You might also like
- ACS AMI FacilitatorDocument21 pagesACS AMI FacilitatorPaul Zantua57% (7)
- Sensing FeelingDocument3 pagesSensing FeelingElena UngureanuNo ratings yet
- Biolis 24i PDFDocument43 pagesBiolis 24i PDFMohamed Ben MohamedNo ratings yet
- PIIS1201971218345090Document9 pagesPIIS1201971218345090favorendaNo ratings yet
- Arc 3Document2 pagesArc 3AnilKumarNo ratings yet
- VIP Fang and Shi 2019 Arch Pathol 2019Document11 pagesVIP Fang and Shi 2019 Arch Pathol 2019Jemma ArakelyanNo ratings yet
- Https:neuronaldo - Com.br:wp Content:uploads:2012:04:7 Actinomyces Paper JVDI Final 7 2015Document6 pagesHttps:neuronaldo - Com.br:wp Content:uploads:2012:04:7 Actinomyces Paper JVDI Final 7 2015Lucas XavierNo ratings yet
- Cytology of Bone Fine Needle Aspiration BiopsyDocument11 pagesCytology of Bone Fine Needle Aspiration BiopsyRavi MehrotraNo ratings yet
- Epilepsy and Developmental Disorders - Next Generation Sequencing in The ClinicDocument9 pagesEpilepsy and Developmental Disorders - Next Generation Sequencing in The ClinicLocklinaNo ratings yet
- Jurnal DiagnostikDocument5 pagesJurnal DiagnostikRadityaRachman LandapaNo ratings yet
- Jama 2019 9394Document1 pageJama 2019 9394OcZzNo ratings yet
- A Systematic Review of Procyanidins Updates On Current Bioactivities and Potential Benefits in Wound HealingDocument6 pagesA Systematic Review of Procyanidins Updates On Current Bioactivities and Potential Benefits in Wound HealingMikail Ahmad FawzyNo ratings yet
- Evaluation of A Manual Identification System For Detection of Mycobacterium Tuberculosis in A Primary Tuberculosis Laboratory in ChinaDocument10 pagesEvaluation of A Manual Identification System For Detection of Mycobacterium Tuberculosis in A Primary Tuberculosis Laboratory in ChinaTonny YuliantoNo ratings yet
- Fchem 10 908386Document16 pagesFchem 10 908386Alan TaleviNo ratings yet
- Cancer VejigaDocument10 pagesCancer VejigaMELANY MIRELLA FLORES RODRIGUEZNo ratings yet
- Optic Nerve Glioma: Case Series With Review of Clinical, Radiologic, Molecular, and Histopathologic CharacteristicsDocument5 pagesOptic Nerve Glioma: Case Series With Review of Clinical, Radiologic, Molecular, and Histopathologic CharacteristicsUtama Hadiputra SurbaktiNo ratings yet
- Canine PlasmaDocument15 pagesCanine PlasmaEmoke PallNo ratings yet
- Edexcel Biology GuideDocument4 pagesEdexcel Biology GuideMageswary Sivalingam67% (3)
- AutismDocument2 pagesAutismGlenn GraystonNo ratings yet
- Sarcopenia ESPEN 2022Document9 pagesSarcopenia ESPEN 2022Tarafainy BasalamahNo ratings yet
- Abdi Et Al 2023 Operative Treatment of Tarlov Cysts Outcomes and Predictors of Improvement After Surgery A Series of 97Document8 pagesAbdi Et Al 2023 Operative Treatment of Tarlov Cysts Outcomes and Predictors of Improvement After Surgery A Series of 97jabarin.hNo ratings yet
- International Journal of International Journal of International Journal ofDocument6 pagesInternational Journal of International Journal of International Journal ofDeepak KumarNo ratings yet
- Estiadah - 113219001 - Tugas Kritisi JurnalDocument5 pagesEstiadah - 113219001 - Tugas Kritisi Jurnalestiadah tri nurmastutiNo ratings yet
- Penelitian AbstraktifDocument9 pagesPenelitian AbstraktifYondi Piter PapulungNo ratings yet
- Endoscopic Mucosal Tissue Sampling ASGE 2013Document9 pagesEndoscopic Mucosal Tissue Sampling ASGE 2013DannyNo ratings yet
