You might also like
- 20 Ways To Draw A CatDocument97 pages20 Ways To Draw A CatBishoy Elia93% (15)
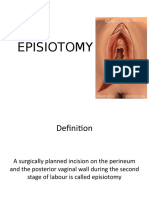
- EpisiotomyDocument30 pagesEpisiotomymob3100% (2)
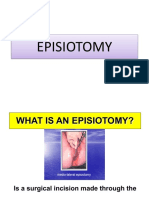
- EpisiotomyDocument30 pagesEpisiotomysubi100% (1)
- 2 Skin Preparation and DrapingDocument34 pages2 Skin Preparation and Drapingclaire yowsNo ratings yet
- Government College of Nursing: Procedure ONDocument6 pagesGovernment College of Nursing: Procedure ONpriyanka100% (6)
- Method Statement With Job Safety Analysis For Road Drains Culverts Road Crossover Final 16 07 2019Document32 pagesMethod Statement With Job Safety Analysis For Road Drains Culverts Road Crossover Final 16 07 2019Imranuddin SyedNo ratings yet
- Episiotomy: A Surgically Planned Incision On The Perineum and The Posterior Vaginal Wall During The Second Stage of LaborDocument27 pagesEpisiotomy: A Surgically Planned Incision On The Perineum and The Posterior Vaginal Wall During The Second Stage of LaborSanthosh.S.UNo ratings yet
- 1 Training Manual Prins TRAINING Manual PRINS VSI - PdfvsiDocument60 pages1 Training Manual Prins TRAINING Manual PRINS VSI - PdfvsiIoana Alexandra100% (1)
- MACW LTB 000000448 CV05042019 - Moorish American Consulate Removal and Acceptance-Decorey Christopher Pitts ElDocument16 pagesMACW LTB 000000448 CV05042019 - Moorish American Consulate Removal and Acceptance-Decorey Christopher Pitts ElSharon T Gale Bey100% (3)
- Injuries To The Birth CanalDocument67 pagesInjuries To The Birth CanalnamitaNo ratings yet
- EpisiotomyDocument29 pagesEpisiotomyhaisuresh100% (1)
- Radical Orchiectomy DURDocument17 pagesRadical Orchiectomy DURyulian salis patriawanNo ratings yet
- Genital Tract InjuriesDocument24 pagesGenital Tract InjuriesManisha ThakurNo ratings yet
- Episiotomy and Perineal TearsDocument21 pagesEpisiotomy and Perineal TearsJeevan VelanNo ratings yet
- EpisiotomyDocument6 pagesEpisiotomyNishaThakuri100% (1)
- Keihin-Everett Forwarding Co v. Tokio Marine Malayan Insurance Co. - Diligence Torts Subrogration PaymentDocument3 pagesKeihin-Everett Forwarding Co v. Tokio Marine Malayan Insurance Co. - Diligence Torts Subrogration PaymentJcNo ratings yet
- Assisting With Dilatation and Curettage ProcedureDocument3 pagesAssisting With Dilatation and Curettage ProceduremanjuNo ratings yet
- Skin Preparation FinalDocument4 pagesSkin Preparation FinalJerson EdilloNo ratings yet
- Assisting in Insertion of Intrauterine Contraceptive Device (Copper-T)Document4 pagesAssisting in Insertion of Intrauterine Contraceptive Device (Copper-T)manju100% (1)
- Demonstration On EpisiotomyDocument11 pagesDemonstration On EpisiotomyBabita DhruwNo ratings yet
- Assignmenton Episiotomy CareDocument5 pagesAssignmenton Episiotomy CarePriyaNo ratings yet
- Skill 23 Perform and Repair An EpisiotomyDocument2 pagesSkill 23 Perform and Repair An EpisiotomyThulasi tootsieNo ratings yet
- Curriculum PlanningDocument16 pagesCurriculum Planningmanju100% (3)
- Nhs Forth Valley: Perineal RepairDocument7 pagesNhs Forth Valley: Perineal RepairKamilah ShafiiNo ratings yet
- Episiotomy DefinitionDocument4 pagesEpisiotomy Definitionnursing school0% (1)
- Suturing An EpisiotomyDocument4 pagesSuturing An EpisiotomySumit YadavNo ratings yet
- Unit 9 Episiotomy and Nursing Management: 9.0 ObjectivesDocument8 pagesUnit 9 Episiotomy and Nursing Management: 9.0 ObjectivesSudip Kumar DeyNo ratings yet
- Procedure ON: EpisiotomyDocument7 pagesProcedure ON: EpisiotomyShalabh JoharyNo ratings yet
- Stage of Labour IIDocument30 pagesStage of Labour IIAdamu lawanNo ratings yet
- NVD With EpisiotomyDocument4 pagesNVD With EpisiotomySimran SimzNo ratings yet
