You might also like
- Foot and Ankle Disability Index and Sports Module (FADI) PDFDocument2 pagesFoot and Ankle Disability Index and Sports Module (FADI) PDFFebryLasantiNo ratings yet
- Foot Function IndexDocument1 pageFoot Function IndexVALENNo ratings yet
- Teach Yourself ThoraxDocument29 pagesTeach Yourself ThoraxSambili Tonny100% (3)
- Twstrs ScalaDocument2 pagesTwstrs ScalaAlin Lin-LinNo ratings yet
- William Vs MC Kenzie-1Document4 pagesWilliam Vs MC Kenzie-1DefaNo ratings yet
- Nyeri Pada Tennis Elbow Tipe IIDocument14 pagesNyeri Pada Tennis Elbow Tipe IIlisaNo ratings yet
- Sop Muskulo (Tennis Elbow)Document15 pagesSop Muskulo (Tennis Elbow)Melissa Erjani Adam100% (2)
- Understanding the Underlying Process of Trauma and Its TreatmentDocument3 pagesUnderstanding the Underlying Process of Trauma and Its TreatmentannyNo ratings yet
- Skin Mechanical Properties - ArinSDocument26 pagesSkin Mechanical Properties - ArinSJack Flow ClickNo ratings yet
- Paralympic No ClassificationDocument33 pagesParalympic No Classificationfirman pratamaNo ratings yet
- Patologi KardiopulmonalDocument43 pagesPatologi Kardiopulmonal9661jackNo ratings yet
- Drop Foot Therapy PracticesDocument3 pagesDrop Foot Therapy PracticesRiina HapsariiNo ratings yet
- Algoritma LeDocument1 pageAlgoritma LerimaNo ratings yet
- Analisis Gerakan Open and Close Kinetic ChainDocument5 pagesAnalisis Gerakan Open and Close Kinetic ChainAyoe FeratywiNo ratings yet
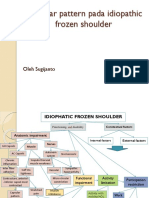
- Capsular pattern identification in idiopathic frozen shoulderDocument11 pagesCapsular pattern identification in idiopathic frozen shoulderRhany JulyatiNo ratings yet
- Ice TowelDocument4 pagesIce TowelAyu sulistiani dianingtyasNo ratings yet
- Wrist Joint Anatomy and TestsDocument38 pagesWrist Joint Anatomy and Testscamy bhagatNo ratings yet
- Tumbang ICF ADHDDocument1 pageTumbang ICF ADHDNovita OktavianaNo ratings yet
- Efektivitas Peningkatan Aktifitas Fungsional Dengan Intervensi Ice Massage Dan Terapi Latihan Pada Kasus Plantar FasciitisDocument8 pagesEfektivitas Peningkatan Aktifitas Fungsional Dengan Intervensi Ice Massage Dan Terapi Latihan Pada Kasus Plantar FasciitisTiara PutriNo ratings yet
- Jurnal William Flexion Exercise PDFDocument13 pagesJurnal William Flexion Exercise PDFRennyRay67% (3)
- Knee Injury and Osteoarthritis Outcome Score Koos PDFDocument4 pagesKnee Injury and Osteoarthritis Outcome Score Koos PDFNuruel Thamie PoethreeNo ratings yet
- Rom IsomDocument1 pageRom Isomnurma aha100% (1)
- Microwave Diathermy 2013Document27 pagesMicrowave Diathermy 2013Faisal QureshiNo ratings yet
- Pelvic Floor Impact Questionnaire (PFIQ-7)Document2 pagesPelvic Floor Impact Questionnaire (PFIQ-7)Dharitri PurohitNo ratings yet
- Mobilisasi ShoulderDocument55 pagesMobilisasi ShoulderMaria Dwi100% (2)
- Effect of Cailliet and Mc. Kenzie Neck Exercise in Reducing Pain in Miofacial Neck Syndrome AbstractDocument5 pagesEffect of Cailliet and Mc. Kenzie Neck Exercise in Reducing Pain in Miofacial Neck Syndrome AbstractVeronika AtaNo ratings yet
