You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5808)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (843)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Preppers Medical Handbook by William ForgeyDocument321 pagesThe Preppers Medical Handbook by William ForgeyAtiwat Tre100% (6)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Pain Assessment in Advanced Dementia (PAINAD) ScaleDocument2 pagesPain Assessment in Advanced Dementia (PAINAD) ScaleRSMKBT100% (1)
- Library of Teachings - The Magnificent Nine - ©the-Teachings-Of-Yogi-Bhajan PDFDocument5 pagesLibrary of Teachings - The Magnificent Nine - ©the-Teachings-Of-Yogi-Bhajan PDFOlympia100% (1)
- Spring Forest QigongDocument14 pagesSpring Forest QigongTomV77100% (3)
- Solution: Using Newton Raphson Method:: Relative HumidityDocument5 pagesSolution: Using Newton Raphson Method:: Relative Humidityhazem ab2009No ratings yet
- Word Final Exam - TextDocument3 pagesWord Final Exam - Texthazem ab2009No ratings yet
- Chapter - 7 in ClassDocument6 pagesChapter - 7 in Classhazem ab2009No ratings yet
- Ray Obtics PhysicsDocument150 pagesRay Obtics Physicshazem ab2009No ratings yet
- بيزDocument6 pagesبيزhazem ab2009No ratings yet
- Section 2 Lab 3 Ph102 HDocument12 pagesSection 2 Lab 3 Ph102 Hhazem ab2009No ratings yet
- FeedbackDocument39 pagesFeedbackhazem ab2009No ratings yet
- EGR 101 - Materials Science For Engineering Applications: Teacher/Examiner: Dr. Shriram DuraisamyDocument21 pagesEGR 101 - Materials Science For Engineering Applications: Teacher/Examiner: Dr. Shriram Duraisamyhazem ab2009No ratings yet
- An Atlas of Engineering Dynamic Systems, Models, and Transfer FunctionsDocument37 pagesAn Atlas of Engineering Dynamic Systems, Models, and Transfer Functionshazem ab2009No ratings yet
- ENGR132 Spring22 Course Project NewDocument19 pagesENGR132 Spring22 Course Project Newhazem ab2009No ratings yet
- CHE320 Sp22 Assessment 2 F3Document3 pagesCHE320 Sp22 Assessment 2 F3hazem ab2009No ratings yet
- Electro-Motion Devices: Lecture 4-Magnetic CircuitsDocument76 pagesElectro-Motion Devices: Lecture 4-Magnetic Circuitshazem ab2009No ratings yet
- Scaled Control Performance Benchmarks and Maneuvers For Small-Scale Unmanned HelicoptersDocument9 pagesScaled Control Performance Benchmarks and Maneuvers For Small-Scale Unmanned Helicoptershazem ab2009No ratings yet
- Topic 3Document34 pagesTopic 3hazem ab2009No ratings yet
- AhmetFatihTabak ME BSC ThesisDocument120 pagesAhmetFatihTabak ME BSC Thesishazem ab2009No ratings yet
- Design Implementation and Control of ScaDocument92 pagesDesign Implementation and Control of Scahazem ab2009No ratings yet
- MA166 Analytic Geometry and Calculus IIDocument30 pagesMA166 Analytic Geometry and Calculus IIhazem ab2009No ratings yet
- Series Ap Directly Operated Proportional Valves: Use and Maintenance ManualDocument16 pagesSeries Ap Directly Operated Proportional Valves: Use and Maintenance Manualhazem ab2009No ratings yet
- Sound and Light PDFDocument23 pagesSound and Light PDFhazem ab2009100% (1)
- 4mesic 2003 PDFDocument13 pages4mesic 2003 PDFhazem ab2009No ratings yet
- Basic Life Support Field GuideDocument56 pagesBasic Life Support Field GuidelmaoheartsNo ratings yet
- Self FlowDocument15 pagesSelf FlowariNo ratings yet
- BioPak 240RDocument19 pagesBioPak 240RForum PompieriiNo ratings yet
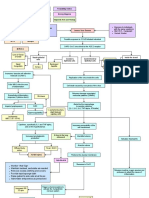
- Predisposing Factors Disease Precipitating Factors: LegendDocument3 pagesPredisposing Factors Disease Precipitating Factors: LegendSOPHIA LOISE TEJANO FULACHENo ratings yet
- The Vampire Codex: Michelle BelangerDocument40 pagesThe Vampire Codex: Michelle Belangertramar725No ratings yet
- Gun Safety Seminar Ver2Document49 pagesGun Safety Seminar Ver2nazh100% (7)
- 2022 PPT Bio K1Document20 pages2022 PPT Bio K1SITI ZAHILA ARYANIE BINTI ABD RAHIM KPM-GuruNo ratings yet
- Yogavani February 2024 3Document33 pagesYogavani February 2024 3MrPpatel100No ratings yet
- Fundamentals of NursingDocument16 pagesFundamentals of NursingFreeNursingNotes85% (26)
- Pressure Regulator FRN Zero Pressure RegulatorDocument4 pagesPressure Regulator FRN Zero Pressure RegulatorImran Ahmed KhanNo ratings yet
- Yoga Daily PracticeDocument11 pagesYoga Daily Practiceanislimit100% (1)
- COPD Case StudyDocument3 pagesCOPD Case Studyshazel chiasaokwuNo ratings yet
- Laporan Praktikum Fishew RespirasiDocument9 pagesLaporan Praktikum Fishew RespirasiputriajengsNo ratings yet
- Midterm Last TopicDocument3 pagesMidterm Last TopicLynette BalodNo ratings yet
- First Aid and CPR NotesDocument19 pagesFirst Aid and CPR NotesShaheer AsifNo ratings yet
- Nursing Care Plan: Assessment Diagnosis Planning Interventions Rationale EvaluationDocument2 pagesNursing Care Plan: Assessment Diagnosis Planning Interventions Rationale EvaluationMina SumaoangNo ratings yet
- P30 SystemDocument5 pagesP30 Systemfdpc1987No ratings yet
- 2ND Quarter Test Questions Els - 40Document4 pages2ND Quarter Test Questions Els - 40Very VaneNo ratings yet
- Nursing Diagnosis Common Health Problems That Develop During InfamcyDocument5 pagesNursing Diagnosis Common Health Problems That Develop During InfamcyNur SanaaniNo ratings yet
- Nytro Izar I Se en SdsDocument31 pagesNytro Izar I Se en SdsFredNo ratings yet
- AS3000 Service ManualDocument180 pagesAS3000 Service ManualRaul PerezNo ratings yet
- Grounding Technique 2Document2 pagesGrounding Technique 2gagan-sidhu-35No ratings yet
- Surface Supply Requirements October 29 2019Document34 pagesSurface Supply Requirements October 29 2019joaquin valenzuelaNo ratings yet
- Krok Review: How To Prepare Krok TestDocument84 pagesKrok Review: How To Prepare Krok Testgaurav100% (2)
- Nursing Care Plan For Client With Lung Cancer 1. DefinitionDocument9 pagesNursing Care Plan For Client With Lung Cancer 1. DefinitionMuslih FerecovNo ratings yet
- Cech and Brauner 2011 Encyclopedia of Fish Physiol Techniques in Respiratory Physiology!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!Document8 pagesCech and Brauner 2011 Encyclopedia of Fish Physiol Techniques in Respiratory Physiology!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!daniel cretuNo ratings yet