You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Chapter 25 - Substantive Test of LiabilitiesDocument10 pagesChapter 25 - Substantive Test of LiabilitiesQuijano GpokskieNo ratings yet
- Points To PonderDocument9 pagesPoints To PonderQuijano GpokskieNo ratings yet
- Physiologic Changes in Aging Affecting Various Systems: Mrs. Joji B. Castellano, R.N.,ManDocument11 pagesPhysiologic Changes in Aging Affecting Various Systems: Mrs. Joji B. Castellano, R.N.,ManQuijano GpokskieNo ratings yet
- Good Moaning ?: Gem Eunice B, QuijanoDocument9 pagesGood Moaning ?: Gem Eunice B, QuijanoQuijano GpokskieNo ratings yet
- Unadjusted Book Balance (1.) 504,000 (2.) 735,000 (3.) 700,000 (4.) 539,000Document2 pagesUnadjusted Book Balance (1.) 504,000 (2.) 735,000 (3.) 700,000 (4.) 539,000Quijano GpokskieNo ratings yet
- Abraham Maslow'S Hierarchy of Basic Human NeedsDocument8 pagesAbraham Maslow'S Hierarchy of Basic Human NeedsQuijano GpokskieNo ratings yet
- Official Study Load Student'S Copy: Section Descriptive Title Days Time Lec Lab UnitsDocument1 pageOfficial Study Load Student'S Copy: Section Descriptive Title Days Time Lec Lab UnitsQuijano GpokskieNo ratings yet
- 3a Competency Assessment - Patient Controlled AnalgesiaDocument2 pages3a Competency Assessment - Patient Controlled AnalgesiaQuijano GpokskieNo ratings yet
- One True KingDocument5 pagesOne True KingQuijano GpokskieNo ratings yet
- ABCDE Assessment Exam: Eunice QuijanoDocument3 pagesABCDE Assessment Exam: Eunice QuijanoQuijano GpokskieNo ratings yet
- Operating and Delivery Room Cases: Data SheetDocument9 pagesOperating and Delivery Room Cases: Data SheetQuijano GpokskieNo ratings yet
- 2 Myocardial Infarction Nursing Care Management and Study GuideDocument13 pages2 Myocardial Infarction Nursing Care Management and Study GuideQuijano Gpokskie100% (2)
- 1 Pain AssessmentDocument13 pages1 Pain AssessmentQuijano GpokskieNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- TTTTDocument26 pagesTTTTMoataz TrabehNo ratings yet
- Angiotensin Converting Enzyme Inhibitors: Properties and Side EffectsDocument6 pagesAngiotensin Converting Enzyme Inhibitors: Properties and Side EffectselvishmicroNo ratings yet
- Guidelines TX of HPNDocument3 pagesGuidelines TX of HPNjheyfteeNo ratings yet
- Congestive Heart FailureDocument89 pagesCongestive Heart FailureMuhammad Mustafa Ijaz100% (3)
- Galappatthy2016 Article LegEdemaWithS-amlodipineVsConvDocument10 pagesGalappatthy2016 Article LegEdemaWithS-amlodipineVsConvPathiwat M ChantanaNo ratings yet
- Cenforce 100mgDocument2 pagesCenforce 100mgjean greyNo ratings yet
- Beta BlockersDocument70 pagesBeta BlockersIrina Cabac-PogoreviciNo ratings yet
- UkpdsDocument100 pagesUkpdsBeny Rilianto0% (1)
- Articulo COVID 19Document9 pagesArticulo COVID 19Omaira TovarNo ratings yet
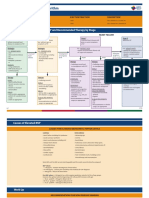
- Heart Failure Treatment Algorithm: Diagnosis and ClassificationDocument7 pagesHeart Failure Treatment Algorithm: Diagnosis and ClassificationLorreine Elisa FaruqNo ratings yet
- Bhagani 2018Document7 pagesBhagani 2018rifky kurniawanNo ratings yet
- Antihypertensive DrugsDocument62 pagesAntihypertensive DrugsYeshaa MiraniNo ratings yet
- 01-09 2022 Pharm Chronic Care in Cardiology 2022 R4Document62 pages01-09 2022 Pharm Chronic Care in Cardiology 2022 R4Amira HelayelNo ratings yet
- IRIS CAT Treatment Recommendations 2023Document17 pagesIRIS CAT Treatment Recommendations 2023Haniel MonteiroNo ratings yet
- ACE InhibitorsDocument26 pagesACE Inhibitorsali mohammedNo ratings yet
- Case Study: A Patient With Type 2 Diabetes Working With An Advanced Practice Pharmacist To Address Interacting ComorbiditiesDocument8 pagesCase Study: A Patient With Type 2 Diabetes Working With An Advanced Practice Pharmacist To Address Interacting ComorbiditiessamanNo ratings yet
- Cardiology Handbook Gondar University Hospital: Management GuidelinesDocument42 pagesCardiology Handbook Gondar University Hospital: Management Guidelinessky nutsNo ratings yet
- Leite de Ovelha - TrabalhoDocument30 pagesLeite de Ovelha - Trabalhodorde1234No ratings yet
- Pharma Compre SamplexDocument19 pagesPharma Compre SamplexStephanie BragatNo ratings yet
- MS 16Document7 pagesMS 16Ferdinand TerceroNo ratings yet
- Hypertensive Emergency PDFDocument14 pagesHypertensive Emergency PDFOsiithaa CañaszNo ratings yet
- Hyperkalemia: Dr. K. K. Gupta Associate Prof. Department of Medicine, KgmuDocument23 pagesHyperkalemia: Dr. K. K. Gupta Associate Prof. Department of Medicine, KgmuPrass Ekasetia PoetraNo ratings yet
- Cardiovascular Drugs: Dr. April Dawn R. LuceroDocument122 pagesCardiovascular Drugs: Dr. April Dawn R. LuceroRjDNo ratings yet
- Heartfailure Management in PlabDocument7 pagesHeartfailure Management in PlabShimmering MoonNo ratings yet
- Acute Renal FailureDocument14 pagesAcute Renal FailuredrtpkNo ratings yet
- Hypertension: Dr. Lucia Mazur-Nicorici Md. PHDDocument34 pagesHypertension: Dr. Lucia Mazur-Nicorici Md. PHDValerianBîcosNo ratings yet
- Heart Failure: Zelalem T., MD Yr III Resident, PediatricsDocument65 pagesHeart Failure: Zelalem T., MD Yr III Resident, PediatricsChalie MequanentNo ratings yet
- Drug Interactions-Principles Examples and ClinicalDocument13 pagesDrug Interactions-Principles Examples and ClinicalRaudhatul JannahNo ratings yet
- Hypertensive Crisis: Instructor'S Guide To Changes in This EditionDocument6 pagesHypertensive Crisis: Instructor'S Guide To Changes in This Editionnurmaliarizky100% (1)
- ACE InhibitorsDocument2 pagesACE InhibitorsJosephine Irena100% (1)