You might also like
- DepED Letterhead (A4)Document2 pagesDepED Letterhead (A4)Levi CorralNo ratings yet
- Equivalent Record FormDocument1 pageEquivalent Record Formbheybie0822No ratings yet
- Special Order Granting of Service Credits: Tarlac City Schools DivisionDocument1 pageSpecial Order Granting of Service Credits: Tarlac City Schools DivisionMarlon C. RufoNo ratings yet
- Attachment No. 4 (Program M & E Report) : On-Site Monitoring and Evaluation Basic InformationDocument12 pagesAttachment No. 4 (Program M & E Report) : On-Site Monitoring and Evaluation Basic Informationconnie saunar100% (1)
- Constructivist Instructional Techniques Observation and Rating SheetDocument2 pagesConstructivist Instructional Techniques Observation and Rating SheetJheryl Malapad Fortun-Guibelondo100% (3)
- Ms. Lance Concon Fortune Miler Exceed 10: 20 Year(s) Old P50,000Document2 pagesMs. Lance Concon Fortune Miler Exceed 10: 20 Year(s) Old P50,000Ryana ConconNo ratings yet
- Brigada Service CreditsDocument2 pagesBrigada Service CreditsLea LaderaNo ratings yet
- Checking of Forms 2020 SHSDocument2 pagesChecking of Forms 2020 SHSNancy AtentarNo ratings yet
- Certificate As HostDocument5 pagesCertificate As HostKenny Ann Grace BatiancilaNo ratings yet
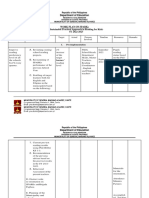
- Department of Education: Work Plan On Sparks (Sustainable Practical Approach in Reading For Kids) SY 2022-2023Document24 pagesDepartment of Education: Work Plan On Sparks (Sustainable Practical Approach in Reading For Kids) SY 2022-2023JOANE PACATANGNo ratings yet
- Sarimanok Seal of Excellence in Classroom ManagementDocument7 pagesSarimanok Seal of Excellence in Classroom ManagementMyla AhmadNo ratings yet
- Output Checklist Quality Assessment Criteria Available 1 Yes 0 No Reviewer Comments (What Needs Improvement? or Total Revision?)Document9 pagesOutput Checklist Quality Assessment Criteria Available 1 Yes 0 No Reviewer Comments (What Needs Improvement? or Total Revision?)Guitnang bayan es 109487No ratings yet
- LIS Justification LetterDocument2 pagesLIS Justification LetterRENEJANE ABALLE0% (1)
- Ro1 LQF Qad 017Document4 pagesRo1 LQF Qad 017MichiOdevilasNo ratings yet
- Quality Form Oplan Kalusugan Sa Deped Accomplishment Report FormDocument24 pagesQuality Form Oplan Kalusugan Sa Deped Accomplishment Report FormJoules Laureta Fabros GaleraNo ratings yet
- Learning Camp RegistrationDocument1 pageLearning Camp RegistrationAaron James LicoNo ratings yet
- 2019 Revised SIP Annex 1A School Community Data Template 10302015Document23 pages2019 Revised SIP Annex 1A School Community Data Template 10302015Jacqueline Resma FloresNo ratings yet
- Schedule of Activities On The Implementation of LDM Course 2Document2 pagesSchedule of Activities On The Implementation of LDM Course 2JaniceTasarraFulgueras100% (1)
- 11 Dorp Froms EsDocument11 pages11 Dorp Froms EsGeoffrey MilesNo ratings yet
- Learning Resource (S) Mapping: Republic of The PhilippinesDocument2 pagesLearning Resource (S) Mapping: Republic of The PhilippinesElectra AmorNo ratings yet
- IPPDDocument2 pagesIPPDMarisa B. CanoNo ratings yet
- Individual Performance Commitment and Review Form (Ipcrf) : User GuideDocument32 pagesIndividual Performance Commitment and Review Form (Ipcrf) : User GuideZaldy TabugocaNo ratings yet
- LAC-SESSION-test ConstructionDocument2 pagesLAC-SESSION-test Constructionjesielz100% (1)
