You might also like
- FMS 1 - Week 7 Tutorial 1 LO PDFDocument17 pagesFMS 1 - Week 7 Tutorial 1 LO PDFAprillia AlmaasNo ratings yet
- CVS: Diuretics GuideDocument2 pagesCVS: Diuretics GuideCatNo ratings yet
- Mental Status Examination Medical StudentsDocument23 pagesMental Status Examination Medical StudentseurocoupeNo ratings yet
- Drugs For AsthmaDocument3 pagesDrugs For AsthmaMelissa Deso MillerNo ratings yet
- Week-2 Mental Status ExaminationDocument23 pagesWeek-2 Mental Status ExaminationSaud TariqNo ratings yet
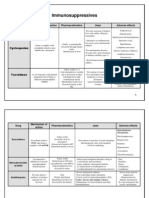
- Immunosuppressive Drugs Mechanisms Uses Side EffectsDocument4 pagesImmunosuppressive Drugs Mechanisms Uses Side EffectsUrugonda VenumadhavNo ratings yet
- Anatomy Ospe PDFDocument25 pagesAnatomy Ospe PDFrizki ardiansyahNo ratings yet
- St. Luke's College of Medicine - William H. Quasha Memorial: AnatomyDocument3 pagesSt. Luke's College of Medicine - William H. Quasha Memorial: AnatomyMavic VillanuevaNo ratings yet
- 4 Blood ProductsDocument11 pages4 Blood ProductsGampa VijaykumarNo ratings yet
- Immune System Docs 2019Document13 pagesImmune System Docs 2019David DavidNo ratings yet
- Hem-Onc: AnswerDocument3 pagesHem-Onc: AnswerAman Raj KNo ratings yet
- 03 The Cardiorespiratory SystemDocument24 pages03 The Cardiorespiratory SystemDuane N Lin WertNo ratings yet
- NSAIDs Guide to Mechanisms and MedicationsDocument20 pagesNSAIDs Guide to Mechanisms and MedicationsEvan Permana PutraNo ratings yet
- Immune System Review QuestionsDocument2 pagesImmune System Review Questionsapi-524061079No ratings yet
- Internal Medicine VivasDocument9 pagesInternal Medicine Vivasponcus payNo ratings yet
- Immune System Review QuestionsDocument2 pagesImmune System Review Questionsapi-521773978No ratings yet
- Case History M.SCDocument10 pagesCase History M.SCRaksha RNNo ratings yet
- Neisseria: Family Neisseriaceae With Four GeneraDocument26 pagesNeisseria: Family Neisseriaceae With Four GeneraAmit Mansukh MistryNo ratings yet
- CALCULATE TRANSFUSION VOLUMESDocument5 pagesCALCULATE TRANSFUSION VOLUMESKristine Mae AbrasaldoNo ratings yet
- Mohammad Altamimi, MD, PHD Jordan UniversityDocument16 pagesMohammad Altamimi, MD, PHD Jordan UniversityDaniel AtiehNo ratings yet
- Chest Pain Investigation, Diagnosis and TreatmentDocument4 pagesChest Pain Investigation, Diagnosis and TreatmentHadsabsaNo ratings yet
- Community OSCE.Document26 pagesCommunity OSCE.aaaskgamerNo ratings yet
- Respiratory AssessmentDocument43 pagesRespiratory AssessmentLui Andrei AnilaNo ratings yet
- Platelet, Coagulation, and Bleeding Disorder Diagnosis and TreatmentDocument11 pagesPlatelet, Coagulation, and Bleeding Disorder Diagnosis and TreatmentSara AshurstNo ratings yet
- SCB 204 Neural Integration and Motor ControlDocument6 pagesSCB 204 Neural Integration and Motor ControlWilliam TongNo ratings yet
- ECG Interpretation GuideDocument11 pagesECG Interpretation GuideJonathan DavisNo ratings yet
- 2a Haematology Saq QuestionsDocument12 pages2a Haematology Saq QuestionskamaluNo ratings yet
- Pap SmearDocument34 pagesPap Smearevi_ermaNo ratings yet
- Asthma DrugsDocument1 pageAsthma DrugskakuNo ratings yet
- Overview of AnaemiaDocument2 pagesOverview of AnaemiaGerardLumNo ratings yet
- Disoreder of PerceptionDocument36 pagesDisoreder of PerceptionUmar Khan100% (1)
- Endocrine Physiology & Pharmacology LecturesDocument22 pagesEndocrine Physiology & Pharmacology LecturesM Marliando Satria PangestuNo ratings yet
- Diuretic DrugsDocument2 pagesDiuretic DrugsEngku ElisaNo ratings yet
- Concise SEO-Optimized Title for Clotting DocumentDocument3 pagesConcise SEO-Optimized Title for Clotting DocumentRyan TurnerNo ratings yet
- Anti Viral DrugsDocument6 pagesAnti Viral DrugskakuNo ratings yet
- 3-Major Veins of The BodyDocument26 pages3-Major Veins of The BodyTJPlayz100% (1)
