You might also like
- 2021-06-01-COVID-19-Algo-ver-4.0 2Document53 pages2021-06-01-COVID-19-Algo-ver-4.0 2Rye CalderonNo ratings yet
- COVID-19 MoHP Protocol May 2020Document14 pagesCOVID-19 MoHP Protocol May 2020BARAKA ROKANo ratings yet
- Covid 19 PathwayDocument17 pagesCovid 19 Pathwayferi adiantoNo ratings yet
- Covid y CorazonDocument19 pagesCovid y CorazonSMIBA MedicinaNo ratings yet
- Alvarado Score For Acute Appendicitis Alvarado Score For Acute AppendicitisDocument2 pagesAlvarado Score For Acute Appendicitis Alvarado Score For Acute AppendicitisrulisakaroziNo ratings yet
- Updates On COVID 19 (19032020, V1) PDFDocument32 pagesUpdates On COVID 19 (19032020, V1) PDFroserosannaNo ratings yet
- Nursing Interventions Ii (N109/N124)Document12 pagesNursing Interventions Ii (N109/N124)Trisha Rimando ÜNo ratings yet
- PSMID Guidelines COVID 19 - EditedDocument8 pagesPSMID Guidelines COVID 19 - EditedIsrael H. ZantuaNo ratings yet
- Community Acquired PneumoniaDocument5 pagesCommunity Acquired PneumoniaJerrica Charlene GalopeNo ratings yet
- Rheumatic Fever PDFDocument3 pagesRheumatic Fever PDFDoc JT BylnNo ratings yet
- Infection, Genetics and Evolution: Research PaperDocument5 pagesInfection, Genetics and Evolution: Research PaperAhmad Afianto MuttolibNo ratings yet
- Questions Choices: Part I: Demographic Characteristics of The ParticipantsDocument4 pagesQuestions Choices: Part I: Demographic Characteristics of The ParticipantsCHLOIE MARIE ROSALEJOSNo ratings yet
- PEDIA-Pneumonia Part II (Dr. Bermejo)Document4 pagesPEDIA-Pneumonia Part II (Dr. Bermejo)Monique BorresNo ratings yet
- Covid Antiviral Medications How To Prescribe Mar 10 2022Document38 pagesCovid Antiviral Medications How To Prescribe Mar 10 2022ABDULLAH SDNo ratings yet
- Case Report 4 - 2013Document5 pagesCase Report 4 - 2013Nguyen Trong PhuocNo ratings yet
- TRD, ND: HtlkrlirrtDocument1 pageTRD, ND: HtlkrlirrtSURESH456789123 111No ratings yet
- Barnet Primary Care Pathway During Covid19 v1 PDFDocument1 pageBarnet Primary Care Pathway During Covid19 v1 PDFAndrew WilkinsonNo ratings yet
- Junio Covid-19 - Sanford GuideDocument8 pagesJunio Covid-19 - Sanford GuideEfraín Castilla MinayaNo ratings yet
- Sanford Guide COVID ManagementDocument10 pagesSanford Guide COVID ManagementAnonymous FCOOcnNo ratings yet
- Pedia COVID POLICIES 2023Document9 pagesPedia COVID POLICIES 2023Katrina Kristine RamosNo ratings yet
- CDC Modernapfizer EmailsDocument1,433 pagesCDC Modernapfizer EmailsZerohedge JanitorNo ratings yet
- Bu Yovita Penanganan Medis Infeksi nCoV 05022020Document18 pagesBu Yovita Penanganan Medis Infeksi nCoV 05022020restulibrianiNo ratings yet
- Jgs 16728 PDFDocument5 pagesJgs 16728 PDFNereida LmtzNo ratings yet
- UK Biologics Checklist May 2014Document2 pagesUK Biologics Checklist May 2014Dr Sneha's Skin and Allergy Clinic IndiaNo ratings yet
- Decision Algorithms For The Telehome Care Management of Asymptomatic or Mildly Symptomatic COVID - 19 PatientsDocument12 pagesDecision Algorithms For The Telehome Care Management of Asymptomatic or Mildly Symptomatic COVID - 19 PatientsPatricia Franco-VillaNo ratings yet
- Management of Mild Cases of COVID-19 in Low-Resource CountriesDocument2 pagesManagement of Mild Cases of COVID-19 in Low-Resource CountriesAnthony HopkinsNo ratings yet
- Tatalaksana Kasus (13022020)Document31 pagesTatalaksana Kasus (13022020)junai arandetaNo ratings yet
- COVID-19 Alvin RinaldoDocument21 pagesCOVID-19 Alvin RinaldoAlvin RinaldoNo ratings yet