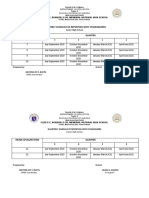
- Quarterly Schedule of Reporting With StakeholdersDocument2 pagesQuarterly Schedule of Reporting With StakeholdersAngelica DalitNo ratings yet
- Don Jose Ynares Sr. Memorial National High School: Population: SYDocument2 pagesDon Jose Ynares Sr. Memorial National High School: Population: SYJudy Panguito AralarNo ratings yet
- Ligaya Annual Supervisory Plan 2020Document7 pagesLigaya Annual Supervisory Plan 2020Emmanuel RecodoNo ratings yet
- Classroom Evaluation ChecklistDocument1 pageClassroom Evaluation ChecklistChel GualbertoNo ratings yet
- Cerificate of Non AvailabilityDocument1 pageCerificate of Non AvailabilityVenus Soriano100% (1)
- Accomplishment Report in The Implementation of The Customized Division Technical Assistance Plan (Cdtap)Document3 pagesAccomplishment Report in The Implementation of The Customized Division Technical Assistance Plan (Cdtap)William FelisildaNo ratings yet
- SardoDocument30 pagesSardoPaul Senen DiduloNo ratings yet
- Department of Education: Republic of The PhilippinesDocument22 pagesDepartment of Education: Republic of The PhilippinesSheryl Cruz EspirituNo ratings yet
- Minutes August 10, 2020Document4 pagesMinutes August 10, 2020GeanAnnSalazarLingling-Jao100% (1)
- ADAS II Competency ProfileDocument3 pagesADAS II Competency Profilechoco chip 0629100% (1)
- Learner's Needs, Progress and Achievement CardexDocument3 pagesLearner's Needs, Progress and Achievement CardexJeremie Mariano AbanNo ratings yet
- Duties and Responsibilities of GrievanceDocument3 pagesDuties and Responsibilities of GrievanceRhadbhel PulidoNo ratings yet
- Guidelines On The Checking of FormsDocument57 pagesGuidelines On The Checking of FormsArnoldBaladjayNo ratings yet
- Brigada Eskwela Form 1: Satisfactor Y Unsatisfactor Y If Unsatisfactory, Describe The ProblemDocument28 pagesBrigada Eskwela Form 1: Satisfactor Y Unsatisfactor Y If Unsatisfactory, Describe The ProblemjmNo ratings yet
- 8th Div Technolympics Memo - Signed PDFDocument40 pages8th Div Technolympics Memo - Signed PDFIaney Minguez EstarisNo ratings yet
- Aip App PPMPDocument88 pagesAip App PPMPJeurdecel Laborada Castro - MartizanoNo ratings yet
- JDM Sdo Sgod 1 Chief Eps Sm&e Socmob 30april14Document34 pagesJDM Sdo Sgod 1 Chief Eps Sm&e Socmob 30april14Juan Obierna100% (1)
- ERF and Reclass PDFDocument2 pagesERF and Reclass PDFSamuel EgallaNo ratings yet
- Ippd Form 1 - Teacher'S Individual Plan For Professional Development (Ippd) SCHOOL YEAR: 2017-2018Document6 pagesIppd Form 1 - Teacher'S Individual Plan For Professional Development (Ippd) SCHOOL YEAR: 2017-2018MarkNo ratings yet
- Community Project Proposal Sample PDFDocument6 pagesCommunity Project Proposal Sample PDFPistol SamNo ratings yet
- 2019 Early Registration TemplateDocument12 pages2019 Early Registration TemplateClifford Tungpalan BorromeoNo ratings yet
- Checklist of Submitted Teacher's Requirements Year End DEpedDocument16 pagesChecklist of Submitted Teacher's Requirements Year End DEpedKristine BarredoNo ratings yet
- Star Observation Form 2023 2024Document4 pagesStar Observation Form 2023 2024Jane ImperialNo ratings yet
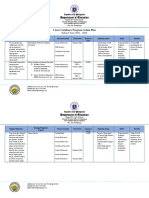
- Department of Education: Career Guidance Program Action PlanDocument4 pagesDepartment of Education: Career Guidance Program Action PlanKathleen Deldoc-AbetoNo ratings yet
