You might also like
- Background Parkinson Disease Is Recognized As One of The Most Common Neurologic Disorders, AffectingDocument27 pagesBackground Parkinson Disease Is Recognized As One of The Most Common Neurologic Disorders, AffectingCharan Pal SinghNo ratings yet
- BAB I PaperDocument22 pagesBAB I Paperindry fitriNo ratings yet
- Seminar On Gait Rehab in PDDocument41 pagesSeminar On Gait Rehab in PDPriya KuberanNo ratings yet
- Parkinson's DiseaseDocument9 pagesParkinson's Diseaselucia desantisNo ratings yet
- Effect of Walking Along Circle On Foot Prints in Parkinson's On FreezingDocument48 pagesEffect of Walking Along Circle On Foot Prints in Parkinson's On FreezingAnup ShankarwarNo ratings yet
- What Is ParkinsonDocument23 pagesWhat Is Parkinsonlakshmi chowdamNo ratings yet
- ParkinsonDocument3 pagesParkinsonRJean TumalaNo ratings yet
- 186-Book Chapter-902-2-10-20210323Document24 pages186-Book Chapter-902-2-10-20210323Yelaena AbrauNo ratings yet
- Parkinson Disease - Radiology Reference ArticleDocument8 pagesParkinson Disease - Radiology Reference Articlenurul auliaNo ratings yet
- ParkinsonsDocument2 pagesParkinsonsidno1008No ratings yet
- Parkinson's DiseaseDocument9 pagesParkinson's DiseaseJahanvi MishraNo ratings yet
- 2019 European Academy of Neurology Parkinson DiseaseDocument16 pages2019 European Academy of Neurology Parkinson DiseaseJuan Diego Gutierrez ZevallosNo ratings yet
- History of Parkinson's Disease. in Western Medical Literature It Was Described by The Physician Galen As Shaking Palsy' in 175ADDocument12 pagesHistory of Parkinson's Disease. in Western Medical Literature It Was Described by The Physician Galen As Shaking Palsy' in 175ADMehar KhanNo ratings yet
- Journal - Collection of Journal NEUROCHEMISTRY 2006Document10 pagesJournal - Collection of Journal NEUROCHEMISTRY 2006leozdmNo ratings yet
- Gaceta 2fsfsdfDocument8 pagesGaceta 2fsfsdfIsrael Silva MartínezNo ratings yet
- Parkinsonism A General Motor Disability PDFDocument9 pagesParkinsonism A General Motor Disability PDFRishabh SinghNo ratings yet
- Parkinsons Disease - An OverviewDocument9 pagesParkinsons Disease - An Overviewapi-260359232No ratings yet
- Beitz 2014Document10 pagesBeitz 2014Anna Beatriz Silva EspindolaNo ratings yet
- Parkinson's DiseaseDocument32 pagesParkinson's DiseaseKristina Marie HernandezNo ratings yet
- PARKINSONISMDocument5 pagesPARKINSONISMPrashanth RajuNo ratings yet
- GeneticsDocument10 pagesGeneticsapi-3835615No ratings yet
- Parkinson Disease and AnesthesiaDocument13 pagesParkinson Disease and AnesthesiaTemoc TemocNo ratings yet
- Bjorn Tysnes 2017 Epidemiology of Parkinson's DiseaseDocument5 pagesBjorn Tysnes 2017 Epidemiology of Parkinson's DiseaseAmirafitrianandaNo ratings yet
- Queens' College 2011-2012 Biology Project-Parkinson'S DiseaseDocument16 pagesQueens' College 2011-2012 Biology Project-Parkinson'S DiseaseAshutosh GuptaNo ratings yet
- Parkinson's Disease: EpidemiologyDocument6 pagesParkinson's Disease: EpidemiologyCarlos MichasNo ratings yet
- Pilate Week 12 ParkinsonsDocument86 pagesPilate Week 12 ParkinsonsFiona Balfour PilateNo ratings yet
- Referensi NeuroDocument3 pagesReferensi NeuroAchmad FauzyNo ratings yet
- Parkinsons Thesis StatementDocument8 pagesParkinsons Thesis StatementMartha Brown100% (1)
