You might also like
- 1 19 Osteoarthritis Year in Review Rehabilitatio 2011 Osteoarthritis and CADocument1 page1 19 Osteoarthritis Year in Review Rehabilitatio 2011 Osteoarthritis and CAEmad Tawfik AhmadNo ratings yet
- Hamstring 7Document7 pagesHamstring 7Ardhyan ArdhyanNo ratings yet
- A. Kasus: Clavicula) - Dokter Menyarankan Untuk Dilakukan Tindakan Operasi Yaitu Pemasangan FiksasiDocument6 pagesA. Kasus: Clavicula) - Dokter Menyarankan Untuk Dilakukan Tindakan Operasi Yaitu Pemasangan FiksasiRyan Luqman HNo ratings yet
- Total Knee Arthroplasty in Stiff Knee Compared With Exible KneesDocument7 pagesTotal Knee Arthroplasty in Stiff Knee Compared With Exible KneesNan SunshinerNo ratings yet
- Non-Pharmacological and Non-Surgical Interventions To Manage Patients With Knee Osteoarthritis: An Umbrella ReviewDocument20 pagesNon-Pharmacological and Non-Surgical Interventions To Manage Patients With Knee Osteoarthritis: An Umbrella ReviewBella MesantikaNo ratings yet
- Non Pharmacological and Non Surgical Interventions To Manage Patients With Knee Osteoarthritis An Umbrella Review FileDocument19 pagesNon Pharmacological and Non Surgical Interventions To Manage Patients With Knee Osteoarthritis An Umbrella Review FileCiocan AlexandraNo ratings yet
- Legnani2011 Article ManagementOfAnteriorCruciateLiDocument8 pagesLegnani2011 Article ManagementOfAnteriorCruciateLiZaro AnitaNo ratings yet
- Exercises Reduce The Progression Rate of Adolescent Idiopathic Scoliosis: Results of A Comprehensive Systematic Review of The LiteratureDocument14 pagesExercises Reduce The Progression Rate of Adolescent Idiopathic Scoliosis: Results of A Comprehensive Systematic Review of The LiteratureIvens NakagawaNo ratings yet
- Exercises Reduce The Progression Rate of Adolescent Idiopathic Scoliosis Results of A Comprehensive Systematic Review of The LiteratureDocument14 pagesExercises Reduce The Progression Rate of Adolescent Idiopathic Scoliosis Results of A Comprehensive Systematic Review of The Literatureeretria100% (1)
- Publication 31Document7 pagesPublication 31Tantia Dewi HariantoNo ratings yet
- Injury: E. Karam, F.S. Shivji, A. Bhattacharya, D.J. Bryson, D.P. Forward, B.E. Scammell, B.J. OllivereDocument5 pagesInjury: E. Karam, F.S. Shivji, A. Bhattacharya, D.J. Bryson, D.P. Forward, B.E. Scammell, B.J. OllivereMultazamNo ratings yet
- 1 s2.0 S0929664619300567 MainDocument8 pages1 s2.0 S0929664619300567 Mainananta restyNo ratings yet
- Physiotherapy After Tibial Plateau Fracture Fixation A Systematic Review of The Literature - PMCDocument1 pagePhysiotherapy After Tibial Plateau Fracture Fixation A Systematic Review of The Literature - PMCmf6wj6ccxqNo ratings yet
- Colibazzi Et Al 2020 Evidence Based Rehabilitation After Hip ArthroplastyDocument10 pagesColibazzi Et Al 2020 Evidence Based Rehabilitation After Hip ArthroplastyRafii KhairuddinNo ratings yet
- Skoliosis wydrukwPDFDocument20 pagesSkoliosis wydrukwPDFLusian VissNo ratings yet
- Early Versus Delayed Passive Range of Motion Exercise For Arthroscopic Rotator Cuff RepairDocument9 pagesEarly Versus Delayed Passive Range of Motion Exercise For Arthroscopic Rotator Cuff RepairJane Elisabeth WauranNo ratings yet
- The Results of Kinesiotaping in Patients With Scoliosis: Kiselev D.A., Gubanov V.V., Laysheva O.A., Tuchkov V.EDocument14 pagesThe Results of Kinesiotaping in Patients With Scoliosis: Kiselev D.A., Gubanov V.V., Laysheva O.A., Tuchkov V.Ealaawagdybv2No ratings yet
- ArticleDocument14 pagesArticleAndrey LingNo ratings yet