- 10 1016@j Cca 2019 12 022Document6 pages10 1016@j Cca 2019 12 022Keyla Stephanie TorradoNo ratings yet
- Exosome Role in Sci RecoveryDocument13 pagesExosome Role in Sci RecoverySilverStarNo ratings yet
- Ma 71 84 PDFDocument5 pagesMa 71 84 PDFMirza ČelebičićNo ratings yet
- Genexpert For Diagnosis of Tubercular Meningitis: Clinical BriefDocument3 pagesGenexpert For Diagnosis of Tubercular Meningitis: Clinical BriefYas MiineNo ratings yet
- Activity 1 - HistopathologyDocument13 pagesActivity 1 - HistopathologyKang DanielNo ratings yet
- NIH Public AccessDocument14 pagesNIH Public AccessJamesNo ratings yet
- Organotypic Cultures of Adult Mouse Retina: Morphologic Changes and Gene ExpressionDocument11 pagesOrganotypic Cultures of Adult Mouse Retina: Morphologic Changes and Gene ExpressionErick MartinezNo ratings yet
- Clinicopathological Correlation in Diagnosis of Hansen's Disease: A Histopathologist's PerspectiveDocument12 pagesClinicopathological Correlation in Diagnosis of Hansen's Disease: A Histopathologist's PerspectiveRani Dwi HapsariNo ratings yet
- Ricafort - Finals Journal Critiquing IS LectureDocument2 pagesRicafort - Finals Journal Critiquing IS Lecturesean ricafortNo ratings yet
- A Systematic Review of The Microbiome in Children With Neurodevelopmental DisordersDocument18 pagesA Systematic Review of The Microbiome in Children With Neurodevelopmental DisordersRaul Morales VillegasNo ratings yet
- Lepra y Neuropatia #5Document6 pagesLepra y Neuropatia #5Arcel De Luca G.No ratings yet
- Development of iPSC-based Clinical Trial Selection Platform For Patients With Ultrarare DiseasesDocument17 pagesDevelopment of iPSC-based Clinical Trial Selection Platform For Patients With Ultrarare DiseasesValen EstevezNo ratings yet
- 433 FullDocument6 pages433 FullBhargav YagnikNo ratings yet
- Apoptosis in Natural Rabies Virus Infection in DogsDocument5 pagesApoptosis in Natural Rabies Virus Infection in DogspapiipiiNo ratings yet
- Intestinal Barrier Breakdown and Mucosal Microbiota Disturbance in Neuromyelitis Optical Spectrum DisordersDocument15 pagesIntestinal Barrier Breakdown and Mucosal Microbiota Disturbance in Neuromyelitis Optical Spectrum DisordersmagarciacastilloNo ratings yet
- Urine Dipstick of Sputum For The Rapid Diagnosis of Community Acquired PneumoniaDocument4 pagesUrine Dipstick of Sputum For The Rapid Diagnosis of Community Acquired PneumoniaStephen JohanNo ratings yet
- 1 s2.0 S0378111916305455 MainDocument4 pages1 s2.0 S0378111916305455 Mainguadalupe.formiaNo ratings yet
- Pi Is 0022534715046030Document8 pagesPi Is 0022534715046030rodesa barnawi17211994No ratings yet
- Ajith TheDocument26 pagesAjith ThekalyanpavuralaNo ratings yet
- Chairside Diagnosis of Periodontal Diseases A ReviewDocument4 pagesChairside Diagnosis of Periodontal Diseases A ReviewEditor IJTSRDNo ratings yet
- International Journal of Infectious DiseasesDocument7 pagesInternational Journal of Infectious DiseasesWINY LESLI ALFONSO BAUTISTANo ratings yet
- Genome Pathways For Cell-09-643644Document12 pagesGenome Pathways For Cell-09-643644AlmedinaNo ratings yet
- A Diagnostic Study Comparing Conventional and Real-Time PCR For Strongyloides Stercoralis On Urine and On Faecal SamplesDocument4 pagesA Diagnostic Study Comparing Conventional and Real-Time PCR For Strongyloides Stercoralis On Urine and On Faecal SamplesSamuel VergaraNo ratings yet