- Fisio Bedah ThoraxDocument7 pagesFisio Bedah ThoraxDian Nindita KusumaningtyasNo ratings yet
- Chondromalacia Patella: Causes, Tests, and Physical Therapy TreatmentsDocument10 pagesChondromalacia Patella: Causes, Tests, and Physical Therapy TreatmentsAfifah NurNo ratings yet
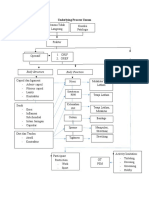
- Underlying Proccess (Clinical Reasoning) : OverusedDocument1 pageUnderlying Proccess (Clinical Reasoning) : OverusedAstrid Nasna LarasatiNo ratings yet
- TM Regio Shoulder Girdle 2014-2015Document83 pagesTM Regio Shoulder Girdle 2014-2015erlinaNo ratings yet
- 1 2 Evidence Based Practice PTDocument68 pages1 2 Evidence Based Practice PT9661jackNo ratings yet
- Development of The Early Activity Scale For EnduranceDocument1 pageDevelopment of The Early Activity Scale For EnduranceAsesino GuerreroNo ratings yet
- Fugl-Meyer Assessment Lower Extremity (Fma-Le) Assessment of Sensorimotor FunctionDocument2 pagesFugl-Meyer Assessment Lower Extremity (Fma-Le) Assessment of Sensorimotor FunctionDũng HoàngNo ratings yet
- Kuesioner LansiaDocument6 pagesKuesioner LansiaNadhratul NadhiraNo ratings yet
- Penatalaksanaan Fisioterapi Pada LymphedemaDocument19 pagesPenatalaksanaan Fisioterapi Pada Lymphedemamaevy dwiNo ratings yet
- Matsyasana (Fish Pose) : TechniqueDocument1 pageMatsyasana (Fish Pose) : TechniqueKarisma SenapatiNo ratings yet
- LBP MyogenikDocument12 pagesLBP MyogenikDewiSukma'sNo ratings yet
- Icf KardiorespirasiDocument8 pagesIcf KardiorespirasiTahu BulatNo ratings yet
- Jurnal Ilmiah Fisioterapi (JIF) Volume 03 Nomor 01 Februari 2020Document6 pagesJurnal Ilmiah Fisioterapi (JIF) Volume 03 Nomor 01 Februari 2020Putri teopani saragihNo ratings yet
- Chest Physio RCT Finds No Benefit in Pediatric PneumoniaDocument7 pagesChest Physio RCT Finds No Benefit in Pediatric Pneumoniaaufa memeyNo ratings yet
- S.S Scale: Skala Braden Versi Indonesia Skala Braden Faktor DeskripsiDocument5 pagesS.S Scale: Skala Braden Versi Indonesia Skala Braden Faktor DeskripsiDIAN EKASOSIAWATINo ratings yet
- Log Sheet Fisioterapi AgustusDocument3 pagesLog Sheet Fisioterapi Agustusdocerick87No ratings yet
- Calcaneus SpurDocument21 pagesCalcaneus SpurekoNo ratings yet
- Pediatric Balance Scale Sixteen Balance TestDocument8 pagesPediatric Balance Scale Sixteen Balance TestEddy Lanang'e JagadNo ratings yet
- UNDERLYING PROCESS MeniscusDocument1 pageUNDERLYING PROCESS MeniscusshafiyahNo ratings yet
- Romberg Test Examines Proprioception DeficitDocument7 pagesRomberg Test Examines Proprioception DeficitDwi P Ramadhani0% (1)
- Faradic CurrentDocument38 pagesFaradic CurrentCHANDAN RAINo ratings yet
- Kinesiology ElbowDocument53 pagesKinesiology Elbowsingle_ladyNo ratings yet
