You might also like
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Ultimate Mega-Training in Real World Results Magick - Jason Louv - Magick - MeDocument11 pagesThe Ultimate Mega-Training in Real World Results Magick - Jason Louv - Magick - Mej mooreNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Test Bank For Human Resource Management 13th Edition MathisDocument33 pagesTest Bank For Human Resource Management 13th Edition MathisMitchellJohnsonktspj100% (35)
- H.3. GAMBOA V TEVESDocument1 pageH.3. GAMBOA V TEVESJuris Doctor 2BNo ratings yet
- 9706 International Accounting Standards (For Examination From 2023)Document58 pages9706 International Accounting Standards (For Examination From 2023)waheeda17100% (1)
- Entry Essay Worksheet For EAPPDocument1 pageEntry Essay Worksheet For EAPPRemryan R. RebutazoNo ratings yet
- Garden Rail - N°286 - 2018-06Document64 pagesGarden Rail - N°286 - 2018-06Valery GagichNo ratings yet
- Proposal SMS GatewayDocument16 pagesProposal SMS GatewayGian TasariNo ratings yet
- Guidance FormDocument1 pageGuidance FormCatherine TominNo ratings yet
- FS 101 Lesson 3 - Lesson 4Document4 pagesFS 101 Lesson 3 - Lesson 4Caye TVblogs75% (4)
- LABOR STANDARDS (Nolasco)Document13 pagesLABOR STANDARDS (Nolasco)Bob CasasolaNo ratings yet
- James Arthur (Singer)Document5 pagesJames Arthur (Singer)ancascribd00No ratings yet
- Toyotas Best-Cost Producer StrategyDocument3 pagesToyotas Best-Cost Producer StrategyYuri Alejandra Perdomo CuellarNo ratings yet
- Competition RulesDocument2 pagesCompetition RulesAbdul Hadi ParmanNo ratings yet
- ,'A Ew Ffiq,: Q ( (:-PR S D Qaqffi FT 3tim (Y P T Q 4I Ilia / Ffi QFL Ffil QRQLDocument9 pages,'A Ew Ffiq,: Q ( (:-PR S D Qaqffi FT 3tim (Y P T Q 4I Ilia / Ffi QFL Ffil QRQLAbhimanyu Yashwant AltekarNo ratings yet
- Shonazarova90@mail - Ru: Faculty: Management and Economics Law Specialization: Legal Affairs in Custom AffairsDocument3 pagesShonazarova90@mail - Ru: Faculty: Management and Economics Law Specialization: Legal Affairs in Custom AffairsMila BellucciNo ratings yet
- MANACCDocument12 pagesMANACCAllan Patrick AlsimNo ratings yet
- Griffin V Freddie Watts and Jimmy BrothersDocument6 pagesGriffin V Freddie Watts and Jimmy Brothersapi-459574692No ratings yet
- Instructions For VisitorsDocument5 pagesInstructions For VisitorsznmudzetNo ratings yet
- Fixedline and Broadband Services: Your Account Summary This Month'S ChargesDocument2 pagesFixedline and Broadband Services: Your Account Summary This Month'S ChargesBharat BhushanNo ratings yet
- My Book List - BooksDocument3 pagesMy Book List - BooksB34 Ankur SahaNo ratings yet
- Schumer's AI One PagerDocument1 pageSchumer's AI One PagerWashington ExaminerNo ratings yet
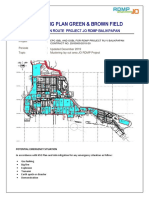
- Mustering Plan Area Green & Brown FieldDocument6 pagesMustering Plan Area Green & Brown FieldBimaNo ratings yet
- Judicial Control Administrative LawDocument12 pagesJudicial Control Administrative LawShailvi RajNo ratings yet
- About The Market: Market Size of Coca Cola's Competitors Are As FollowsDocument3 pagesAbout The Market: Market Size of Coca Cola's Competitors Are As FollowsPrateek AgrawalNo ratings yet
- Session 7Document18 pagesSession 7Digvijay SinghNo ratings yet
- Income TaxDocument60 pagesIncome TaxVaibhav GuptaNo ratings yet
- Account Details of AmialDocument13 pagesAccount Details of Amialarifur RahmanNo ratings yet
- 1 s2.0 S1877042815032371 MainDocument5 pages1 s2.0 S1877042815032371 Maincovid19 bebasNo ratings yet
- Rights of TransgenderDocument11 pagesRights of TransgenderAarti MaanNo ratings yet
- Pay It Forward Copy - EditedDocument3 pagesPay It Forward Copy - Editedgmeredith1968No ratings yet