- MG 1Document7 pagesMG 1Cristobal Ramirez FacusseNo ratings yet
- 2014 Return To Sport After ACL ReconstructionDocument6 pages2014 Return To Sport After ACL ReconstructionJaime Fernandez FernandezNo ratings yet
- Core 2Document8 pagesCore 2Jenny VibsNo ratings yet
- Art - Equilibrio y PropiocepcionDocument7 pagesArt - Equilibrio y PropiocepcionYuLyChNo ratings yet
- 1 s2.0 S1836955319300918 Main PDFDocument7 pages1 s2.0 S1836955319300918 Main PDFJuliano BritoNo ratings yet
- SEAS (Scientific Exercises Approach To Scoliosis) : A Modern and Effective Evidence Based Approach To Physiotherapic Specific Scoliosis ExercisesDocument20 pagesSEAS (Scientific Exercises Approach To Scoliosis) : A Modern and Effective Evidence Based Approach To Physiotherapic Specific Scoliosis ExercisesLâm Đặng ĐứcNo ratings yet
- Rotator Cuff Repair vs. Nonoperative Treatment - 2021 (Tema 3)Document12 pagesRotator Cuff Repair vs. Nonoperative Treatment - 2021 (Tema 3)Carlos NoronaNo ratings yet
- Scoliosis BraceDocument8 pagesScoliosis BraceChandralina PakpahanNo ratings yet
- Stasinopoulos 2012Document8 pagesStasinopoulos 2012toaldoNo ratings yet
- Ejh 110 253Document9 pagesEjh 110 253Diogo GadelhaNo ratings yet
- C Rioter ApyDocument6 pagesC Rioter ApyDanNy ClaudiuNo ratings yet
- Knee Osteoarthritis Impact On Quality of Life Andeffectiveness of Total Knee ArthroplastyDocument6 pagesKnee Osteoarthritis Impact On Quality of Life Andeffectiveness of Total Knee ArthroplastyWeasleNotNo ratings yet
- Acl N PilatesDocument8 pagesAcl N PilatesDeva JCNo ratings yet
- Comparison of Effects of Abdominal Draw-InDocument9 pagesComparison of Effects of Abdominal Draw-InYoh ChenNo ratings yet
- The Effectiveness of Core Stabilization Exercise in Adolescent Idiopathic Scoliosis: A Randomized Controlled TrialDocument8 pagesThe Effectiveness of Core Stabilization Exercise in Adolescent Idiopathic Scoliosis: A Randomized Controlled Triali pentungNo ratings yet
- 8Document1 page8Daniel GuevaraNo ratings yet
- Miralles 2016Document6 pagesMiralles 2016Khalid AhmedNo ratings yet
- 2018 Article 2834Document11 pages2018 Article 2834mitroisergiuNo ratings yet
- 4 03000605221103974Document13 pages4 03000605221103974Teuku FadhliNo ratings yet
- I C M M, M O, H P A M T P - F H P: A R C TDocument9 pagesI C M M, M O, H P A M T P - F H P: A R C TAngie D. AndradesNo ratings yet
- 1 s2.0 S1836955321000540 MainDocument13 pages1 s2.0 S1836955321000540 MainAyu SuprabawatiNo ratings yet
- 1 s2.0 S0020138313005718 MainDocument7 pages1 s2.0 S0020138313005718 MainMutiara Rachmawati ViorhaNo ratings yet
- Role of Continuous Passive Motion of Elbow To Improve Feeding in Stroke A Comparative StudyDocument5 pagesRole of Continuous Passive Motion of Elbow To Improve Feeding in Stroke A Comparative StudyResearch ParkNo ratings yet
- Kraus 2021Document7 pagesKraus 2021翁嘉聰No ratings yet
- Para Tradudir Ejercisios y Espondilitis AnquilosanteDocument10 pagesPara Tradudir Ejercisios y Espondilitis AnquilosanteCarla Bocca MoralesNo ratings yet
- Mandibular Changes Produced by Functional Appliances in Class II Malocclusion: A Systematic ReviewDocument13 pagesMandibular Changes Produced by Functional Appliances in Class II Malocclusion: A Systematic ReviewSai KrupaNo ratings yet
- Anterior Cruciate Ligament Reconstruction Rehabilitation: MOON GuidelinesDocument5 pagesAnterior Cruciate Ligament Reconstruction Rehabilitation: MOON GuidelinesSilvy OktavianaNo ratings yet
- Effecthiparthroplasy 2012Document10 pagesEffecthiparthroplasy 2012JESSICA OQUENDO OROZCONo ratings yet