- Aneuploidy ConcordanceDocument12 pagesAneuploidy ConcordancejuanNo ratings yet
- Triagem Pré Anestésica de Cães IdososDocument5 pagesTriagem Pré Anestésica de Cães IdososRafaela RodriguesNo ratings yet
- Study 1Document7 pagesStudy 1Suyash BagdeNo ratings yet
- Evaluationofsmearmicroscopyandgene XpertfortbDocument6 pagesEvaluationofsmearmicroscopyandgene XpertfortbYohci FitrianiNo ratings yet
- Antinuclear Antibodies by Indirect Immunofluorescence: Optimum Screening Dilution For Diagnosis of Systemic Lupus ErythematosusDocument5 pagesAntinuclear Antibodies by Indirect Immunofluorescence: Optimum Screening Dilution For Diagnosis of Systemic Lupus ErythematosusMargriet MayasinNo ratings yet
- Journal of Pediatric Surgery: Justin P. Wagner, Veronica F. Sullins, James C.Y. DunnDocument6 pagesJournal of Pediatric Surgery: Justin P. Wagner, Veronica F. Sullins, James C.Y. DunnNiningFirganMr-GenNo ratings yet
- Gold-Nanobeacons For Gene Therapy: Evaluation of Genotoxicity, Cell Toxicity and Proteome Profiling AnalysisDocument63 pagesGold-Nanobeacons For Gene Therapy: Evaluation of Genotoxicity, Cell Toxicity and Proteome Profiling AnalysisGargi MishraNo ratings yet
- 2.2 Validation of Autopsy and Specimen Collection Techniques and RNA Quality Assessment 2.2.1 BackgroundDocument12 pages2.2 Validation of Autopsy and Specimen Collection Techniques and RNA Quality Assessment 2.2.1 BackgroundjoliboomNo ratings yet
- Central Nervous System Diseases of Cattle in Georgia, 2001-2017Document6 pagesCentral Nervous System Diseases of Cattle in Georgia, 2001-2017Ni Putu YudiantariNo ratings yet
- 1 s2.0 S1063458421009602 MainDocument12 pages1 s2.0 S1063458421009602 Mainabo_youssof20047438No ratings yet
- Evaluation of Real Time PCR Aspergillus Spp. in Bronchoalveolar Lavage SamplesDocument4 pagesEvaluation of Real Time PCR Aspergillus Spp. in Bronchoalveolar Lavage Sampleskern tranhNo ratings yet
- Clin Infect Dis.-2013-Baron-cid-cit278Document100 pagesClin Infect Dis.-2013-Baron-cid-cit278RoNo ratings yet
- 54 482 1 PBDocument5 pages54 482 1 PBsansastarkNo ratings yet
- An Uncommon Poorly Differentiated Small Cell Neuro-Endocrine Carcinoma of Urinary Bladder A Review With Case ReportDocument3 pagesAn Uncommon Poorly Differentiated Small Cell Neuro-Endocrine Carcinoma of Urinary Bladder A Review With Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Microsart @media: Advanced System For Touch-Free Membrane TransferDocument4 pagesMicrosart @media: Advanced System For Touch-Free Membrane TransferVijay Kumar NandagiriNo ratings yet
- Head Space Gas Chromatography Analysis of Residual Solvents in Temozolomide by Using Zb-624 ColumnDocument9 pagesHead Space Gas Chromatography Analysis of Residual Solvents in Temozolomide by Using Zb-624 ColumnchiralicNo ratings yet
- Drugs 1Document14 pagesDrugs 1Theesha SophieNo ratings yet
- A Review On Recent Developments in The Determination of Residual Solvents by Gas ChromatographyDocument9 pagesA Review On Recent Developments in The Determination of Residual Solvents by Gas ChromatographychiralicNo ratings yet
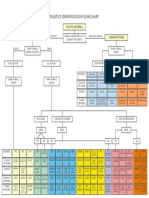
- Plastics Identification Flow ChartDocument1 pagePlastics Identification Flow ChartchiralicNo ratings yet