- Efektivitas Quadriceps Setting Exercise (QSE) Dalam Meningkatkan Kemampuan Fungsional Pada Pasien Osteoartritis Lutut Genu BilateralDocument8 pagesEfektivitas Quadriceps Setting Exercise (QSE) Dalam Meningkatkan Kemampuan Fungsional Pada Pasien Osteoartritis Lutut Genu BilateralSiti lestarinurhamidahNo ratings yet
- Contrast Bath - MKKDocument10 pagesContrast Bath - MKKKishore KumarNo ratings yet
- Modified Bass TestDocument7 pagesModified Bass Testchristopher100% (1)
- 02 Naskah PublikasiDocument15 pages02 Naskah PublikasiDesbyan candraNo ratings yet
- Shoulder Pain Index for Assessing DisabilityDocument2 pagesShoulder Pain Index for Assessing DisabilityLindaPramusintaNo ratings yet
- Laporan Assesment TMJDocument21 pagesLaporan Assesment TMJHusnannisa ArifNo ratings yet
- Genu Valgus Genu VarusDocument35 pagesGenu Valgus Genu VarusRatu FaniaNo ratings yet
- Fugel MayerDocument2 pagesFugel MayerRoman AlexandruNo ratings yet
- Shoulder Dislocation ARSDocument4 pagesShoulder Dislocation ARSBambang Ulan AeiyuNo ratings yet
- Ankle SprainDocument6 pagesAnkle Sprainshifali guptaNo ratings yet
- CASE REPORT PTB-SC - RajaDocument15 pagesCASE REPORT PTB-SC - RajaAristyoLeksonoNo ratings yet
- CASE REPORT TSB - RajaDocument12 pagesCASE REPORT TSB - RajaAristyoLeksonoNo ratings yet
- Physiotherapy management of paediatric flat feetDocument20 pagesPhysiotherapy management of paediatric flat feetCalvina Mizumi100% (1)
- Terapi Latihan: Kelompok 4: Nurul Dian Efendi Claudia Margarani Gungde Yudhanta BellawaDocument56 pagesTerapi Latihan: Kelompok 4: Nurul Dian Efendi Claudia Margarani Gungde Yudhanta BellawaGildarts KunNo ratings yet
- Kelompok 3: Stretching ExerciseDocument46 pagesKelompok 3: Stretching ExerciseGildarts KunNo ratings yet
- ResistanceDocument43 pagesResistanceGildarts KunNo ratings yet
- Exercise For Impaired BalanceDocument43 pagesExercise For Impaired BalanceGildarts KunNo ratings yet
- Range of MotionDocument34 pagesRange of MotionGildarts KunNo ratings yet
- Berg Balance ScaleDocument4 pagesBerg Balance ScaleSanjanaNo ratings yet
- Comparison of The Effects of Fartlek Exercise and Interval Training Towards The Improvement of Vo2 MaximumDocument6 pagesComparison of The Effects of Fartlek Exercise and Interval Training Towards The Improvement of Vo2 MaximumGildarts KunNo ratings yet
- Frozen Shoulder Short ReportDocument4 pagesFrozen Shoulder Short ReportGildarts KunNo ratings yet
- 15.2.1 - Postoperative Management of The Hip MonographDocument26 pages15.2.1 - Postoperative Management of The Hip MonographAngelaNo ratings yet
- Kelompok 3 Casing SindromeDocument9 pagesKelompok 3 Casing SindromeChristinaTriAstutiPauNo ratings yet
- Cat Dissection Guide NetDocument46 pagesCat Dissection Guide NetHazel Grace Bellen100% (3)
- Basic Anatomy & Physiology Study QuestionsDocument10 pagesBasic Anatomy & Physiology Study QuestionsHema JothyNo ratings yet
- Space Regainer 2Document12 pagesSpace Regainer 2rahmadhanidianNo ratings yet