- Comparison of Aggressive and Traditional Postoperative Rehabilitation Protocol After Rotator Cuff Repair: A Meta-AnalysisDocument6 pagesComparison of Aggressive and Traditional Postoperative Rehabilitation Protocol After Rotator Cuff Repair: A Meta-AnalysisNico BrantesNo ratings yet
- The Study To Assess The Effect of Prehabilitation On Postoperative Outcome of The Patients On Total Knee Arthroplasty at Selected HospitalDocument4 pagesThe Study To Assess The Effect of Prehabilitation On Postoperative Outcome of The Patients On Total Knee Arthroplasty at Selected HospitalEditor IJTSRDNo ratings yet
- Ankle Sprain CPR For ManipulationDocument13 pagesAnkle Sprain CPR For ManipulationChaim MalineNo ratings yet
- 189-198 FukatoVol8No3 PDFDocument10 pages189-198 FukatoVol8No3 PDFIndah YulantariNo ratings yet
- Hyaluronic Acid Single Intra-Articular Injection IDocument12 pagesHyaluronic Acid Single Intra-Articular Injection IMos Viorel DanutNo ratings yet
- PSR Module 2 - Web CourseDocument101 pagesPSR Module 2 - Web CourseAndrei R LupuNo ratings yet
- Specific Exercises Reduce The Need For Bracing in Adolescents With Idiopathic Scoliosis - A Practical Clinical TrialDocument8 pagesSpecific Exercises Reduce The Need For Bracing in Adolescents With Idiopathic Scoliosis - A Practical Clinical TrialAriella GandraNo ratings yet
- Negrini 2Document5 pagesNegrini 2iguija6769No ratings yet
- Evidence-Based Treatment Choices For Acute Lateral Ankle Sprain: A Comprehensive Systematic ReviewDocument9 pagesEvidence-Based Treatment Choices For Acute Lateral Ankle Sprain: A Comprehensive Systematic ReviewMilton RezzaNo ratings yet
- Abenavoli 2020Document7 pagesAbenavoli 2020consueloamado.medNo ratings yet
- Knee OADocument10 pagesKnee OAInaauliahanNo ratings yet
- 9 - 5 - The Effect of Mirror Therapy On Balance Ability of Subacute Stroke Patients - Bella Syafitri PDFDocument6 pages9 - 5 - The Effect of Mirror Therapy On Balance Ability of Subacute Stroke Patients - Bella Syafitri PDFAkhyar FtNo ratings yet
- Anterior Open Bite Correction Using Bite Block ACase ReportDocument6 pagesAnterior Open Bite Correction Using Bite Block ACase ReportRommy MelgarejoNo ratings yet
- Introduction To The Three-Dimensional Scoliosis Treatment According To SchrothDocument6 pagesIntroduction To The Three-Dimensional Scoliosis Treatment According To SchrothIvens NakagawaNo ratings yet
- Gichul Kim 2016Document4 pagesGichul Kim 2016Ivens NakagawaNo ratings yet
- Weiss2003 PDFDocument8 pagesWeiss2003 PDFIvens NakagawaNo ratings yet
- 1748 7161 6 17Document22 pages1748 7161 6 17cristdara100% (1)
- Saltikov 2014Document39 pagesSaltikov 2014Ivens NakagawaNo ratings yet
- Exercises Reduce The Progression Rate of Adolescent Idiopathic Scoliosis: Results of A Comprehensive Systematic Review of The LiteratureDocument14 pagesExercises Reduce The Progression Rate of Adolescent Idiopathic Scoliosis: Results of A Comprehensive Systematic Review of The LiteratureIvens NakagawaNo ratings yet
- EN Paper-5Document11 pagesEN Paper-5isabellemdelmasNo ratings yet
- M.S Engineering (Aerospace) Application Form: For Office UseDocument4 pagesM.S Engineering (Aerospace) Application Form: For Office Useshashasha123No ratings yet
- 66 Essential Phrasal Verbs EnglishDocument6 pages66 Essential Phrasal Verbs EnglishNarcisVega100% (15)
- Chapter 12.1.2 Respiratory Substrates and RQDocument30 pagesChapter 12.1.2 Respiratory Substrates and RQnie20060301No ratings yet