- nCoV Algorithm-ManagementDocument1 pagenCoV Algorithm-ManagementyoelpadronNo ratings yet
- Covid For ClerksDocument60 pagesCovid For ClerksNehemiah FranciscoNo ratings yet
- Coronavirus19 1Document60 pagesCoronavirus19 1bekbekk cabahugNo ratings yet
- MoHP Protocol For COVID19 November 2020Document28 pagesMoHP Protocol For COVID19 November 2020medya dostorNo ratings yet
- Bsn-Rs-Careplan 3-2Document12 pagesBsn-Rs-Careplan 3-2api-509646698No ratings yet
- Visual Triage FormDocument1 pageVisual Triage FormtardecilladianaNo ratings yet
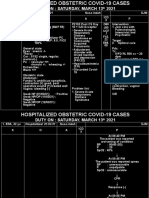
- Duty On: Saturday, March 13 2021: +severe AcuteDocument2 pagesDuty On: Saturday, March 13 2021: +severe AcuteJananuraga MaharddhikaNo ratings yet
- (IM2) 6.6 Sepsis & Septic Shock - DR - ChunguncoDocument13 pages(IM2) 6.6 Sepsis & Septic Shock - DR - ChunguncoMaria Gracia Yamson100% (1)
- Syncope: DR - Hardja Priatna, SPJP, Fiha 26 Februari 2018Document77 pagesSyncope: DR - Hardja Priatna, SPJP, Fiha 26 Februari 2018pkm cibodasariNo ratings yet
- Aden Covid-19 Protocol 26-5-2020 (ASIA) 22-1Document14 pagesAden Covid-19 Protocol 26-5-2020 (ASIA) 22-1محمدرزازالتبعيNo ratings yet
- Update On Clinical Management - PrivateDocument57 pagesUpdate On Clinical Management - PrivateJashveerBediNo ratings yet
- Status Klinis COVID-19 Kombinasi Dengan Penyakit KardiovaskularDocument21 pagesStatus Klinis COVID-19 Kombinasi Dengan Penyakit KardiovaskularMariaAmeliaGoldieNo ratings yet
- DR Anggraeni RSHS PPI EditDocument36 pagesDR Anggraeni RSHS PPI EditdinarNo ratings yet
- Covid HypertensionDocument9 pagesCovid HypertensionFemma ElizabethNo ratings yet
- Association of Hypertension andDocument9 pagesAssociation of Hypertension andDeny Dwi HartantoNo ratings yet
- Morning Report 23-01-18Document36 pagesMorning Report 23-01-18Yohanes FirmansyahNo ratings yet
- Updated - COVID TX Algorithm - July 15Document4 pagesUpdated - COVID TX Algorithm - July 15Krim GalanNo ratings yet
- Surveillance System in The PhilippinesDocument38 pagesSurveillance System in The PhilippinesFred C. MirandaNo ratings yet
- PHEM ReportDocument2 pagesPHEM ReportmekuriaNo ratings yet
- Sample Case Studies of COVID-19 in PregnancyDocument29 pagesSample Case Studies of COVID-19 in PregnancyAbdibaset Mohamed AdenNo ratings yet
- Ruchi: InterpretationDocument2 pagesRuchi: InterpretationKuldeep KumarNo ratings yet
- AIARDocument3 pagesAIARABHISHEK SINGHNo ratings yet
- Management Protocol Covid 19 V08 21-7-2020Document1 pageManagement Protocol Covid 19 V08 21-7-2020EdgarNo ratings yet
- PJR BF02723652Document2 pagesPJR BF02723652lenirizkiNo ratings yet
- Tarun Kumar Report - 15012022 - 120821Document1 pageTarun Kumar Report - 15012022 - 120821navdeep madheshiyaNo ratings yet
- COVID Latest GuidelinesDocument48 pagesCOVID Latest Guidelinesarrestedinlove123No ratings yet
- Released: Sunpower Philippines Medical Screening Form (MSF)Document2 pagesReleased: Sunpower Philippines Medical Screening Form (MSF)glenn dalesNo ratings yet
- PREOPinguinalherniaDocument2 pagesPREOPinguinalherniapatriciaatan1497No ratings yet
- SE05Document3 pagesSE05Yash PratapNo ratings yet
- Emerging Covid19 Neurology Affections. 8jul20 Supplementary-DataDocument26 pagesEmerging Covid19 Neurology Affections. 8jul20 Supplementary-DataRohan KhooshiNo ratings yet
- Radiologi 3Document5 pagesRadiologi 3Sarah watiNo ratings yet
- Chronic Inflammatory Demyelinating PolyneuropathyDocument36 pagesChronic Inflammatory Demyelinating PolyneuropathySafitri MuhlisaNo ratings yet