- SDO Camarines Norte: Facilitating Dreams, Valuing AspirationsDocument6 pagesSDO Camarines Norte: Facilitating Dreams, Valuing AspirationsZyra CabarleNo ratings yet
- Enclosure No. 2 Revised L D Form For INSETDocument10 pagesEnclosure No. 2 Revised L D Form For INSETJoselito S. CuisonNo ratings yet
- Master Teachers: Implementing Rules and RegulationsDocument19 pagesMaster Teachers: Implementing Rules and RegulationsChristine PobleteNo ratings yet
- Lesson Plan in ENGLISH 3 DemoDocument5 pagesLesson Plan in ENGLISH 3 DemoCris Nanette Arcenas100% (1)
- SLRP Approval SheetDocument3 pagesSLRP Approval SheetJolina NacpilNo ratings yet
- Certificate For ESATDocument1 pageCertificate For ESATVladimer Pionilla100% (1)
- DM HROD 2021 0011 Supporting Documents To DepEd Streamlining For PBBDocument7 pagesDM HROD 2021 0011 Supporting Documents To DepEd Streamlining For PBBjanette riveraNo ratings yet
- School Form 7 (SF7)Document9 pagesSchool Form 7 (SF7)Dennis Reyes67% (3)
- Contingency Plan Tool KitDocument24 pagesContingency Plan Tool KitGWEN BORRELNo ratings yet
- I.Program Implementation Progress: ST ND RD THDocument3 pagesI.Program Implementation Progress: ST ND RD THKaren BlythNo ratings yet
- Lyceum of Alabang Inc: Basic Education DepartmentDocument2 pagesLyceum of Alabang Inc: Basic Education DepartmentRham GidaNo ratings yet
- 2021 2022 Learner Enrollment and Survey Form - v8 - EnglishDocument3 pages2021 2022 Learner Enrollment and Survey Form - v8 - EnglishJeferson Eborda RoselNo ratings yet
- Transmital Letter McisDocument1 pageTransmital Letter McisThe Great PapyrusNo ratings yet
- Exit PlanDocument9 pagesExit PlanThe Great PapyrusNo ratings yet
- Exit Plan SSCDocument1 pageExit Plan SSCThe Great PapyrusNo ratings yet
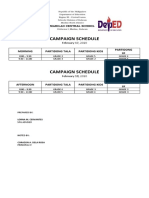
- Schedule of CampaignDocument1 pageSchedule of CampaignThe Great PapyrusNo ratings yet
- SPG Election 2020 SPG Election 2020 SPG Election 2020Document2 pagesSPG Election 2020 SPG Election 2020 SPG Election 2020The Great PapyrusNo ratings yet
- SCIENCE Elem. Matrix For The Learning Continuity PlanDocument7 pagesSCIENCE Elem. Matrix For The Learning Continuity PlanThe Great Papyrus100% (1)
- Economic Reforms of 1991Document21 pagesEconomic Reforms of 1991somnathmangarajNo ratings yet
- Bhagavad Gita Marathi - Adhyay 11Document28 pagesBhagavad Gita Marathi - Adhyay 11aekay100% (2)
- Lecture 1Document87 pagesLecture 1Raymer OclaritNo ratings yet
- IT and Computer ApplicationDocument4 pagesIT and Computer ApplicationJunaid SarwarNo ratings yet
- Argana vs. RepublicDocument31 pagesArgana vs. RepublicMark NoelNo ratings yet
- BARNES Et Al - Contribution of Anthropology To The Study of Climate ChangeDocument4 pagesBARNES Et Al - Contribution of Anthropology To The Study of Climate ChangeAnna JéssicaNo ratings yet
- Apendice 5 Asme VIII 2 PDFDocument12 pagesApendice 5 Asme VIII 2 PDFBrendaNo ratings yet
- Hexco March 2014 Engineering MathsDocument3 pagesHexco March 2014 Engineering MathsNdumiso MoyoNo ratings yet
- Module 3: Reflection Paper 2 Juliann Macnicoll Pacific Oaks College HD 315: The Art of Observation Terry Stone 5/24/17Document5 pagesModule 3: Reflection Paper 2 Juliann Macnicoll Pacific Oaks College HD 315: The Art of Observation Terry Stone 5/24/17api-379926458No ratings yet
- LABORATORY EXERCISE The Gastrointestinal System With Accessory GlandDocument5 pagesLABORATORY EXERCISE The Gastrointestinal System With Accessory GlandGelo AlonzoNo ratings yet