- Inkubator TransportDocument8 pagesInkubator TransportYassarNo ratings yet
- PHY130 Lab Report 2Document7 pagesPHY130 Lab Report 2Declan Gale Anak DellyNo ratings yet
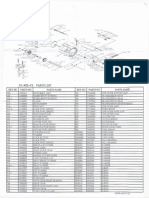
- Okuma CL302L Parts List & ManualDocument3 pagesOkuma CL302L Parts List & Manualcoolestkiwi100% (1)
- Phy Interface Pci Express Sata Usb31 Architectures Ver43 PDFDocument99 pagesPhy Interface Pci Express Sata Usb31 Architectures Ver43 PDFRaj Shekhar ReddyNo ratings yet
- AWS Abbreviations Oxyfuel Cutting - OFC Oxyacetylene Cutting - OFC-A Oxyfuel Cutting - Process and Fuel GasesDocument8 pagesAWS Abbreviations Oxyfuel Cutting - OFC Oxyacetylene Cutting - OFC-A Oxyfuel Cutting - Process and Fuel GasesahmedNo ratings yet
- C Ce 200Document59 pagesC Ce 200hanieh rezapourNo ratings yet
- Important Notice About The GPS Week-Number Roll-Over ProblemDocument12 pagesImportant Notice About The GPS Week-Number Roll-Over ProblemFred 2RockstarNo ratings yet
- Kompilasi Soal Paket BDocument10 pagesKompilasi Soal Paket Babdul wahidNo ratings yet
- Competency Based Learning Materials: Housekeeping NciiDocument54 pagesCompetency Based Learning Materials: Housekeeping NciiNickolodian AsuncionNo ratings yet
- BT JOE Quiz 4 MasonryDocument1 pageBT JOE Quiz 4 Masonrycorazon phil100% (1)
- Snowflake Schema - JennyDocument2 pagesSnowflake Schema - JennyJennyNo ratings yet
- TDBFP - Gear Pump API 676 PDFDocument42 pagesTDBFP - Gear Pump API 676 PDFRamon A. Ruiz O.No ratings yet
- 08 LCD Slide Handout 1Document5 pages08 LCD Slide Handout 1Jana Gabrielle Canonigo0% (1)
- Taxation - Deduction - Quizzer - CPA Review - 2017Document6 pagesTaxation - Deduction - Quizzer - CPA Review - 2017Kenneth Bryan Tegerero Tegio100% (1)
- Filcro - LabrevDocument19 pagesFilcro - LabrevKim ArniñoNo ratings yet
- A Simple and Convenient Synthesis of Pseudo Ephedrine From N-MethylamphetamineDocument2 pagesA Simple and Convenient Synthesis of Pseudo Ephedrine From N-Methylamphetaminedh329No ratings yet
- File Handling in Python PDFDocument25 pagesFile Handling in Python PDFNileshNo ratings yet
- Shenkar 2001 Cultural Distance RevisitedDocument17 pagesShenkar 2001 Cultural Distance RevisitedMalthe EriksenNo ratings yet
- Product Positioning & Promotional Strategy of FevicolDocument5 pagesProduct Positioning & Promotional Strategy of FevicolBhat NaieemNo ratings yet
- Cheats BFG Doom 3Document5 pagesCheats BFG Doom 3screw_x3No ratings yet
- Cancer Registry Standard Operating ProceduresDocument3 pagesCancer Registry Standard Operating ProceduresAnan AghbarNo ratings yet
- CostcoDocument12 pagesCostcoThảo Nguyên PhạmNo ratings yet
- Passive Voice PDFDocument5 pagesPassive Voice PDFJohan FloresNo ratings yet
- Tutorial Set (Queing Model)Document5 pagesTutorial Set (Queing Model)Samuel kwateiNo ratings yet
- 46GA On Designers For CEED, UCEED and NID - Stuff You LookDocument3 pages46GA On Designers For CEED, UCEED and NID - Stuff You LookReshmi Varma100% (1)
- Scheme and Syllabus of B.E. (Computer Science and Engineering) 3 TO8 Semester 2017-2018Document170 pagesScheme and Syllabus of B.E. (Computer Science and Engineering) 3 TO8 Semester 2017-2018pratik YadavNo ratings yet
- Stable Relation: A Memoir of One Woman's Spirited Journey Home, by Way of the BarnFrom EverandStable Relation: A Memoir of One Woman's Spirited Journey Home, by Way of the BarnRating: 5 out of 5 stars5/5 (4)
- Horse Care 101: How to Take Care of a Horse for BeginnersFrom EverandHorse Care 101: How to Take Care of a Horse for BeginnersRating: 4 out of 5 stars4/5 (5)