- Parkinson S DiseaseDocument91 pagesParkinson S DiseaseTrisha Tolentino100% (1)
- Farrer 2006Document13 pagesFarrer 2006Somanshu BanerjeeNo ratings yet
- Biology of Parkinson S Disease Pathogenesis and Pathophysiology of A Multisystem Neurodegenerative DisorderDocument23 pagesBiology of Parkinson S Disease Pathogenesis and Pathophysiology of A Multisystem Neurodegenerative DisorderNelly LeónNo ratings yet
- Parkinson's Disease A Review 2014 PDFDocument19 pagesParkinson's Disease A Review 2014 PDFjeanNo ratings yet
- 1295188732neuro Essay 7 - How Have Studies of Neuropharmacology Helped Our Understanding of Movement Disorders EssayDocument4 pages1295188732neuro Essay 7 - How Have Studies of Neuropharmacology Helped Our Understanding of Movement Disorders EssayscholifyNo ratings yet
- Schizophrenia: Overview and Treatment OptionsDocument18 pagesSchizophrenia: Overview and Treatment OptionsMeindayaniNo ratings yet
- ParkinsonDocument6 pagesParkinsonSohret PektuncNo ratings yet
- AANA Journal Course: Update For Nurse Anesthetists Parkinson DiseaseDocument6 pagesAANA Journal Course: Update For Nurse Anesthetists Parkinson DiseaseMarianne GarciaNo ratings yet
- Parkinson Disease Epidemiology, Pathology, Genetics, and PathophysiologyDocument12 pagesParkinson Disease Epidemiology, Pathology, Genetics, and PathophysiologyAna María Arenas DávilaNo ratings yet
- Epigenetic Inactivation of The Autophagy - Lysosomal System in Appendix in Parkinson 'S DiseaseDocument18 pagesEpigenetic Inactivation of The Autophagy - Lysosomal System in Appendix in Parkinson 'S DiseaseOliwia MalonNo ratings yet
- Physiology - Research PaperDocument9 pagesPhysiology - Research PaperKaylee BlankenshipNo ratings yet
- Prof BSP-Akinetic Rigid Synd - PDDocument139 pagesProf BSP-Akinetic Rigid Synd - PDSavitha BasriNo ratings yet
- Sleep Disorders in Parkinson’s Disease: Management and Case StudyFrom EverandSleep Disorders in Parkinson’s Disease: Management and Case StudyChun-Feng LiuNo ratings yet
- Phytotherapy in Treatment of Parkinson's Disease: A Review: Pharmaceutical BiologyDocument9 pagesPhytotherapy in Treatment of Parkinson's Disease: A Review: Pharmaceutical BiologyG. Araya MoraNo ratings yet
- ParkinsonDocument2 pagesParkinsonpatel Mehul100% (1)
- Epidemiology of PDDocument11 pagesEpidemiology of PDElaAcevesNo ratings yet
- Drug-Induced Parkinsonism: Hae-Won Shin, Sun Ju ChungDocument7 pagesDrug-Induced Parkinsonism: Hae-Won Shin, Sun Ju ChungBaskarazrNo ratings yet
- Parkinson ThesisDocument4 pagesParkinson Thesisandreajimenezomaha100% (1)
- Stem Cell-Based Therapies For Parkinson DiseaseDocument17 pagesStem Cell-Based Therapies For Parkinson DiseaseYunita Christiani BiyangNo ratings yet
- What Is Parkinson's Disease?Document3 pagesWhat Is Parkinson's Disease?pingkan septianiNo ratings yet
- TG 4 Parkinson (NL)Document20 pagesTG 4 Parkinson (NL)Novi AdriNo ratings yet
- Pisa Syndrome Source Clin Neuropharmacol SO 2015 Jul Aug 38 4 135 40 (PMIDT26166239)Document6 pagesPisa Syndrome Source Clin Neuropharmacol SO 2015 Jul Aug 38 4 135 40 (PMIDT26166239)dai shujuanNo ratings yet
- Research Paper Parkinson DiseaseDocument5 pagesResearch Paper Parkinson Diseasem0d1p1fuwub2100% (1)