- Summer Training Report: Submitted To: DR Ranu Sharma Submitted By: Charu SinghDocument47 pagesSummer Training Report: Submitted To: DR Ranu Sharma Submitted By: Charu SinghAbhishek KachhawalNo ratings yet
- Accounting 202 Chapter 15 TestansquestiDocument4 pagesAccounting 202 Chapter 15 TestansquestiSandra ReidNo ratings yet
- Old Man and The SeaDocument22 pagesOld Man and The Seaapi-268644570No ratings yet
- Brand Meaning - Mark BateyDocument2 pagesBrand Meaning - Mark BateyMartin Guy ChoquetteNo ratings yet
- Lesson PlanDocument2 pagesLesson Planapi-584057836No ratings yet
- Carpediemconsulting's Blog: Row Wise Initialized Variable in OBIEE 11g and VALUELISTOF FunctionDocument11 pagesCarpediemconsulting's Blog: Row Wise Initialized Variable in OBIEE 11g and VALUELISTOF FunctionChakri ReddyNo ratings yet
- AaryajananiDocument3 pagesAaryajananijananisasi68No ratings yet
- The Aeta People of The PhilippinesDocument11 pagesThe Aeta People of The PhilippinesaironjazzcasosolaNo ratings yet
- Brinas V People G.R. No. 254005Document9 pagesBrinas V People G.R. No. 254005weddanever.cornelNo ratings yet
- World Neuroscience Conference 2020 - BrochureDocument11 pagesWorld Neuroscience Conference 2020 - BrochureGrace LilyNo ratings yet
- Nonstationary Precipitation Intensity-Duration-Frequency Curves For Infrastructure Design in A Changing ClimateDocument6 pagesNonstationary Precipitation Intensity-Duration-Frequency Curves For Infrastructure Design in A Changing ClimateOfosu AnimNo ratings yet
- Composition and Oxidative Stability of Soybean Oil in Mixtures With Jojoba OilDocument8 pagesComposition and Oxidative Stability of Soybean Oil in Mixtures With Jojoba OilYonatan AdiNo ratings yet
- Abdelwahab Elmessiri - Secularism, Immanence, and DeconstructionDocument15 pagesAbdelwahab Elmessiri - Secularism, Immanence, and DeconstructionAfthab EllathNo ratings yet
- Previous Years UPSC Prelims Questions Medieval Indian History 2013 2020Document9 pagesPrevious Years UPSC Prelims Questions Medieval Indian History 2013 2020P B PatilNo ratings yet
- Case Study NAEYC Standard 4: Using Developmentally Effective ApproachesDocument6 pagesCase Study NAEYC Standard 4: Using Developmentally Effective Approachesapi-316131028No ratings yet
- (GeoJournal Library 103) Charlotta Hedberg, Renato Miguel do Carmo (auth.), Charlotta Hedberg, Renato Miguel do Carmo (eds.) - Translocal Ruralism_ Mobility and Connectivity in European Rural Spaces-S.pdfDocument235 pages(GeoJournal Library 103) Charlotta Hedberg, Renato Miguel do Carmo (auth.), Charlotta Hedberg, Renato Miguel do Carmo (eds.) - Translocal Ruralism_ Mobility and Connectivity in European Rural Spaces-S.pdffalmo123No ratings yet
- International Islamic University Malaysia End-Of-Semester Final Assessment SEMESTER 1, 2020/2021 SESSIONDocument15 pagesInternational Islamic University Malaysia End-Of-Semester Final Assessment SEMESTER 1, 2020/2021 SESSIONAli NajhanNo ratings yet
- Chapter 1-Introduction To Financial ManagementDocument15 pagesChapter 1-Introduction To Financial ManagementfatinfyNo ratings yet
- Three-Dimensional Conformal Radiation Therapy (3DCRT) For Prostate CancerDocument34 pagesThree-Dimensional Conformal Radiation Therapy (3DCRT) For Prostate CancerMuhammad Safwan Ahmad FadzilNo ratings yet
- NCP UgibDocument4 pagesNCP UgibErnest Brian FernandezNo ratings yet