- The Everything Horse Book: Buying, riding, and caring for your equine companionFrom EverandThe Everything Horse Book: Buying, riding, and caring for your equine companionRating: 2 out of 5 stars2/5 (1)
- Joey: How a Blind Rescue Horse Helped Others Learn to SeeFrom EverandJoey: How a Blind Rescue Horse Helped Others Learn to SeeRating: 5 out of 5 stars5/5 (23)
- Hoof Physics: How to Recognize the Signs of Hoof DistortionFrom EverandHoof Physics: How to Recognize the Signs of Hoof DistortionRating: 5 out of 5 stars5/5 (1)
- The Faraway Horses: The Adventures and Wisdom of America's Most Renowned HorsemenFrom EverandThe Faraway Horses: The Adventures and Wisdom of America's Most Renowned HorsemenRating: 4.5 out of 5 stars4.5/5 (49)
- Fitness Evaluation of the HorseFrom EverandFitness Evaluation of the HorseRating: 5 out of 5 stars5/5 (1)
- Groundwork with horses: Natural Horsemanship & Groundwork Training for Your HorseFrom EverandGroundwork with horses: Natural Horsemanship & Groundwork Training for Your HorseNo ratings yet
- Project Solomon: The True Story of a Lonely Horse Who Found a Home--and Became a HeroFrom EverandProject Solomon: The True Story of a Lonely Horse Who Found a Home--and Became a HeroRating: 5 out of 5 stars5/5 (9)
- Milo's Eyes: How a Blind Equestrian and Her "Seeing Eye Horse" Rescued Each OtherFrom EverandMilo's Eyes: How a Blind Equestrian and Her "Seeing Eye Horse" Rescued Each OtherRating: 5 out of 5 stars5/5 (2)
- Whole Heart, Whole Horse: Building Trust Between Horse and RiderFrom EverandWhole Heart, Whole Horse: Building Trust Between Horse and RiderRating: 5 out of 5 stars5/5 (9)
- 101 Fun Facts and Trivia About Horses: All You Need To Know If You Are Crazy About HorsesFrom Everand101 Fun Facts and Trivia About Horses: All You Need To Know If You Are Crazy About HorsesNo ratings yet
- The Equine Listenology Guide - Essential Horsemanship, Horse Body Language & Behaviour, Groundwork, In-hand Exercises & Riding Lessons to Develop Softness, Connection & Collection.From EverandThe Equine Listenology Guide - Essential Horsemanship, Horse Body Language & Behaviour, Groundwork, In-hand Exercises & Riding Lessons to Develop Softness, Connection & Collection.Rating: 5 out of 5 stars5/5 (1)
- Building Your Dream Horse: Charles Wilhelm's Ultimate Foundation TrainingFrom EverandBuilding Your Dream Horse: Charles Wilhelm's Ultimate Foundation TrainingRating: 4 out of 5 stars4/5 (4)
- The Everything Horse Care Book: A Complete Guide to the Well-being of Your HorseFrom EverandThe Everything Horse Care Book: A Complete Guide to the Well-being of Your HorseNo ratings yet
- The Ultimate Book of Horse Bits: What They Are, What They Do, and How They Work (2nd Edition)From EverandThe Ultimate Book of Horse Bits: What They Are, What They Do, and How They Work (2nd Edition)Rating: 5 out of 5 stars5/5 (1)
- Horses: 101 Super Fun Facts and Amazing Pictures (Featuring The World's Top 18 Horse Breeds)From EverandHorses: 101 Super Fun Facts and Amazing Pictures (Featuring The World's Top 18 Horse Breeds)Rating: 3.5 out of 5 stars3.5/5 (11)
- There's More to Training Horses: 100 Tips, 100 Days, 100% BetterFrom EverandThere's More to Training Horses: 100 Tips, 100 Days, 100% BetterNo ratings yet
- Horse training simply explained: Basic Horse training, Foal training, Natural Horsemanship and much moreFrom EverandHorse training simply explained: Basic Horse training, Foal training, Natural Horsemanship and much moreNo ratings yet