- Visual Phototransduction Is The SensoryDocument5 pagesVisual Phototransduction Is The SensoryNTA UGC-NETNo ratings yet
- Sensory Physiology Student ProtocolDocument18 pagesSensory Physiology Student ProtocolManuel Alejandro Chiguay GonzalezNo ratings yet
- Dr. Mahmmoud Ayish Lecture on AnemiaDocument21 pagesDr. Mahmmoud Ayish Lecture on AnemiaRashed ShatnawiNo ratings yet
- Anti Arrhythmic Anti Arrhythmic: Class IDocument1 pageAnti Arrhythmic Anti Arrhythmic: Class Inizam_ghaniNo ratings yet
- Histology PlacentaDocument26 pagesHistology Placentakhiks34100% (2)
- Table Summary For Gross Anatomy of Upper LimbDocument20 pagesTable Summary For Gross Anatomy of Upper Limbafifah zabidiNo ratings yet
- Acute Post Streptococcal Glomerulonephritis: DiseaseDocument3 pagesAcute Post Streptococcal Glomerulonephritis: DiseaseHades Luciferos PallonesNo ratings yet
- Neurological exam guide for medical studentsDocument13 pagesNeurological exam guide for medical studentslailatul husna100% (1)
- 1 6 Regulation of Blood Glucose PDFDocument3 pages1 6 Regulation of Blood Glucose PDFtiaraNo ratings yet
- Autoimmune Diseases: SLE, RA, and Thyroid ConditionsDocument47 pagesAutoimmune Diseases: SLE, RA, and Thyroid ConditionsGalih Putra RanggaNo ratings yet
- Immunosuppressant DrugsDocument87 pagesImmunosuppressant DrugsNagu KopparapuNo ratings yet
- Antiepileptic Drugs: Mechanisms of Action and Treatment OptionsDocument65 pagesAntiepileptic Drugs: Mechanisms of Action and Treatment OptionsZarish IftikharNo ratings yet
- Cell Inclusions: John SantangeloDocument45 pagesCell Inclusions: John Santangelosaint5470No ratings yet
- Assessing Musculoskeletal System Part 1Document30 pagesAssessing Musculoskeletal System Part 1Rodriguez MiaNo ratings yet
- Advances in Pathobiology and Management of Paget’s Disease of BoneFrom EverandAdvances in Pathobiology and Management of Paget’s Disease of BoneSakamuri V. ReddyNo ratings yet
- Pancoast Syndrome, (Apical Lung Cancer) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandPancoast Syndrome, (Apical Lung Cancer) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Cross Match TechniqueDocument5 pagesCross Match TechniqueANDREW MWITI100% (3)
- Drugs For Heart Failure: Drugs Catego Ry Drug Function Adverse Effect NoteDocument2 pagesDrugs For Heart Failure: Drugs Catego Ry Drug Function Adverse Effect NoteyukariNo ratings yet
- A Simple Guide to Hyperaldosteronism, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Hyperaldosteronism, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Deep Tendon Reflex Examination GuideDocument4 pagesDeep Tendon Reflex Examination GuideDan Ali100% (1)
- IV Fluid ChartDocument2 pagesIV Fluid Chartbenny christantoNo ratings yet
- Cranial Nerve Examination Part IDocument91 pagesCranial Nerve Examination Part IAARYANo ratings yet
- Data Collection Tool for Assessing Breastfeeding Knowledge and PracticesDocument1 pageData Collection Tool for Assessing Breastfeeding Knowledge and PracticesAmuNo ratings yet
- William Gouge: "There Is No Substitute For Mother'S Love, There Is No Substitute For Mothers Milk."Document2 pagesWilliam Gouge: "There Is No Substitute For Mother'S Love, There Is No Substitute For Mothers Milk."AmuNo ratings yet
- Breast Feeding PTTDocument1 pageBreast Feeding PTTAmuNo ratings yet
- Research TOOL FOR DATA COLLECTION PTTDocument1 pageResearch TOOL FOR DATA COLLECTION PTTAmuNo ratings yet
- There Is No Substitute For Mothers Milk.": William GougeDocument2 pagesThere Is No Substitute For Mothers Milk.": William GougeAmuNo ratings yet
- Baby Centre Medical Advisory BoardDocument1 pageBaby Centre Medical Advisory BoardAmuNo ratings yet
- Jain Philip Conducted A Descriptive Study To Assess The Knowledge and Practice Regarding Urinary Tract Infection During Pregnancy Among 80 Antenatal Mothers at Sreeramapuram Antenatal Clinic inDocument1 pageJain Philip Conducted A Descriptive Study To Assess The Knowledge and Practice Regarding Urinary Tract Infection During Pregnancy Among 80 Antenatal Mothers at Sreeramapuram Antenatal Clinic inAmuNo ratings yet