- Https Emedicine - Medscape.com Article 1831191-PrintDocument59 pagesHttps Emedicine - Medscape.com Article 1831191-PrintNoviatiPrayangsariNo ratings yet
- Vitro Neurotransmitter Receptor Binding: Assessment of Psychoactive Potential of Flemingia Macrophylla Following in AssayDocument15 pagesVitro Neurotransmitter Receptor Binding: Assessment of Psychoactive Potential of Flemingia Macrophylla Following in Assaylalit2008_2008No ratings yet
- American Academy of Neurology Key PointsDocument193 pagesAmerican Academy of Neurology Key Pointszayat13No ratings yet
- Molecular Neurology: Parkinson's DiseaseDocument32 pagesMolecular Neurology: Parkinson's DiseaseSoumya Sunny100% (1)
- Bab I Pendahuluan: "Essay On The Shaking Palsy"Document40 pagesBab I Pendahuluan: "Essay On The Shaking Palsy"hidayatul rahmoNo ratings yet
- ptj4008504 PDFDocument8 pagesptj4008504 PDFDiva VashtiNo ratings yet
- What Is Parkinson's Disease?Document26 pagesWhat Is Parkinson's Disease?Sunil Kumar SinghNo ratings yet
- Animal Model of EADocument13 pagesAnimal Model of EAzigurat00No ratings yet
- The Genes of Parkinson's DiseaseDocument6 pagesThe Genes of Parkinson's Diseaseapi-26116142No ratings yet
- CGMP 210 PDFDocument3 pagesCGMP 210 PDFshamma shahulhameedNo ratings yet
- Design and Evaluation of Buccal Patches Containing Combination of Hydrochlorothiazide and AtenololDocument8 pagesDesign and Evaluation of Buccal Patches Containing Combination of Hydrochlorothiazide and Atenololshamma shahulhameedNo ratings yet
- Buccal Drug Delivery SystemDocument35 pagesBuccal Drug Delivery Systemshamma shahulhameedNo ratings yet
- Single Layer Drug in Adhesives. Multi-Layer Drug in Adhesives. Micro Reservoir Controlled TddsDocument47 pagesSingle Layer Drug in Adhesives. Multi-Layer Drug in Adhesives. Micro Reservoir Controlled Tddsshamma shahulhameedNo ratings yet
- 2020 Liver DiseasesDocument43 pages2020 Liver Diseasesshamma shahulhameedNo ratings yet
- Upper Respiratory Tract InfectionsDocument20 pagesUpper Respiratory Tract Infectionsshamma shahulhameedNo ratings yet
- Diabetes Mellitus 1Document19 pagesDiabetes Mellitus 1shamma shahulhameedNo ratings yet
- Epilepsy: Incidence and PrevalenceDocument25 pagesEpilepsy: Incidence and Prevalenceshamma shahulhameedNo ratings yet
- Generic Drug ApprovalDocument17 pagesGeneric Drug Approvalshamma shahulhameedNo ratings yet
- HEPATITSDocument21 pagesHEPATITSshamma shahulhameedNo ratings yet
- Impaired Neurotransmission in Early-Treated Phenylketonuria PatientsDocument9 pagesImpaired Neurotransmission in Early-Treated Phenylketonuria PatientsAndreea StefanNo ratings yet
- Structure and Neural Mechanisms of CatatoniaDocument10 pagesStructure and Neural Mechanisms of CatatoniaAlejandra ToralNo ratings yet
- References BeevisDocument70 pagesReferences BeevisEdarl Jupia NazarioNo ratings yet
- Angol Nyelv Emelt Szint: Azonosító JelDocument2 pagesAngol Nyelv Emelt Szint: Azonosító JelAnita BódiNo ratings yet
- Chapt 39Document7 pagesChapt 39Hakesh PratikNo ratings yet
- How Emotionally Intelligent People Handle Toxic PeopleDocument5 pagesHow Emotionally Intelligent People Handle Toxic PeopleMarkoNo ratings yet
- Research:Senior-Principal Scientist or Director or Group LeaderDocument9 pagesResearch:Senior-Principal Scientist or Director or Group Leaderapi-121636983No ratings yet