- Hold the foot firmly in dorsiflexion to relax the gastrocnemiusmuscle and expose the Achilles tendon fullyDocument13 pagesHold the foot firmly in dorsiflexion to relax the gastrocnemiusmuscle and expose the Achilles tendon fullyNurul Huda M ShahrinNo ratings yet
- Biomedic (Myology)Document19 pagesBiomedic (Myology)Sadam_fasterNo ratings yet
- Development of Occlusion in Primary and Permanent DentitionDocument18 pagesDevelopment of Occlusion in Primary and Permanent DentitionAshis BiswasNo ratings yet
- SonoAce - R7 - Reference Manual - PDocument230 pagesSonoAce - R7 - Reference Manual - PEcomedical PlussNo ratings yet
- Deep Neck InfectionDocument46 pagesDeep Neck InfectionVicky SankaranNo ratings yet
- Therapeutic Exercise: The HipDocument39 pagesTherapeutic Exercise: The HipMuhammad UsmanNo ratings yet
- Common Gym Equipments: 1. Name: Treadmill DescriptionDocument12 pagesCommon Gym Equipments: 1. Name: Treadmill DescriptiongtNo ratings yet
- S.3 Biology - Home Assignment 2020Document3 pagesS.3 Biology - Home Assignment 2020mark lwangaNo ratings yet
- ANATOMY AND PHYSIOLOGY (Muscular System)Document2 pagesANATOMY AND PHYSIOLOGY (Muscular System)Gwyn Louise CarolinoNo ratings yet
- Cat Dissection GuideDocument46 pagesCat Dissection GuideShelomi GerdanNo ratings yet
- Airway Management For The Respiratory TherapistDocument30 pagesAirway Management For The Respiratory TherapistapolloNo ratings yet
- Shoulder WorkoutDocument2 pagesShoulder Workoutsteven stowelNo ratings yet
- Reflex: Ginus Partadiredja Department of PhysiologyDocument18 pagesReflex: Ginus Partadiredja Department of PhysiologyAdeLia Nur FitrianaNo ratings yet
- Total Body Training by Darko 31Document6 pagesTotal Body Training by Darko 31Matthew ThompsonNo ratings yet
- Postural HygieneDocument10 pagesPostural Hygienethemasterofanaldestruction33No ratings yet
- Una Comparación Biomecánica de Diferentes Métodos de Entrenamiento de Bateo de Béisbol.Document11 pagesUna Comparación Biomecánica de Diferentes Métodos de Entrenamiento de Bateo de Béisbol.jhonattan sandovalNo ratings yet
- Muscles of The BackDocument7 pagesMuscles of The BackDon RaulNo ratings yet
- Improve Your Cardiorespiratory and Muscular FitnessDocument16 pagesImprove Your Cardiorespiratory and Muscular FitnessArabella Grace AcibarNo ratings yet
- Module Two Wellness Plan 2 1 1 1Document15 pagesModule Two Wellness Plan 2 1 1 1LailaNo ratings yet
- Development of Rhombencephalon and MesencephalonDocument27 pagesDevelopment of Rhombencephalon and MesencephalonRafique AhmedNo ratings yet
- Thyroid Diseases Embryology, Anatomy, Investigations and TreatmentDocument41 pagesThyroid Diseases Embryology, Anatomy, Investigations and TreatmentUday Kumar KolluriNo ratings yet
- Hormonal Control of Metabolism During ExerciseDocument32 pagesHormonal Control of Metabolism During ExerciseamirNo ratings yet
- Defining anatomy and physiologyDocument3 pagesDefining anatomy and physiologyMARY ANGELA LERIOSNo ratings yet
- V. B.A.,D.D.S. : Complete DenturesDocument10 pagesV. B.A.,D.D.S. : Complete DenturesbarbieNo ratings yet