ratings yet
- 6 Psychological Aspects of Perinatal Los PDFDocument11 pages6 Psychological Aspects of Perinatal Los PDFJa CorbatoNo ratings yet
- Leopolds Maneuver ChecklistDocument5 pagesLeopolds Maneuver ChecklistSheen CatayongNo ratings yet
- Case Press Ob WardDocument9 pagesCase Press Ob Wardjohn castroNo ratings yet
- Human Reproduction QuestionsDocument3 pagesHuman Reproduction QuestionsMohamed Mohammed50% (2)
- We Lived in The Gaps Between The Stories (2021) Lena ChenDocument4 pagesWe Lived in The Gaps Between The Stories (2021) Lena ChensaturnsaysNo ratings yet
- DR Maitri Chaudhuri: Fetal Echocardiography Scope & Future !Document28 pagesDR Maitri Chaudhuri: Fetal Echocardiography Scope & Future !merin sunilNo ratings yet
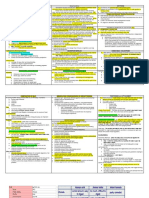
- Strategic Intervention MaterialDocument9 pagesStrategic Intervention MaterialHana Karudi100% (1)
- Placenta Types and GradingDocument37 pagesPlacenta Types and GradingNishant RajNo ratings yet
- GAD Plan Template NutritionDocument29 pagesGAD Plan Template NutritionAres ColeNo ratings yet
- Thesis ProtocolDocument11 pagesThesis ProtocolSuyajna JoshiNo ratings yet
- Case Report On The Effect of Virechana in Male Infertility W.S.R.T OligozoospermiaDocument4 pagesCase Report On The Effect of Virechana in Male Infertility W.S.R.T OligozoospermiaEditor IJTSRDNo ratings yet
- Elc231 Apr 2019 Mid-Sem Set 1Document8 pagesElc231 Apr 2019 Mid-Sem Set 1fatin nadiaNo ratings yet
- Quiz NCM107Document20 pagesQuiz NCM107MARC JOSHUA SARANILLONo ratings yet
- Animal Biotechnology For Livestock Production 3 Springer, 2023Document334 pagesAnimal Biotechnology For Livestock Production 3 Springer, 2023Gilbert MethewNo ratings yet
- Malaria Schematic DiagramDocument5 pagesMalaria Schematic DiagramCrazy about JunglesNo ratings yet
- Ways To Control Population GrowthDocument5 pagesWays To Control Population GrowthMarie TaylaranNo ratings yet
- Comprehensive Gynecology 8Th Edition David M Gershenson MD Full ChapterDocument67 pagesComprehensive Gynecology 8Th Edition David M Gershenson MD Full Chapterinez.garcia238100% (3)
- HysterosalpingographyDocument12 pagesHysterosalpingographyGita Chan0% (2)
- Science DLL q2w3Document5 pagesScience DLL q2w3ANGELBERT PEDNGA0% (1)