- Data Microsart Ejet SM 2008 A DataDocument2 pagesData Microsart Ejet SM 2008 A DatachiralicNo ratings yet
- ISO Standards and Bias Pierce DrorDocument10 pagesISO Standards and Bias Pierce DrorchiralicNo ratings yet
- Microsart Manifolds: The Filtration Stand That Adapts To Your NeedDocument8 pagesMicrosart Manifolds: The Filtration Stand That Adapts To Your NeedchiralicNo ratings yet
- Application: Organic Volatile Impurities in Pharmaceutical Products: Selectivity of Capillary GC ColumnsDocument2 pagesApplication: Organic Volatile Impurities in Pharmaceutical Products: Selectivity of Capillary GC ColumnschiralicNo ratings yet
- The World Clock - WorldwideDocument1 pageThe World Clock - WorldwidechiralicNo ratings yet
- Fungi: Candida Auris: A Review of Recommendations For Detection and Control in Healthcare SettingsDocument11 pagesFungi: Candida Auris: A Review of Recommendations For Detection and Control in Healthcare SettingschiralicNo ratings yet
- Attune NXT Flow Cytometer: Efficient. Flexible. TransformativeDocument36 pagesAttune NXT Flow Cytometer: Efficient. Flexible. TransformativechiralicNo ratings yet
- Simultaneous Estimation of Residual Solvents (Ethanol, Acetone, Dichloromethane and Ethyl Acetate) in Dosage Form by GC-HS-FIDDocument7 pagesSimultaneous Estimation of Residual Solvents (Ethanol, Acetone, Dichloromethane and Ethyl Acetate) in Dosage Form by GC-HS-FIDchiralicNo ratings yet
- Candida Auris: A Brief ReviewDocument7 pagesCandida Auris: A Brief ReviewchiralicNo ratings yet
- On-Site Fuel and Lubricant Quality Control by Portable FTIR AnalysersDocument2 pagesOn-Site Fuel and Lubricant Quality Control by Portable FTIR AnalyserschiralicNo ratings yet
- KAM LKF and PKF: Karl Fischer Moisture AnalyzerDocument22 pagesKAM LKF and PKF: Karl Fischer Moisture AnalyzerchiralicNo ratings yet
- Electrodes For Titration: Which Electrode For Which Application?Document2 pagesElectrodes For Titration: Which Electrode For Which Application?chiralicNo ratings yet
- Application Note - HiQ Hydrogen As An Alternative To Helium For GC - tcm899-90120Document16 pagesApplication Note - HiQ Hydrogen As An Alternative To Helium For GC - tcm899-90120chiralicNo ratings yet
- CO Incubator: Resource GuideDocument8 pagesCO Incubator: Resource GuidechiralicNo ratings yet
- Baths - Chillers - Resource GuideDocument8 pagesBaths - Chillers - Resource GuidechiralicNo ratings yet
- Grain and Processed Grain Solutions: The Complete Product RangeDocument8 pagesGrain and Processed Grain Solutions: The Complete Product RangechiralicNo ratings yet
- Quality Control Solutions For The Feed IndustryDocument4 pagesQuality Control Solutions For The Feed IndustrychiralicNo ratings yet
- And The Correct Answers Are:: You Got All Good Values: !!! You Are AnDocument3 pagesAnd The Correct Answers Are:: You Got All Good Values: !!! You Are AnchiralicNo ratings yet
- 425-06 - Duo Sas 360 - UkDocument1 page425-06 - Duo Sas 360 - UkchiralicNo ratings yet
- On-Site Fuel and Lubricant Quality Control by Portable FTIR AnalysersDocument2 pagesOn-Site Fuel and Lubricant Quality Control by Portable FTIR AnalyserschiralicNo ratings yet
- Application Compare Sipper Cuvettes Cary-3500 Uv-Vis 5994-1951en Us AgilentDocument6 pagesApplication Compare Sipper Cuvettes Cary-3500 Uv-Vis 5994-1951en Us AgilentchiralicNo ratings yet