- Episiotomy and SuturingDocument5 pagesEpisiotomy and SuturingAnila SajeshNo ratings yet
- Episiotomy 130403091515 Phpapp01Document12 pagesEpisiotomy 130403091515 Phpapp01Hamss AhmedNo ratings yet
- EPISIOTOMYDocument9 pagesEPISIOTOMYkailash chand atal100% (1)
- Procedure On Peforming and Suturing EpisiotomyDocument2 pagesProcedure On Peforming and Suturing Episiotomyshivani dasNo ratings yet
- Episiotomyror 181013114602Document27 pagesEpisiotomyror 181013114602Raluca HabaNo ratings yet
- EPISIOTOMY (Perineotomy)Document21 pagesEPISIOTOMY (Perineotomy)Abdullahi Suleiman MakaNo ratings yet
- Episiotomyprocedure 220126053356Document45 pagesEpisiotomyprocedure 220126053356nellius mutindiNo ratings yet
- Epi SutureDocument7 pagesEpi SutureyayitsnayNo ratings yet
- Nur 146 RleDocument47 pagesNur 146 RleKeziah Marie Chua Santa-AnaNo ratings yet
- EPISIOTOMYDocument17 pagesEPISIOTOMYKaye Arriane TenorioNo ratings yet
- EpisiotomyDocument2 pagesEpisiotomy007 Abhishek BindlishNo ratings yet
- Suturing Perineal Lacerations EditedDocument5 pagesSuturing Perineal Lacerations EditedJanzell Anne Borja AlbaniaNo ratings yet
- Episiotomy VideoDocument20 pagesEpisiotomy VideoEkram Gamal MorshedʚɞNo ratings yet
- Types of EpisiotomiesDocument2 pagesTypes of EpisiotomieskewpietheresaNo ratings yet
- Episeotomy Procedure, Care, ComplicationsDocument3 pagesEpiseotomy Procedure, Care, ComplicationsNejib M/AminNo ratings yet
- EPISIOTOMY FinalDocument30 pagesEPISIOTOMY FinalBindu PhilipNo ratings yet
- Episiotomy PDFDocument15 pagesEpisiotomy PDFNabighah ZukriNo ratings yet
- C Section Step by StepDocument2 pagesC Section Step by Stepj_nagelyNo ratings yet
- Circumcision Lecture NotesDocument45 pagesCircumcision Lecture NotesRoseNo ratings yet
- EpisiotomyDocument49 pagesEpisiotomyBharat ThapaNo ratings yet
- Operative Obstetrics: Madira Emmanuel Lira UniversityDocument27 pagesOperative Obstetrics: Madira Emmanuel Lira Universityvictor onapaNo ratings yet
- Or Write Up (Appendectomy) : Pines City Colleges College of NursingDocument9 pagesOr Write Up (Appendectomy) : Pines City Colleges College of Nursingthomasfinley44No ratings yet
- 9 - Soft Tissue InjuryDocument5 pages9 - Soft Tissue InjuryEastern SamarNo ratings yet
- Thora Procedure 1Document10 pagesThora Procedure 1E PadzNo ratings yet
- Perineal LacerationDocument16 pagesPerineal Lacerationbasman1212No ratings yet
- Rupture UterusDocument23 pagesRupture Uterushacker ammerNo ratings yet
- NCM 107 SKL FinalsDocument33 pagesNCM 107 SKL FinalsCyriz Ann Mae PacisNo ratings yet
- Episiotomy: By: Charisse Ann G. GasatayaDocument23 pagesEpisiotomy: By: Charisse Ann G. GasatayaCharisse Ann GasatayaNo ratings yet
- The Second Stage of LaborDocument11 pagesThe Second Stage of LaborZechariah NicholasNo ratings yet
- APPENDECTOMYDocument12 pagesAPPENDECTOMYayouNo ratings yet
- EpisiotomyDocument33 pagesEpisiotomyShruthi KumarNo ratings yet
- Episiotomy and RepairDocument20 pagesEpisiotomy and RepairwendeliciousNo ratings yet
- Zingaretti Et Al. 2019Document5 pagesZingaretti Et Al. 2019Walid SasiNo ratings yet
- Thoracentesis - ClinicalKey (1) (11-23)Document13 pagesThoracentesis - ClinicalKey (1) (11-23)jose luisNo ratings yet
- Birth Canal Injuries Final LectureDocument63 pagesBirth Canal Injuries Final Lecturepeter njoguNo ratings yet
- Surgical Procedure For Dehorning and Penile AmputationDocument17 pagesSurgical Procedure For Dehorning and Penile AmputationHikmat UllahNo ratings yet
- A Manual of the Operations of Surgery: For the Use of Senior Students, House Surgeons, and Junior PractitionersFrom EverandA Manual of the Operations of Surgery: For the Use of Senior Students, House Surgeons, and Junior PractitionersNo ratings yet