- A Randomized Controlled Pilot Study Was Conducted On Daily Cranberry Juice For The Prevention of Asymptomatic Bacteriurea in Pregnancy Among 188 WomenDocument1 pageA Randomized Controlled Pilot Study Was Conducted On Daily Cranberry Juice For The Prevention of Asymptomatic Bacteriurea in Pregnancy Among 188 WomenAmuNo ratings yet
- Most of The Mothers TTDocument1 pageMost of The Mothers TTAmuNo ratings yet
- Some of The Unhygienic Practices Like Unhygienic Bathing After 40 Days and Not Frequently Changing of PadDocument1 pageSome of The Unhygienic Practices Like Unhygienic Bathing After 40 Days and Not Frequently Changing of PadAmuNo ratings yet
- Determine The Prevalence of UTI Among Symptomatic and Asymptomatic Pregnant Women inDocument1 pageDetermine The Prevalence of UTI Among Symptomatic and Asymptomatic Pregnant Women inAmuNo ratings yet
- Urinary Tract Infection Is Caused by The Pathogenic MicroDocument1 pageUrinary Tract Infection Is Caused by The Pathogenic MicroAmuNo ratings yet
- Some of The Unhygienic Practices Like Unhygienic Bathing After 40 Days and Not Frequently Changing of PadDocument1 pageSome of The Unhygienic Practices Like Unhygienic Bathing After 40 Days and Not Frequently Changing of PadAmuNo ratings yet
- One of The Important Event in The Human Life Is BirthDocument1 pageOne of The Important Event in The Human Life Is BirthAmuNo ratings yet
- During PregnancyDocument1 pageDuring PregnancyAmuNo ratings yet
- The Aim Women Was To Compare Healing and Perineal Pain With The Use of Continuous and Interrupted Suture Techniques in Women After Normal DeliveryDocument1 pageThe Aim Women Was To Compare Healing and Perineal Pain With The Use of Continuous and Interrupted Suture Techniques in Women After Normal DeliveryAmuNo ratings yet
- One of The Important Event in The Human Life Is BirthDocument1 pageOne of The Important Event in The Human Life Is BirthAmuNo ratings yet
- Some of The Unhygienic Practices Like Unhygienic Bathing After 40 Days and Not Frequently Changing of PadDocument1 pageSome of The Unhygienic Practices Like Unhygienic Bathing After 40 Days and Not Frequently Changing of PadAmuNo ratings yet
- A Study Conducted On Survey On Postnatal Perineal MorbidityDocument1 pageA Study Conducted On Survey On Postnatal Perineal MorbidityAmuNo ratings yet
- The Association of Skin Infection Due To Urinary IncontinenceDocument1 pageThe Association of Skin Infection Due To Urinary IncontinenceAmuNo ratings yet
- Hygiene and Comfort Are Really Important After Birth Mothers Need To Change Pad Frequently To Stay Fresh and Help Prevent InfectionDocument1 pageHygiene and Comfort Are Really Important After Birth Mothers Need To Change Pad Frequently To Stay Fresh and Help Prevent InfectionAmuNo ratings yet
- Pregnancy Induced Hypertension Case StudyDocument75 pagesPregnancy Induced Hypertension Case StudyJing CruzNo ratings yet
- Pregnancy and Childbirth Related Complications Are The Leading Causes of Morbidity and Mortality Among Women of Reproductive Age in Developing CountriesDocument1 pagePregnancy and Childbirth Related Complications Are The Leading Causes of Morbidity and Mortality Among Women of Reproductive Age in Developing CountriesAmuNo ratings yet
- Hypertension-Guideline Approved 120716-1Document32 pagesHypertension-Guideline Approved 120716-1AmuNo ratings yet
- Perineal Hygiene Is A Procedure Employed To Clean The VulvaDocument1 pagePerineal Hygiene Is A Procedure Employed To Clean The VulvaAmuNo ratings yet
- Pregnancy and Childbirth Related Complications Are The Leading Causes of Morbidity and Mortality Among Women of Reproductive Age in Developing CountriesDocument1 pagePregnancy and Childbirth Related Complications Are The Leading Causes of Morbidity and Mortality Among Women of Reproductive Age in Developing CountriesAmuNo ratings yet