- Electrodes For Titration: Which Electrode For Which Application?Document2 pagesElectrodes For Titration: Which Electrode For Which Application?chiralicNo ratings yet
- AN362Document2 pagesAN362chiralicNo ratings yet
- HPLC003 Adamas 10-2018-LRDocument20 pagesHPLC003 Adamas 10-2018-LRchiralicNo ratings yet
- Bax System q7 Mpb-2001Document8 pagesBax System q7 Mpb-2001Tlw QuirogaNo ratings yet
- Allosteric Regulation & Covalent ModificationDocument10 pagesAllosteric Regulation & Covalent ModificationBhaskar Ganguly100% (1)
- Midterm and Final Exam TFNDocument6 pagesMidterm and Final Exam TFNalchriwNo ratings yet
- MSDS TSHDocument8 pagesMSDS TSHdwiNo ratings yet
- Public Policy Connect AnswersDocument11 pagesPublic Policy Connect AnswersMargarita ArnoldNo ratings yet
- Algerian Carob Tree Products PDFDocument10 pagesAlgerian Carob Tree Products PDFStîngă DanielaNo ratings yet
- IDSA Guias Infeccion de Tejidos Blandos 2014 PDFDocument43 pagesIDSA Guias Infeccion de Tejidos Blandos 2014 PDFyonaNo ratings yet
- Bio 2Document3 pagesBio 2ganchimeg gankhuuNo ratings yet
- Manufacturing ProcessesDocument6 pagesManufacturing ProcessesSudalai MadanNo ratings yet
- Hitec 8888Z Atf C4 & To4 - TDSDocument2 pagesHitec 8888Z Atf C4 & To4 - TDSPranit More Arabian Petroleum LimitedNo ratings yet
- Business ModelDocument3 pagesBusiness ModelEric AryeepahNo ratings yet
- 1000 Câu Word FormDocument36 pages1000 Câu Word FormThùy Linh LêNo ratings yet
- Aliyani Association Between Vitamin D Deficiency and Psoriasis A CasecontrolstudyDocument5 pagesAliyani Association Between Vitamin D Deficiency and Psoriasis A CasecontrolstudyAzmi FadhlihNo ratings yet
- Aaron Magana's Resume, Business AnalystDocument3 pagesAaron Magana's Resume, Business AnalystEmiNo ratings yet
- SAVULESCU, Julian - A Simple Solution To The Puzzles of End of LifeDocument5 pagesSAVULESCU, Julian - A Simple Solution To The Puzzles of End of Lifediradosta_1992No ratings yet
- Animal Death Unknown 2010Document57 pagesAnimal Death Unknown 2010Vincent J. CataldiNo ratings yet
- Invoice, packing list mẫuDocument2 pagesInvoice, packing list mẫuPHI BUI MINHNo ratings yet
- Siklus Biogeokimia - Retensi NutrienDocument24 pagesSiklus Biogeokimia - Retensi NutrienPutri Nur Fadhilah YasharNo ratings yet
- Method For Emission Spectrometric Analysis of Plain Carbon and Low Alloy Steels Point To Plane Technique (Document8 pagesMethod For Emission Spectrometric Analysis of Plain Carbon and Low Alloy Steels Point To Plane Technique (DiptiNo ratings yet
- Bylaws-Craigs Mill Hoa 2013Document10 pagesBylaws-Craigs Mill Hoa 2013api-243024250No ratings yet
- Khalifa NagwaDocument111 pagesKhalifa NagwajokonudiNo ratings yet
- Climate Responsive ArchitectureDocument32 pagesClimate Responsive ArchitectureNikhila CherughattuNo ratings yet
- Lymph Node Levels of The NeckDocument2 pagesLymph Node Levels of The NeckRem AlfelorNo ratings yet
- Bộ Đề Ôn Tập HK1 (Kèm Lời Giải Chi Tiết)Document51 pagesBộ Đề Ôn Tập HK1 (Kèm Lời Giải Chi Tiết)Lê Thị Ngọc AnhNo ratings yet
- DS 1 CatDocument38 pagesDS 1 CatMuhammad Bilal Khattak100% (1)
- Mayank Yadav: Academic QualificationDocument2 pagesMayank Yadav: Academic QualificationJacob PruittNo ratings yet
- My Project PresentationDocument12 pagesMy Project Presentationkarunasand15No ratings yet
- Problems SetDocument10 pagesProblems SetSajith KurianNo ratings yet