- Hydatidiform MoleDocument27 pagesHydatidiform MolemanjuNo ratings yet
- TeenagepregnancyDocument16 pagesTeenagepregnancymanjuNo ratings yet
- Reduction of Risk of The RadiationsDocument2 pagesReduction of Risk of The RadiationsmanjuNo ratings yet
- SimulationDocument22 pagesSimulationmanjuNo ratings yet
- Development Assistant Salary Grade 7 and Also License Inspector Salary 6 Thank You CBA 7 Professional Eligibility Required Some Professional Help Civil Service Exams on March Filing December So Good Luck That IDocument2 pagesDevelopment Assistant Salary Grade 7 and Also License Inspector Salary 6 Thank You CBA 7 Professional Eligibility Required Some Professional Help Civil Service Exams on March Filing December So Good Luck That ICaptain Armer D' LuffyNo ratings yet
- Fargo DTC550 Service Manual PDFDocument614 pagesFargo DTC550 Service Manual PDFnelutuanv-1No ratings yet
- 2010 PCDC Annual Spring Gala - Dinner JournalDocument86 pages2010 PCDC Annual Spring Gala - Dinner Journalpcdc1993No ratings yet
- Revisiting The Nifty Fifty: Valuing Growth StocksDocument5 pagesRevisiting The Nifty Fifty: Valuing Growth StocksbrineshrimpNo ratings yet
- Q02Document41 pagesQ02samy kookaNo ratings yet
- Greek Democracy: AssignmentDocument11 pagesGreek Democracy: AssignmentMahima RaoNo ratings yet
- A-12-02809 KMT ToolingSystems2013 SectionA KMDocument636 pagesA-12-02809 KMT ToolingSystems2013 SectionA KMdeepaNo ratings yet
- Hi-Pe High Performance Metal DetectorDocument2 pagesHi-Pe High Performance Metal Detectorhaitem burweenNo ratings yet
- Case Study: Manajemen Logistik & Rantai PasokDocument30 pagesCase Study: Manajemen Logistik & Rantai PasokDede AtmokoNo ratings yet
- 1000 State Bank of PakistanDocument4 pages1000 State Bank of PakistanRJNo ratings yet
- Two Ways AnovaDocument67 pagesTwo Ways AnovaQurratul AiniNo ratings yet
- SnowflakeDocument18 pagesSnowflakesaipriyacooolNo ratings yet
- E-283 (2) Gondi 930K PDFDocument1 pageE-283 (2) Gondi 930K PDFLuis Manuel CastilloNo ratings yet
- Ch1 - Sustainable DevelopmentDocument9 pagesCh1 - Sustainable DevelopmentLee Tin YanNo ratings yet
- PLDT v. City of Bacolod, G.R. No. 149179, July 15, 2005Document7 pagesPLDT v. City of Bacolod, G.R. No. 149179, July 15, 2005JamieNo ratings yet
- PantaloonsDocument17 pagesPantaloonsatishdkNo ratings yet
- Analisis Akun Twitter Berpengaruh Terkait Covid-19 Menggunakan SocialDocument8 pagesAnalisis Akun Twitter Berpengaruh Terkait Covid-19 Menggunakan SocialDodi AndriNo ratings yet
- Mphasis Buyback LOF Final 27 NovDocument77 pagesMphasis Buyback LOF Final 27 NovRajeshNo ratings yet
- AP PHYSICS B 1988 MC + AnswersDocument17 pagesAP PHYSICS B 1988 MC + AnswersbastardNo ratings yet
- Salesforce Sample Resume TemplateDocument4 pagesSalesforce Sample Resume TemplateGirishNo ratings yet
- Protect Yourself From These 7 ScamsDocument8 pagesProtect Yourself From These 7 ScamsKelsay HartNo ratings yet
- OB GYN Pages From Vmueller Snowdenpencer Armamentarium Catalogue 2Document36 pagesOB GYN Pages From Vmueller Snowdenpencer Armamentarium Catalogue 2Frechel Ann Landingin PedrozoNo ratings yet
- LESSOn 4-8Document39 pagesLESSOn 4-8Jemayka UlalanNo ratings yet
- JHMV102 Test 2 2019Document3 pagesJHMV102 Test 2 2019sithembeleNo ratings yet
- Implementation of EU Directives On Work-Life Balance and On Transparent and Predictable Working ConditionsDocument38 pagesImplementation of EU Directives On Work-Life Balance and On Transparent and Predictable Working ConditionsAdelina Elena OlogeanuNo ratings yet