- Brain Mnemonic SDocument36 pagesBrain Mnemonic SLouie OkayNo ratings yet
- 1940 Doreal Spiritual Power Magnetic HealingDocument29 pages1940 Doreal Spiritual Power Magnetic HealingNight BirdNo ratings yet
- 100 Weird Facts About The Human BodyDocument11 pages100 Weird Facts About The Human Bodycryonics20039984No ratings yet
- BSC Psychology 2017Document65 pagesBSC Psychology 2017THOMAS NJNo ratings yet
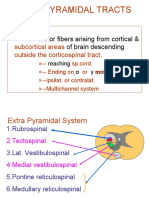
- Extrapyramidal Tracts: Motor Fibers Arising From Cortical & of Brain DescendingDocument21 pagesExtrapyramidal Tracts: Motor Fibers Arising From Cortical & of Brain DescendingAsfoor gake1No ratings yet
- Soal MCQ Blok 16Document14 pagesSoal MCQ Blok 16Mira Pandora100% (1)
- (Adolphs) Recognizing Emotion From Facial Exprressions - Psychological and Neurological MechanismsDocument43 pages(Adolphs) Recognizing Emotion From Facial Exprressions - Psychological and Neurological MechanismsPriss SaezNo ratings yet
- PsychopathologyDocument27 pagesPsychopathologyDessy EkaNo ratings yet
- TheWisestCalendar 2024 by PavanBhattadDocument22 pagesTheWisestCalendar 2024 by PavanBhattadSachin SharmaNo ratings yet
- Coordinated Functions of Nervous SystemDocument22 pagesCoordinated Functions of Nervous SystemMindi May AguilarNo ratings yet
- The Science of Psychology An Appreciative View 2020 5Th Edition Laura A King Full ChapterDocument67 pagesThe Science of Psychology An Appreciative View 2020 5Th Edition Laura A King Full Chaptergerald.chamberland888100% (5)
- Executive Function and Emotion Regulation - Strategy Use in AdolescentesDocument7 pagesExecutive Function and Emotion Regulation - Strategy Use in AdolescentesMiguel Ángel DominguezNo ratings yet
- Caile Ascendente Si Calea PiramidalaDocument4 pagesCaile Ascendente Si Calea PiramidalaLuca NicolaeNo ratings yet
- Lesson 5 - The Powers of The MindDocument4 pagesLesson 5 - The Powers of The MindCin DyNo ratings yet
- Full Download Test Bank For Discovering Behavioral Neuroscience An Introduction To Biological Psychology 3rd Edition PDF Full ChapterDocument36 pagesFull Download Test Bank For Discovering Behavioral Neuroscience An Introduction To Biological Psychology 3rd Edition PDF Full Chapterraving.odeleteux8100% (19)
- Neuroimage: Lukasz Smigielski, Milan Scheidegger, Michael Kometer, Franz X. VollenweiderDocument9 pagesNeuroimage: Lukasz Smigielski, Milan Scheidegger, Michael Kometer, Franz X. VollenweiderblondaylibraNo ratings yet
- Modelling The Human BrainDocument38 pagesModelling The Human BrainHuy NguyenNo ratings yet
- Superior Model School: Time: 1hr Subject: Mathematics Max Marks: Class: 6Document5 pagesSuperior Model School: Time: 1hr Subject: Mathematics Max Marks: Class: 6saifi_786No ratings yet
- The Brain NotesDocument42 pagesThe Brain Notessaswati biswalNo ratings yet
- Session 9Document27 pagesSession 9Quang Minh TrầnNo ratings yet
- Fulltext 01Document54 pagesFulltext 01Shafayet UddinNo ratings yet
- Intellectual DevelopmentDocument7 pagesIntellectual Developmentapi-639785554No ratings yet
- Mosconi-Sweeney2015 Article SensorimotorDysfunctionsAsPrimDocument8 pagesMosconi-Sweeney2015 Article SensorimotorDysfunctionsAsPrimEccoNo ratings yet