You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
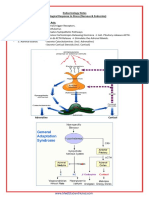
- A&P - 7. Physiological Response To Stress (5p)Document5 pagesA&P - 7. Physiological Response To Stress (5p)Sreejith Jagal KishoreNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- A&p - All Files in One PDFDocument52 pagesA&p - All Files in One PDFSreejith Jagal KishoreNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A&P - 4. Insulin, Glucagon & Regulation of Metabolism (6p) PDFDocument6 pagesA&P - 4. Insulin, Glucagon & Regulation of Metabolism (6p) PDFSreejith Jagal KishoreNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- A&P - 2. The Hypothalamo-Pituitary Axis (9p) PDFDocument9 pagesA&P - 2. The Hypothalamo-Pituitary Axis (9p) PDFSreejith Jagal KishoreNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Surgical CountingDocument41 pagesSurgical CountingSreejith Jagal KishoreNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- DR PDFDocument252 pagesDR PDFa_ouchar0% (1)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Comparing Exponential NumbersDocument5 pagesComparing Exponential NumbersMaya RahayuNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Irina Maleeva - Ariel Snowflake x6 - ENG - FreeDocument4 pagesIrina Maleeva - Ariel Snowflake x6 - ENG - FreeMarinaKorzinaNo ratings yet
- Innerwear Industry Pitch PresentationDocument19 pagesInnerwear Industry Pitch PresentationRupeshKumarNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- 4 Force & ExtensionDocument13 pages4 Force & ExtensionSelwah Hj AkipNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Passion For Cacti and Other Succulents: June 2017Document140 pagesThe Passion For Cacti and Other Succulents: June 2017golf2010No ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
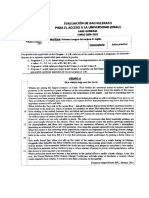
- Texto EBAU 1Document2 pagesTexto EBAU 1haridianrm13No ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Better - Homes.and - Gardens.usa - TruePDF December.2018Document136 pagesBetter - Homes.and - Gardens.usa - TruePDF December.2018MadaMadutsaNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Owner'S Manual: 2023 Chassis CabDocument444 pagesOwner'S Manual: 2023 Chassis CabDmitry DimasNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- 2015 Nos-Dcp National Oil Spill Disaster Contingency PlanDocument62 pages2015 Nos-Dcp National Oil Spill Disaster Contingency PlanVaishnavi Jayakumar100% (1)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Cost Analysis - Giberson Art GlassDocument3 pagesCost Analysis - Giberson Art GlassSessy Saly50% (2)
- Circle The Best Answer A, B, C, D or EDocument4 pagesCircle The Best Answer A, B, C, D or Ewilder jackNo ratings yet
- S TR GEN ID (Component Marking) (Rev 3 2009) - AN Marked UpDocument6 pagesS TR GEN ID (Component Marking) (Rev 3 2009) - AN Marked UpsnclgsraoNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Material Specification - 077154C-000-JSS-1700-009 - DDocument13 pagesMaterial Specification - 077154C-000-JSS-1700-009 - DStructures ProductionNo ratings yet
- Food Taste Panel Evaluation Form 2Document17 pagesFood Taste Panel Evaluation Form 2Akshat JainNo ratings yet
- Catalogo GatesDocument255 pagesCatalogo GatesBenjamin HedoneweNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Considerations For Impeller Trimming - Empowering Pumps and EquipmentDocument8 pagesConsiderations For Impeller Trimming - Empowering Pumps and Equipment김기준No ratings yet
- Drilling & GroutingDocument18 pagesDrilling & GroutingSantosh Laxman PatilNo ratings yet
- EXP4 The Diels Alder ReactionsDocument3 pagesEXP4 The Diels Alder ReactionsLaura GuidoNo ratings yet
- 300 PSI CTS (MP-1115) Operation Manual Rev1.3Document18 pages300 PSI CTS (MP-1115) Operation Manual Rev1.3Juan Manuel VizosoNo ratings yet
- 12/1/2014 Powder MetallurgyDocument29 pages12/1/2014 Powder Metallurgysofyan sam0% (2)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Cross Talk Details and RoutingDocument29 pagesCross Talk Details and RoutingRohith RajNo ratings yet
- 3 Tasks and ANS - Gamma Maths PDFDocument6 pages3 Tasks and ANS - Gamma Maths PDFNora ZhangNo ratings yet
- Indor Lighting DesignDocument33 pagesIndor Lighting DesignRajesh MalikNo ratings yet
- OurCatholicFaith PowerPoint Chapter1Document21 pagesOurCatholicFaith PowerPoint Chapter1VinNo ratings yet
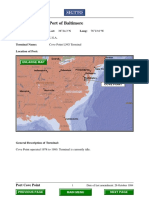
- Port Name: Port of BaltimoreDocument17 pagesPort Name: Port of Baltimoremohd1khairul1anuarNo ratings yet
- CBSE DetailsDocument6 pagesCBSE DetailsNARESH KUMARNo ratings yet
- Poly 103Document20 pagesPoly 103Sharifah Zulaikha BenYahyaNo ratings yet
- 08 Activity 1 (10) (LM)Document2 pages08 Activity 1 (10) (LM)Jhanine Mae Oriola FortintoNo ratings yet
- Cargo ManagementDocument45 pagesCargo ManagementShubham Chaurasia75% (8)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)