- Gastroenterology PT MRCP I 2019 2nd Edition PDF HXP DR NotesDocument1,142 pagesGastroenterology PT MRCP I 2019 2nd Edition PDF HXP DR NotesRami NaousNo ratings yet
- What Are The Possible Causes of DyspneaDocument9 pagesWhat Are The Possible Causes of DyspneaHanis Afiqah Violet MeowNo ratings yet
- Dr. S.K. Haldar's Lectures On Industrial Health For AFIH Students - PesticidesDocument3 pagesDr. S.K. Haldar's Lectures On Industrial Health For AFIH Students - PesticidesDr. Prakash KulkarniNo ratings yet
- Alice in Wonderland SyndromeDocument4 pagesAlice in Wonderland SyndromeDoraNo ratings yet
- The Borax Conspiracy The End of The Osteoarthritis CureDocument15 pagesThe Borax Conspiracy The End of The Osteoarthritis Cureneptu88100% (1)
- Antihyperlipidemic AgentsDocument79 pagesAntihyperlipidemic AgentsKishori Kedia100% (1)
- Makshika Visha - The Concepts of Honey Bee Envenomation in AyurvedaDocument6 pagesMakshika Visha - The Concepts of Honey Bee Envenomation in AyurvedaAdvanced Research PublicationsNo ratings yet
- AfflictionsDocument12 pagesAfflictionsshiraaazNo ratings yet
- Post-Traumatic Stress DisorderDocument12 pagesPost-Traumatic Stress Disorderecbt100% (2)
- A Beautiful Mind PsychologyDocument4 pagesA Beautiful Mind Psychologysunny peoupangNo ratings yet
- Edible Vaccines: Promises and Challenges: Vrinda M Kurup Jaya ThomasDocument12 pagesEdible Vaccines: Promises and Challenges: Vrinda M Kurup Jaya ThomasBelaNo ratings yet
- Palliative Care - Overview of Cough, Stridor, and Hemoptysis - UpToDateDocument19 pagesPalliative Care - Overview of Cough, Stridor, and Hemoptysis - UpToDateThaísa NogueiraNo ratings yet
- Dozois 5e Chapter01 TIFDocument32 pagesDozois 5e Chapter01 TIFrebeccaNo ratings yet
- Iccu / Cicu: Patients Heart Attacks Unstable Angina Cardiac DysrhythmiaDocument4 pagesIccu / Cicu: Patients Heart Attacks Unstable Angina Cardiac DysrhythmiaAlya Putri KhairaniNo ratings yet
- Elios Omœopathy: AB G T HDocument28 pagesElios Omœopathy: AB G T HAlberto Garcia100% (8)
- Isolation of Lactobacillus AcidophilusDocument4 pagesIsolation of Lactobacillus AcidophilusIqra MustafaNo ratings yet
- Introduction To Behavioral Medicine For Mental Health CounselorsDocument28 pagesIntroduction To Behavioral Medicine For Mental Health CounselorsDeva ChiruNo ratings yet
- Iaso Tea IngredientDocument7 pagesIaso Tea Ingredientsizzla7No ratings yet
- What Is MrsaDocument17 pagesWhat Is MrsaAnonymous NVBCqKWHNo ratings yet
- Gram Negative RodsDocument23 pagesGram Negative RodsYasir KareemNo ratings yet
- Calcium Channel Blockers in Antihypertensive Treatment The Role of LecardipineDocument35 pagesCalcium Channel Blockers in Antihypertensive Treatment The Role of LecardipineAndi WirawanNo ratings yet
- Ok Sa Deped Form B - For SchoolsDocument5 pagesOk Sa Deped Form B - For SchoolsAna Cella Rico MarzoNo ratings yet
- Special Operations Forces Nutrition GuideDocument225 pagesSpecial Operations Forces Nutrition GuideNick Vanb100% (2)
- Cefuroxime 1Document3 pagesCefuroxime 1Gwyn RosalesNo ratings yet
- Inclusiveness Students' Short Note in 2012 E.C.Document62 pagesInclusiveness Students' Short Note in 2012 E.C.Mitiku Abebe100% (1)
- 13 IMPLANT SUPPORTED FIXED PROSTHESESmic PDFDocument52 pages13 IMPLANT SUPPORTED FIXED PROSTHESESmic PDFManaila GeorgianNo ratings yet
- Pasar Rbe CutieDocument11 pagesPasar Rbe CutieElla RetizaNo ratings yet
- SD Bioline Salmonella Typhi Igg Igm FastDocument1 pageSD Bioline Salmonella Typhi Igg Igm FastLabor KaruniaNo ratings yet