You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- CJASN 2006 Jul 1 (4) 641-54, Figure 1Document1 pageCJASN 2006 Jul 1 (4) 641-54, Figure 1Ethar LoveNo ratings yet
- Tomich Fetal Heart Rate Monitoring772014Document69 pagesTomich Fetal Heart Rate Monitoring772014Ethar LoveNo ratings yet
- Git PDFDocument106 pagesGit PDFEthar LoveNo ratings yet
- Diuretics: How Do They Work?Document13 pagesDiuretics: How Do They Work?Ethar LoveNo ratings yet
- Adrenergic AgonistsDocument22 pagesAdrenergic AgonistsEthar LoveNo ratings yet
- Syphilis2014 2Document62 pagesSyphilis2014 2Ethar LoveNo ratings yet
- Risk & Causation: Frances Aviles MD MPH BsDocument47 pagesRisk & Causation: Frances Aviles MD MPH BsEthar LoveNo ratings yet
- Pharmacology DiscussionDocument13 pagesPharmacology DiscussionEthar LoveNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Pathophysiology of StrokeDocument2 pagesPathophysiology of StrokeACe JAy100% (2)
- Module 18 Respiratory FinalDocument15 pagesModule 18 Respiratory FinalJayR MendonesNo ratings yet
- Catheter Ablation For Atrial Fibrillation: Original ArticleDocument7 pagesCatheter Ablation For Atrial Fibrillation: Original ArticleGavin WinkelNo ratings yet
- The Physiology of Ageing: Key PointsDocument5 pagesThe Physiology of Ageing: Key PointsArmani Gontijo Plácido Di AraújoNo ratings yet
- Tetralogy of Fallot: R. Wilson, O. Ross and M.J. GriksaitisDocument8 pagesTetralogy of Fallot: R. Wilson, O. Ross and M.J. Griksaitiscomiza92No ratings yet
- Chlorophyll and Other Pigments: Week 7Document15 pagesChlorophyll and Other Pigments: Week 7Rheanet UbidoNo ratings yet
- Test 3Document9 pagesTest 3jec9229No ratings yet
- Circadian Rhythm NotesDocument2 pagesCircadian Rhythm NotesTiffany ZenhoihsangNo ratings yet
- Autonomic Nervous System - Basic and Clinical AspectsDocument393 pagesAutonomic Nervous System - Basic and Clinical AspectsGrossl Schorr Fernando100% (1)
- Geriatri EndodontikDocument4 pagesGeriatri EndodontikMeidi KurniaNo ratings yet
- Animal Simulator BrochureDocument3 pagesAnimal Simulator BrochureSuhas SakarkarNo ratings yet
- 5ОМ англ ВОП 1Document22 pages5ОМ англ ВОП 1p69b24hy8pNo ratings yet
- TwoProcessModel PPSChapter BorbleyDocument16 pagesTwoProcessModel PPSChapter Borbleysuresh2250No ratings yet
- Parts of A Neuron: 1. Dendrites 2. Cell Body With Nucleus 3. Axon 4. Synaptic TerminalDocument3 pagesParts of A Neuron: 1. Dendrites 2. Cell Body With Nucleus 3. Axon 4. Synaptic TerminalDonald KingNo ratings yet
- 327616blood Flow Restriction (BFR) Training - Sports Medicine Center ...Document2 pages327616blood Flow Restriction (BFR) Training - Sports Medicine Center ...tyrelawlknNo ratings yet
- Diagnosing Secondary Headaches (Practical Neurology) (2020 - 05)Document5 pagesDiagnosing Secondary Headaches (Practical Neurology) (2020 - 05)Apostolos T.No ratings yet
- SAAOL Medicine With Mech. of ActionDocument58 pagesSAAOL Medicine With Mech. of ActionSusanta RoutNo ratings yet
- 2020 - A Physiologic Approach To Hemodynamic Monitoring and Optimizing Oxygen Delivery in Shock ResuscitationDocument18 pages2020 - A Physiologic Approach To Hemodynamic Monitoring and Optimizing Oxygen Delivery in Shock ResuscitationAndre OliveiraNo ratings yet
- The Relation of Grades 9 and 10 Students' Sleeping Patterns and Their Attendance in Saint Francis of Assisi College Main CampusDocument15 pagesThe Relation of Grades 9 and 10 Students' Sleeping Patterns and Their Attendance in Saint Francis of Assisi College Main CampusJesary Marc ArnosaNo ratings yet
- STEMI Care Reperfusions Trategy - DR Eka GinanjarDocument39 pagesSTEMI Care Reperfusions Trategy - DR Eka GinanjarIra MashadiNo ratings yet
- Body Temperature - QuestionsDocument6 pagesBody Temperature - QuestionsErjus Hoxhaj50% (2)
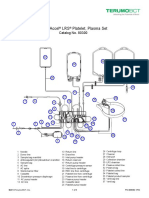
- Trima Accel LRS Platelet, Plasma Set: Catalog No. 80300Document10 pagesTrima Accel LRS Platelet, Plasma Set: Catalog No. 80300Suneo HonekawaNo ratings yet
- Blood Flow Mechanics (Medicalstudyzone - Com)Document31 pagesBlood Flow Mechanics (Medicalstudyzone - Com)Lordoc DoctorsaabNo ratings yet
- Anabolic Sleeping 1Document53 pagesAnabolic Sleeping 1DavidBrionesBetanzoNo ratings yet
- Biology Assignment 2 Atefah Razack 1Document15 pagesBiology Assignment 2 Atefah Razack 1api-491258706No ratings yet
- Electron Transport ChainDocument11 pagesElectron Transport ChainSoofia SharifNo ratings yet
- Worksheet FormsDocument5 pagesWorksheet FormsedoyNo ratings yet
- Health Assessment Form - BHERTDocument2 pagesHealth Assessment Form - BHERTPoblacion 04 San LuisNo ratings yet
- Acute Kidney Injury: Lantin/Reyes/Sanchez/SevillaDocument32 pagesAcute Kidney Injury: Lantin/Reyes/Sanchez/SevillaKen Edward ZataNo ratings yet
- Circulatory SystemDocument3 pagesCirculatory Systemapi-521781723No ratings yet