- Physiology and Management of Normal PuerperiumDocument132 pagesPhysiology and Management of Normal PuerperiumAmuNo ratings yet
- Diwali Offer PDFDocument14 pagesDiwali Offer PDFAmuNo ratings yet
- Review Cram SheetDocument57 pagesReview Cram Sheetjim j100% (1)
- Nursing Advanced Skills 1684126397. - PrintDocument421 pagesNursing Advanced Skills 1684126397. - PrintFahir ÖZBAYNo ratings yet
- COPD Patient Nursing Care PlanDocument2 pagesCOPD Patient Nursing Care PlanNicole SimoneNo ratings yet
- Cerebro Lys inDocument18 pagesCerebro Lys inKathleen PalomariaNo ratings yet
- Informative SpeechDocument3 pagesInformative Speechapi-27794699886% (7)
- Daftar Peralatan Elektromedik Menurut Ecri Dan WhoDocument4 pagesDaftar Peralatan Elektromedik Menurut Ecri Dan WhoAulia ArthaNo ratings yet
- Allen's Test (Wikipedia)Document2 pagesAllen's Test (Wikipedia)Anonymous LnWIBo1GNo ratings yet
- Chapter 12 Organophosphate PoisoningDocument13 pagesChapter 12 Organophosphate Poisoningarief muhammadNo ratings yet
- At-A-Glance Pocket Reference 2007Document8 pagesAt-A-Glance Pocket Reference 2007Arum PelangiNo ratings yet
- Research Essay Final WeeblyDocument12 pagesResearch Essay Final Weeblyapi-519040910No ratings yet
- Virtualreal Psychotherapeutic ToolDocument29 pagesVirtualreal Psychotherapeutic Toollic.evelincincottaNo ratings yet
- Continuous Passive Motion (CPM) : Theory and Principles of Clinical ApplicationDocument10 pagesContinuous Passive Motion (CPM) : Theory and Principles of Clinical ApplicationlaurentiaNo ratings yet
- DSM - IV ClassificationDocument13 pagesDSM - IV ClassificationSashi RajanNo ratings yet
- LPL - Lpl-Rohini (National Reference Lab) Sector - 18, Block - E Rohini DELHI 110085Document1 pageLPL - Lpl-Rohini (National Reference Lab) Sector - 18, Block - E Rohini DELHI 110085Vinothkumar VKNo ratings yet
- DR Pankaj NaramDocument20 pagesDR Pankaj NaramNitesh Kumar50% (6)
- BPHDocument20 pagesBPHHerly KakaNo ratings yet
- Monograph GarlicDocument2 pagesMonograph GarlicJoann PortugalNo ratings yet
- Prevalence and Risk Factors of Inguinal Hernia Study in A Semi-Urban Area in Rayalaseema, Andhra PradeshDocument4 pagesPrevalence and Risk Factors of Inguinal Hernia Study in A Semi-Urban Area in Rayalaseema, Andhra Pradeshsamsara vrindaNo ratings yet
- Bethesda 4Document5 pagesBethesda 4Pablo Gamez MontfortNo ratings yet
- Abortion BSN 0PR-2: Case Study of BelleDocument27 pagesAbortion BSN 0PR-2: Case Study of BellekervinNo ratings yet
- Pregnancy and Maternal Health: August 2019Document188 pagesPregnancy and Maternal Health: August 2019Katheryn RiañoNo ratings yet
- EXAM QUESTIONS On Wound Healing and Surgical Site InfectionsDocument2 pagesEXAM QUESTIONS On Wound Healing and Surgical Site Infectionsjc_sibal13No ratings yet
- Here's The Latest On COVID-19 VaccinesDocument45 pagesHere's The Latest On COVID-19 VaccinesLiar LiarNo ratings yet
- Aha Guidelinedriven Management of Hypertension An Evidencebased UpdateDocument56 pagesAha Guidelinedriven Management of Hypertension An Evidencebased UpdateNanda Gopal Reddy AnamNo ratings yet
- Q AND A RLE NCM 103 MergedDocument5 pagesQ AND A RLE NCM 103 MergedTADZMALYN JINANGNo ratings yet
- Chest Tube Thoracostomy ProcedureDocument17 pagesChest Tube Thoracostomy ProcedureJill Catherine CabanaNo ratings yet
- Activity - PT - With - Fluid & Lyte ImbalanceDocument3 pagesActivity - PT - With - Fluid & Lyte ImbalanceAngel Joy CatalanNo ratings yet
- Sensory Experience QuestionnaireDocument11 pagesSensory Experience QuestionnaireEdvaldo FreitasNo ratings yet
- 8feeding The Preterm InfantDocument5 pages8feeding The Preterm InfanttephaniNo ratings yet
- Angular ConjunctivitisDocument12 pagesAngular ConjunctivitisGhaniRahmaniNo ratings yet